Article Text

Statistics from Altmetric.com
The major cause of pediatric anterior urethral injuries (AUIs) is blunt trauma.1 2 Penetrating injuries caused by explosive trauma are rare in pediatric patients. Both early and delayed urethral repairs are optional strategies to manage AUIs. Studies from clinical management of blunt trauma have concluded rich experiences. However, poor experiences can be used to manage explosive AUIs. In this case, a 7-year-old boy threw a detonator into the fire. His external genitalia and bilateral medial region of the thigh were injured in a sudden explosion. Corpus spongiosum penis was covered by incomplete prepuce. Splintered glans penis with high-degree edema concealed the urethral meatus. The swollen testis was detected in the tattered scrotum. Muscular layer was included in explosive injuries of the bilateral thigh (figure 1). Surgical debridement was performed urgently. It was difficult to identify the external urethral orifice in the seriously damaged penis with progressive edema. Cystoscopy and urethral catheter insertion were abandoned. Open suprapubic cystostomy was performed. On day 5, reduced edema of the impaired penis made it possible to identify urethral meatus. Application of cystoscopy discovered a small laceration of the urethral meatus. The posterior urethra and neck of the bladder were normal. Simple urethral closure was done to repair the laceration and a urinary catheter was installed. The residual defect of the prepuce was repaired by the scrotal septum free graft urethroplasty, and urinary diversion ended on day 12 (figure 2). Application of urgent suprapubic diversion then delayed exploration and repair at the fifth day of AUI reduced the risk of urethral trauma-related complications. No urinary fistula or urethral trauma-related complications were observed within 1 year of follow-up. Pediatric blast AUIs lead to serious tissue damages and high-degree edema. Urgent urethral exploration may increase the risk of secondary injuries. Urine diversion is a priority step for early management. Swelling degradation of the injured urethra is a better timing resolution.
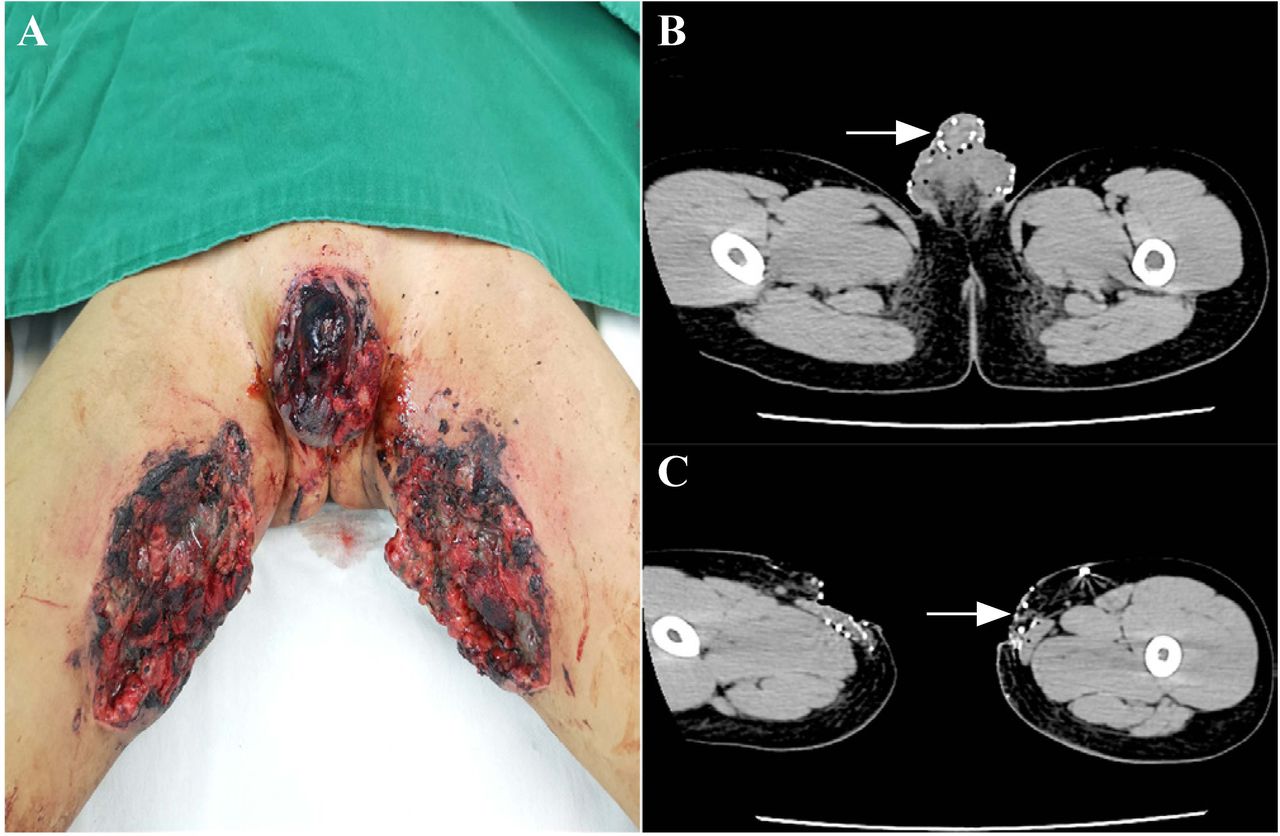
Injured region and films of CT scan taken on day 1 of a boy with a diagnosis of genital blast injury. (A) Incomplete coverage of prepuce, swollen testis, tattered scrotum and opening injury deep to the muscular layer of the medial region at the bilateral thigh. (B) Scattered metal fragments in the body of the penis, testis and scrotum (white arrow). (C) Defects of soft tissue deep to the muscular layer and scattered metal fragments in the medial region of the bilateral thigh (white arrow).
{kind=link}
{kind=link}
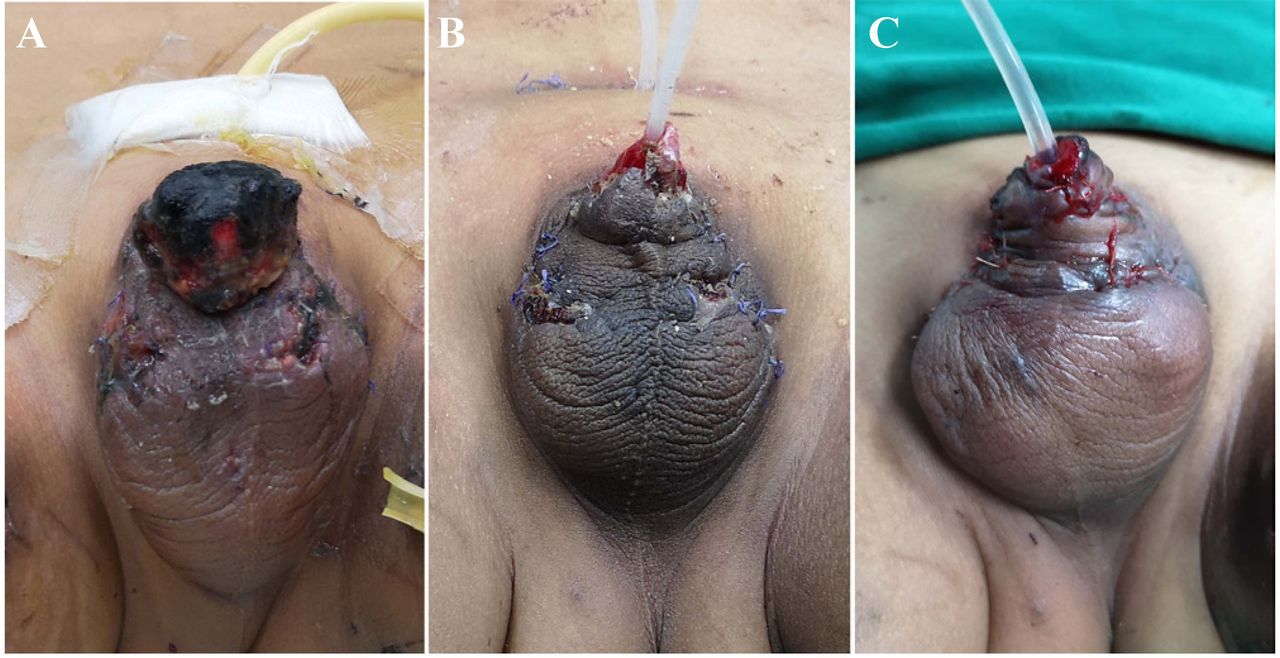
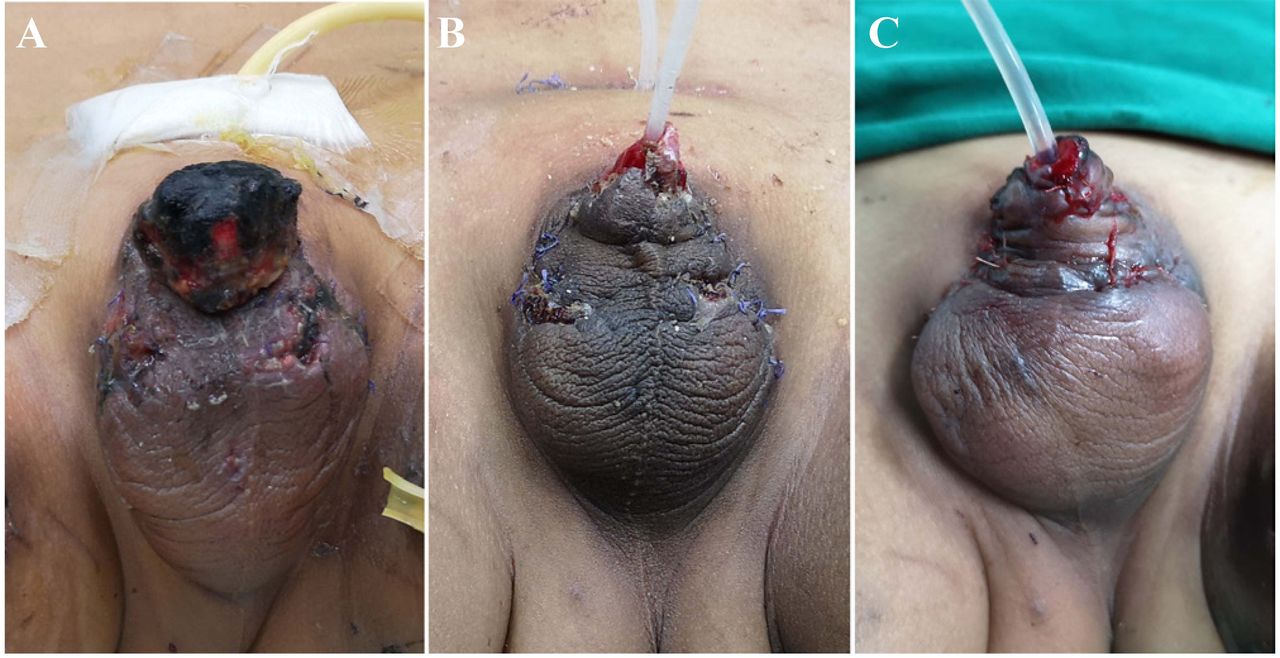
Repair and reconstruction of the external genitalia in a series of plastic operations. (A) Impaired penis with the coverage of black crust and reduced edema in the genital region on day 5 after the primary implementation of debridement. (B) Large prepuce and the cavernous body of penis defects on day 12 after the placement of the urinary canal and clearance of necrotic tissues. (C) Scrotal skin flap covering the rest of the cavernous body on day 17.
Footnotes
Contributors WN read the related literature, reviewed the patient’s medical records, collected the documentary of medical imaging, wrote the draft of the manuscript and was involved in the critical revision of the paper. CY completed patient’s follow-up. WXD reviewed the clinical picture of the patient. LXD provided the imaging films. All authors contained in the present work approved the final version.
Funding The authors received financial support from the Yunnan Provincial Department of Education (2019J0780).
Competing interests None declared.
Patient consent for publication The patient’s mother gave her consent for all material on the medical record, images and any other information about the patient to be published in a medical journal.
Ethics approval The study obeys medical ethics standards and was subjected to approved by our Medical Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available. Deidentified participant data.