MTHFR Gene Polymorphisms Prevalence and Cardiovascular Risk Factors Involved in Cardioembolic Stroke Type and Severity

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Clinical and Biochemical Evaluation
2.3. Evaluation of Stroke Severity
2.4. Imagistic Evaluation
2.5. Genetic Testing of MTHFR (C677T and A1298C) Polymorphisms
2.6. Ultrasound Evaluation of the Heart and Carotid Arteries
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Donkor, E.S. Stroke in the21stCentury: A snapshot of the burden, epidemiology, and quality of life. Stroke Res. Treat. 2018, 2018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yiin, G.S.C.; Howard, D.P.J.; Paul, N.L.M.; Li, L.; Luengo-Fernandez, R.; Bull, L.M.; Welch, S.J.V.; Gutnikov, S.A.; Mehta, Z.; Rothwell, P.M. Age-specific incidence, outcome, cost, and projected future burden of atrial fibrillation related embolic vascular events. Circulation 2014, 130, 1236–1244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Le, T.Q.H.; Nguyen, V.T.; Nguyen, T.K.; Phan, H.T. 1162: Echocardiography and cardioembolic stroke. Ultrasound Med. Boil. 2009, 35, S143. [Google Scholar] [CrossRef]
- Arboix, A.; Alió, J. Cardioembolic stroke: Clinical features, specific cardiac disorders and prognosis. Curr. Cardiol. Rev. 2010, 6, 150–161. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.O.; Park, H.S.; Ryu, C.S.; Shin, J.-W.; Kim, J.; Oh, S.H.; Kim, O.J.; Kim, N.K. Interplay between 3′-UTR polymorphisms in the methylenetetrahydrofolate reductase (MTHFR) gene and the risk of ischemic stroke. Sci. Rep. 2017, 7, 12464. [Google Scholar] [CrossRef] [Green Version]
- Kamel, H.; Okin, P.M.; Elkind, M.S.; Iadecola, C. Atrial fibrillation and mechanisms of stroke: Time for a new model. Stroke 2016, 47, 895–900. [Google Scholar] [CrossRef] [Green Version]
- Alkhouli, M.; Noseworthy, P.A.; Rihal, C.S.; Holmes, D.R. Stroke prevention in nonvalvular atrial fibrillation. J. Am. Coll. Cardiol. 2018, 71, 2790–2801. [Google Scholar] [CrossRef]
- Kelly, P.J.; Rosand, J.; Kistler, J.P.; Shih, V.E.; Silveira, S.; Plomaritoglou, A.; Furie, K.L. Homocysteine, MTHFR 677C→T polymorphism, and risk of ischemic stroke. Results of a meta-analysis. Neurology 2002, 59, 529–536. [Google Scholar] [CrossRef]
- Casas, J.P.; Bautista, L.E.; Smeeth, L.; Sharma, P.; Hingorani, A.D. Homocysteine and stroke: Evidence on a causal link from mendelian randomisation. Lancet 2005, 365, 224–232. [Google Scholar] [CrossRef]
- Jiang, S.; Zhao, R.; Pan, M.; Venners, S.A.; Zhong, G.; Hsu, Y.-H. Associations of MTHFR and MTRR Polymorphisms with Serum Lipid levels in Chinese Hypertensive Patients. Clin. Appl. Thromb. 2012, 20, 400–410. [Google Scholar] [CrossRef] [Green Version]
- Kotlęga, D.; Gołąb-Janowska, M.; Masztalewicz, M.; Ciećwież, S.; Nowacki, P. Association between selected gene polymorphisms and statin metabolism, risk of ischemic stroke and cardiovascular disorders. Postępy Higieny Medycyny Doświadczalnej 2016, 70, 435–447. [Google Scholar] [CrossRef] [PubMed]
- Mulder, A.B.; Van Lijf, H.J.; Bon, M.A.; Bergh, F.A.V.D.; Touw, D.; Neef, C.; Vermes, I. Association of polymorphism in the cytochrome CYP2D6 and the efficacy and tolerability of simvastatin. Clin. Pharmacol. Ther. 2001, 70, 546–551. [Google Scholar] [CrossRef] [PubMed]
- Munshi, A.; Sharma, V.; Kaul, S.; Al-Hazzani, A.; Alshatwi, A.A.; Shafi, G.; Koppula, R.; Mallemoggala, S.B.; Jyothy, A. Association of 1347 G/A cytochrome P450 4F2 (CYP4F2) gene variant with hypertension and stroke. Mol. Boil. Rep. 2011, 39, 1677–1682. [Google Scholar] [CrossRef] [PubMed]
- Arsene, D.E.; Găină, G.; Bălescu, C.; Ardeleanu, C. C677T and A1298C methylenetetrahydropholate reductase (MTHFR) polymorphisms as factors involved in ischemic stroke. Rom. J. Morphol. Embryol. Rev. Roum. de Morphol. Embryol. 2011, 52, 1203–1207. [Google Scholar]
- Holmes, M.V.; Newcombe, P.; Hubacek, J.A.; Sofat, R.; Ricketts, S.L.; Cooper, J.; Breteler, M.; Bautista, L.E.; Sharma, P.; Whittaker, J.; et al. Effect modification by population dietary folate on the association between MTHFR genotype, homocysteine, and stroke risk: A meta-analysis of genetic studies and randomised trials. Lancet 2011, 378, 584–594. [Google Scholar] [CrossRef] [Green Version]
- Rutten-Jacobs, L.; Traylor, M.; Adib-Samii, P.; Thijs, V.; Sudlow, C.L.M.; Rothwell, P.M.; Boncoraglio, G.; Dichgans, M.; Meschia, J.; Maguire, J.; et al. Association of MTHFR C677T Genotype with Ischemic Stroke is confined to cerebral small vessel disease subtype. Stroke 2016, 47, 646–651. [Google Scholar] [CrossRef] [Green Version]
- Kang, S.; Wu, Y.; Liu, L.; Zhao, X.; Zhang, D. Association of the A1298C polymorphism in MTHFR gene with ischemic stroke. J. Clin. Neurosci. 2014, 21, 198–202. [Google Scholar] [CrossRef]
- Zhang, L.-L.; Hu, Z.-C.; Yin, Y.-W.; Li, B.-H.; Liu, Y.; Liao, S.-Q.; Gao, C.-Y.; Li, J.; Zhang, L.-L. A Meta-Analysis of the Relationship between MTHFR Gene A1298C polymorphism and the risk of adult stroke. Cerebrovasc. Dis. 2014, 38, 425–432. [Google Scholar] [CrossRef]
- Marcucci, R.; Betti, I.; Cecchi, E.; Poli, D.; Giusti, B.; Fedi, S.; Lapini, I.; Abbate, R.; Gensini, G.F.; Prisco, D. Hyperhomocysteinemia and vitamin B6 deficiency: New risk markers for nonvalvular atrial fibrillation? Am. Hear. J. 2004, 148, 456–461. [Google Scholar] [CrossRef]
- Giusti, B.; Gori, A.M.; Marcucci, R.; Sestini, I.; Saracini, C.; Sticchi, E.; Gensini, F.; Fatini, C.; Abbate, R.; Gensini, G.F. Role of C677T and A1298C MTHFR, A2756G MTR and -786 C/T eNOS Gene Polymorphisms in atrial fibrillation susceptibility. PLoS ONE 2007, 2, e495. [Google Scholar] [CrossRef]
- Içli, A.; Erten, N.; Arslan, A.; Yucel, H.; Akçay, S.; Yasar, E.; Uysal, B.A.; Baş, H.A.; Aksoy, F.; Sutcu, R. No Association between the Methyleletetrahydrofolate Reductase A1298C Variants and Atrial Fibrillation with Ischemic stroke in Turkish Population. J. Am. Coll. Cardiol. 2013, 62, C135–C136. [Google Scholar] [CrossRef] [Green Version]
- Chung, J.; Park, S.H.; Kim, N.; Kim, W.; Park, J.H.; Ko, Y.; Yang, M.H.; Jang, M.S.; Han, M.-K.; Jung, C.; et al. Trial of ORG 10172 in acute stroke treatment (TOAST) classification and vascular territory of ischemic stroke lesions diagnosed by diffusion-weighted imaging. J. Am. Hear. Assoc. 2014, 3. [Google Scholar] [CrossRef] [Green Version]
- Hacke, W.; Kaste, M.; Fieschi, C.; Toni, D.; Lesaffre, E.; Von Kummer, R.; Boysen, G.; Bluhmki, E.; Höxter, G.; Mahagne, M.-H.; et al. Intravenous thrombolysis with recombinant tissue plasminogen activator for acute hemispheric stroke. JAMA 1995, 274, 1017–1025. [Google Scholar] [CrossRef] [PubMed]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.-T.; Corrà, U.; Cosyns, B.; Deaton, C.; et al. 2016 European guidelines on cardiovascular disease prevention in clinical practice: The sixth joint task force of the European society of cardiology and other societies on cardiovascular disease prevention in clinical practice (constituted by representatives of 10 societies and by invited experts)developed with the special contribution of the European association for cardiovascular prevention & rehabilitation (EACPR). Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar] [PubMed]
- Nathan, D.M. The diabetes control and complications trial/epidemiology of diabetes interventions and complications study at 30 years: Overview. Diabetes Care 2013, 37, 9–16. [Google Scholar] [CrossRef] [Green Version]
- Little, R.; Rohlfing, C.; Wiedmeyer, H.M.; Myers, G.L.; Sacks, D.B.; Goldstein, D.E. The national glycohemoglobin standardization program: A five-year progress report. Clin. Chem. 2001, 47, 1985–1992. [Google Scholar]
- American Diabetes Association. American Diabetes Association Standards of Medical Care in Diabetes—2011. Diabetes Care 2010, 34, S11–S61. [Google Scholar] [CrossRef] [Green Version]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: The task force for the diagnosis and treatment of acute and chronic heart failure of the European society of cardiology (ESC) developed with the special contribution of the heart failure association (HFA) of the ESC. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar]
- January, C.T.; Wann, L.S.; Alpert, J.S.; Calkins, H.; Cigarroa, J.E.; Cleveland, J.C.; Conti, J.B.; Ellinor, P.T.; Ezekowitz, M.D.; Field, M.E.; et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation. J. Am. Coll. Cardiol. 2014, 64, e1–e76. [Google Scholar] [CrossRef] [Green Version]
- Lane, D.A.; Lip, G.Y. Use of the CHA 2 DS 2 -VASc and HAS-BLED scores to aid decision making for thromboprophylaxis in nonvalvular atrial fibrillation. Circulation 2012, 126, 860–865. [Google Scholar] [CrossRef] [Green Version]
- National Institutes of Health Stroke Scale (NIHSS). In Wiley StatsRef: Statistics Reference Online. Available online: https://onlinelibrary.wiley.com/doi/abs/10.1002/9781118445112.stat06823 (accessed on 10 February 2019).
- Sulter, G.; Steen, C.; De Keyser, J. Use of the Barthel index and modified Rankin scale in acute stroke trials. Stroke 1999, 30, 1538–1541. [Google Scholar] [CrossRef] [Green Version]
- Henning, R.J. Diagnosis and treatment of heart failure with preserved left ventricular ejection fraction. World J. Cardiol. 2020, 12, 7–25. [Google Scholar] [CrossRef] [PubMed]
- Rosenblatt, D.W.D.S. Inherited Disorders of Folate Transport and Metabolism. In The Metabolic Basis of Inherited Disease; McGraw-Hill: New York, NY, USA, 1989. [Google Scholar]
- Liew, S.-C.; Das Gupta, E. Methylenetetrahydrofolate reductase (MTHFR) C677T polymorphism: Epidemiology, metabolism and the associated diseases. Eur. J. Med. Genet. 2015, 58, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Hickey, S.E.; Curry, C.J.; Toriello, H.V. ACMG practice guideline: Lack of evidence for MTHFR polymorphism testing. Genet. Med. 2013, 15, 153–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biselli-Chicote, P.; Guerzoni, A.R.; De Godoy, M.F.; Eberlin, M.N.; Haddad, R.; Carvalho, V.M.; Vannucchi, H.; Pavarino-Bertelli, É.C.; Goloni-Bertollo, E. Genetic polymorphisms involved in folate metabolism and concentrations of methylmalonic acid and folate on plasma homocysteine and risk of coronary artery disease. J. Thromb. Thrombolysis 2009, 29, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Meng, Y.; Liu, X.; Ma, K.; Zhang, L.; Lu, M.; Zhao, M.; Guan, M.; Qin, G. Association of MTHFR C677T polymorphism and type 2 diabetes mellitus (T2DM) susceptibility. Mol. Genet. Genom. Med. 2019, 7. [Google Scholar] [CrossRef] [Green Version]
- Zhu, B.; Wu, X.; Zhi, X.; Liu, L.; Zheng, Q.; Sun, G. Methylenetetrahydrofolate Reductase C677T polymorphism and Type 2 diabetes Mellitus in Chinese Population: A meta-analysis of 29 case-control studies. PLoS ONE 2014, 9, e102443. [Google Scholar] [CrossRef]
- Hermans, M.P.; Gala, J.L.; Buysschaert, M. The MTHFR CT polymorphism confers a high risk for stroke in both homozygous and heterozygous T allele carriers with Type 2 diabetes. Diabetic Med. 2006, 23, 529–536. [Google Scholar] [CrossRef]
- Chen, S.; Dong, Z.; Cheng, M.; Zhao, Y.; Wang, M.; Sai, N.; Wang, X.; Liu, H.; Huang, G.; Zhang, X. Homocysteine exaggerates microglia activation and neuroinflammation through microglia localized STAT3 overactivation following ischemic stroke. J. Neuroinflamm. 2017, 14, 187. [Google Scholar] [CrossRef] [Green Version]
- Hu, X.; Wang, J.; Li, Y.; Wu, J.; Qiao, S.; Xu, S.; Huang, J.; Chen, L. The β-fibrinogen gene 455G/A polymorphism associated with cardioembolic stroke in atrial fibrillation with low CHA2DS2-VaSc score. Sci. Rep. 2017, 7, 17517. [Google Scholar] [CrossRef]
- Baum, L.; Wong, K.S.; Ng, H.K.; Tomlinson, B.; Rainer, T.; Chan, D.K.Y.; Thomas, G.N.; Chen, X.; Poon, P.; Cheung, W.S.; et al. Methylenetetrahydrofolate reductase gene A222V polymorphism and risk of ischemic stroke. Clin. Chem. Lab. Med. 2004, 42, 1370–1376. [Google Scholar] [CrossRef] [PubMed]
- Arboix, A.; Alió, J. Acute cardioembolic stroke: An update. Expert Rev. Cardiovasc. Ther. 2011, 9, 367–379. [Google Scholar] [CrossRef]
- Kang, S.; Zhao, X.; Liu, L.; Wu, W.; Zhang, N. Association of the C677T Polymorphism in the MTHFR Gene with Hemorrhagic Stroke: A Meta-Analysis. Genet. Test. Mol. Biomark. 2013, 17, 412–417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sazci, A.; Ergul, E.; Tuncer, N.; Akpınar, G.; Kara, I. Methylenetetrahydrofolate reductase gene polymorphisms are associated with ischemic and hemorrhagic stroke: Dual effect of MTHFR polymorphisms C677T and A1298C. Brain Res. Bull. 2006, 71, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Munshi, A.; Das, S.; Roy, S.; Kaul, S.; Jyothy, A. MTHFR gene (C677T) polymorphism in Ischemic stroke, its subtypes and hemorrhagic stroke in a South Indian population. Acta Medica Int. 2015, 2, 28–33. [Google Scholar] [CrossRef]
- Soriente, L.; Coppola, A.; Madonna, P.; Cerbone, A.M.; Di Minno, G.; Orefice, G.; D’Angelo, A. Homozygous C677T Mutation of the 5,10 Methylenetetrahydrofolate Reductase gene and Hyperhomocysteinemia in Italian patients with a history of early-onset ischemic stroke. Stroke 1998, 29, 869–871. [Google Scholar] [CrossRef]
- Fekih-Mrissa, N.; Mrad, M.; Klai, S.; Mansour, M.; Nsiri, B.; Gritli, N.; Mrissa, R. Methylenetetrahydrofolate Reductase (C677T and A1298C) Polymorphisms, Hyperhomocysteinemia, and Ischemic Stroke in Tunisian Patients. J. Stroke Cerebrovasc. Dis. 2013, 22, 465–469. [Google Scholar] [CrossRef]
- Al-Allawi, N.; Avo, A.; Jubrael, J.; Na, A.-A.; As, A.; Jm, J. Methylenetetrahydrofolate reductase C677T polymorphism in Iraqi patients with ischemic stroke. Neurol. India 2009, 57, 631–635. [Google Scholar] [CrossRef]
- Bellin, A.; Berto, P.; Themistoclakis, S.; Chandak, A.; Giusti, P.; Cavalli, G.; Bakshi, S.; Tessarin, M.; DeAmbrosis, P.; Chinellato, A. New oral anti-coagulants versus vitamin K antagonists in high thromboembolic risk patients. PLoS ONE 2019, 14, e0222762. [Google Scholar] [CrossRef]
- Cole, S.R.; Platt, R.W.; Schisterman, E.F.; Chu, H.; Westreich, D.; Richardson, D.; Poole, C. Illustrating bias due to conditioning on a collider. Int. J. Epidemiol. 2009, 39, 417–420. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Without MTHFR C677T Mutation (n = 41) | With MTHFR C677T Mutation (n = 26) | pT | ||
|---|---|---|---|---|---|
| Mean ± Std. Deviation (Median) | Mean Rank | Mean ± Std. Deviation (Median) | Mean Rank | ||
| Age, y | 73.00 ± 8.09 | 31.05 | 75.00 ± 9.03 | 38.65 | 0.119 |
| BMI, kg/m2 | 30.3 ± 4.04 | 28.25 | 32.01 ± 3.25 | 37.65 | 0.054 |
| NIHSS | (9) | 27.66 | (15) | 44.00 | 0.001 * |
| mRS | (3) | 28.52 | (4) | 42.63 | 0.003 * |
| CHA2DS2VASC | (5) | 29.93 | (7) | 40.42 | 0.029 * |
| HASBLED | (3) | 29.96 | (4) | 40.37 | 0.025 * |
| HTN grade, n (%) | (2) | 28.90 | (2) | 37.23 | 0.037 * |
| HF NYHA, n (%) | (0) | 27.21 | (2) | 38.30 | 0.016 * |
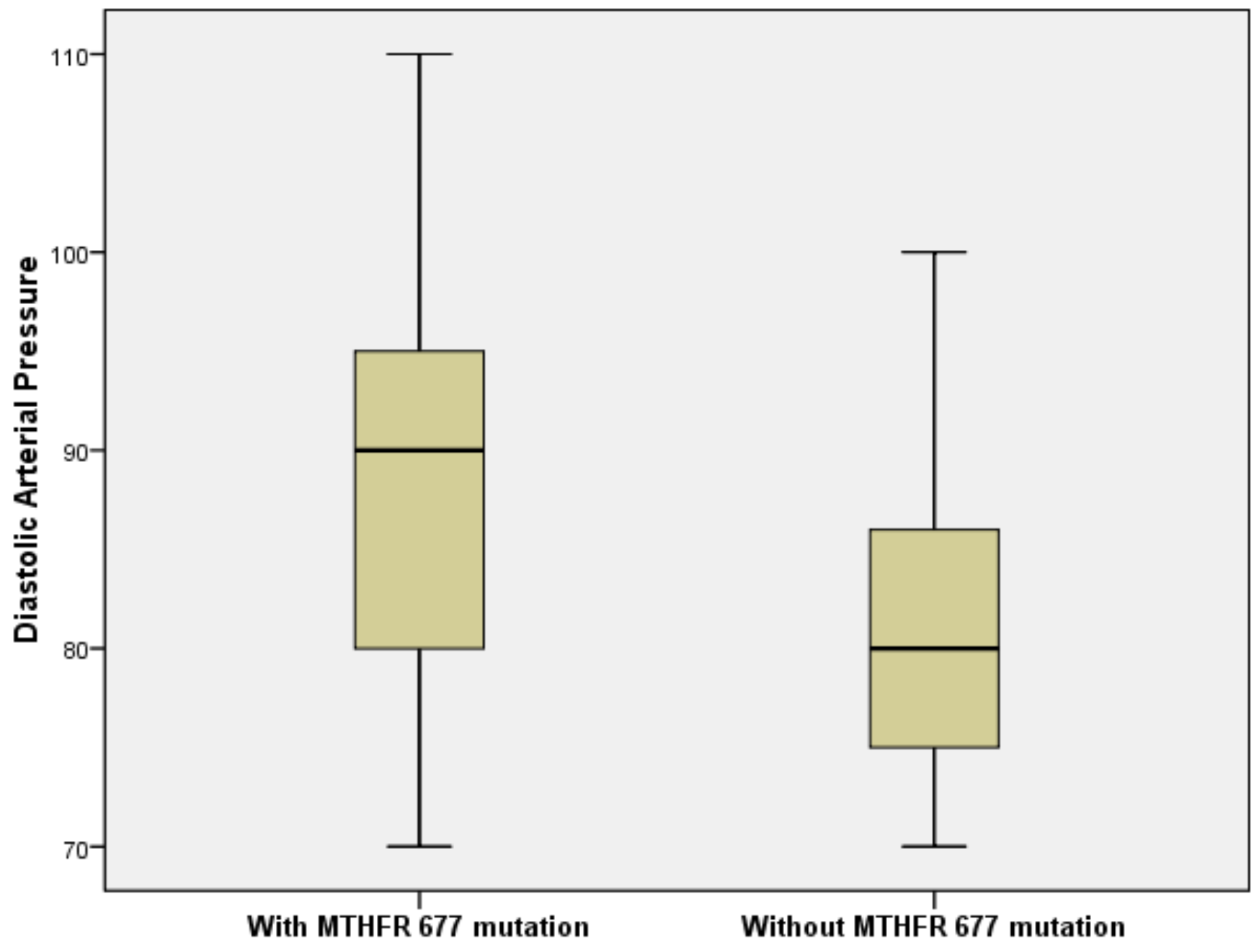
| DBP, mmHg | 81.5 ± 8.846 | 25.98 | 88.9 ± 11.593 | 39.09 | 0.007 * |
| SBP, mmHg | 159.19 ± 18.88 | 28.27 | 168.49 ± 23.57 | 37.63 | 0.054 |
| TC, mg/dL | 218.34 ± 59.52 | 39.66 | 176.96 ± 46.64 | 25.08 | 0.003 * |
| LDLc, mg/dL | 115.69 ± 33.83 | 25.19 | 152.02 ± 52.85 | 39.59 | 0.003 * |
| HDLc, mg/dL | 51.31 ± 14.92 | 46.27 | 36.24 ± 13.92 | 26.22 | <0.001 * |
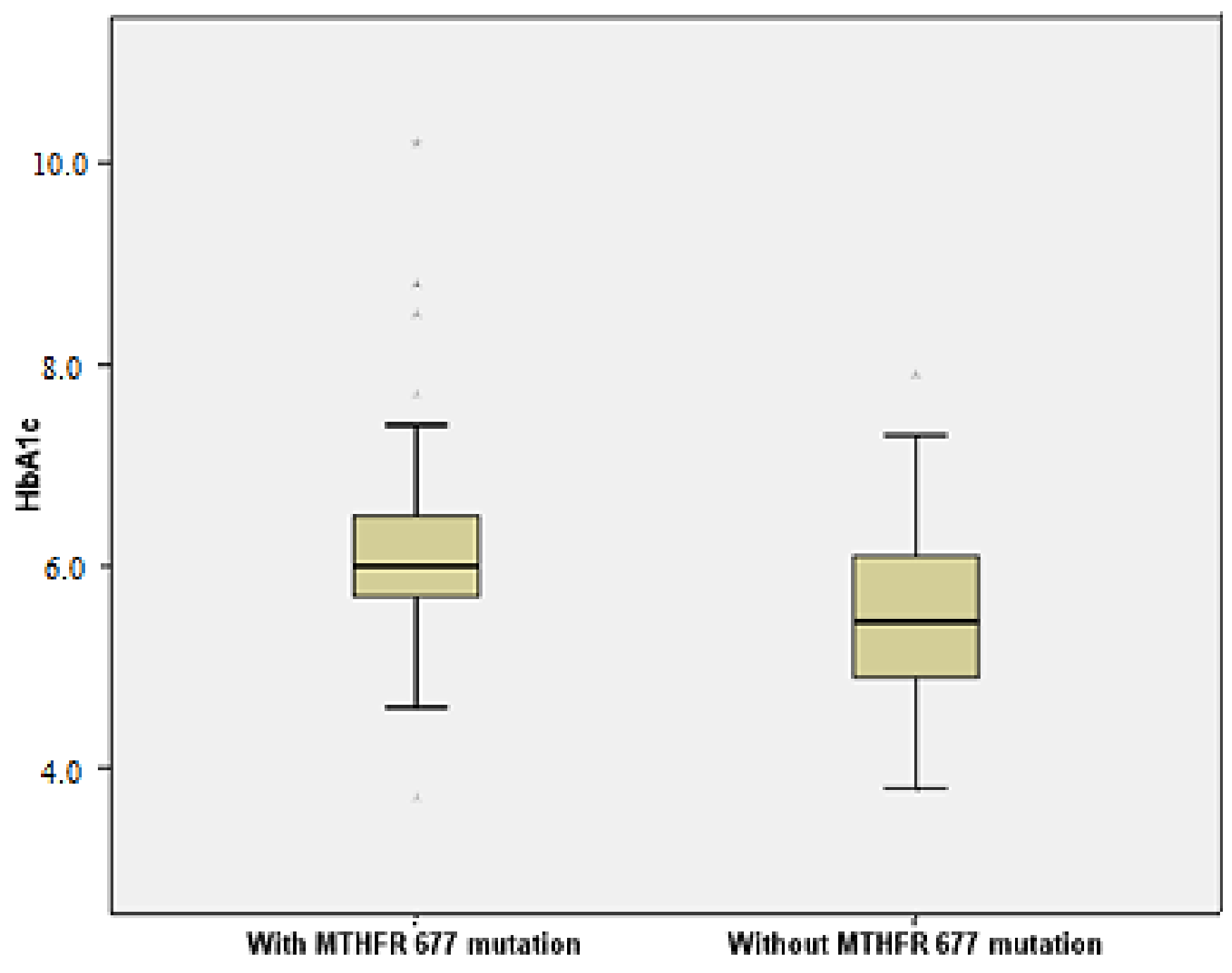
| HbA1c,% | 5.53 ± 1.02 | 25.40 | 6.23 ± 1.14 | 39.45 | 0.004 * |
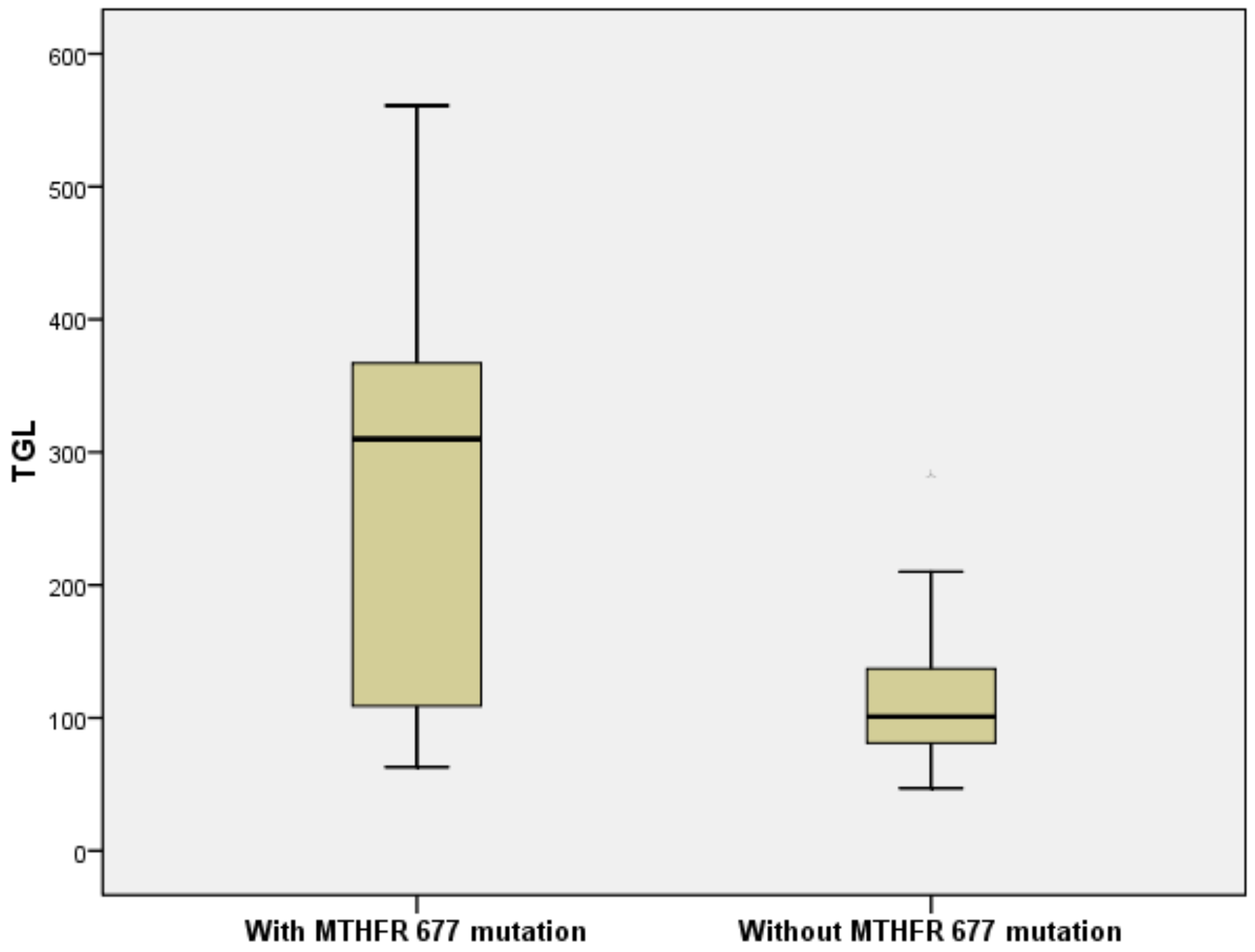
| TGL, mg/dL | 114.12 ± 52.24 | 22.02 | 266.1 ± 149.3 | 41.60 | <0.001 * |
| LAV, mL | 79.8 ± 29.25 | 31.83 | 85.19 ± 22.41 | 37.42 | 0.252 |
| LVEDV, mL | 122.56 ± 34.97 | 30.37 | 135.5 ± 31.19 | 39.73 | 0.055 |
| LVEF,% | 45.37 ± 9.94 | 30.24 | 50.42 ± 11.06 | 39.92 | 0.047 * |
| IMT, mm | 0.92 ± 0.3 | 31.43 | 1.03 ± 0.28 | 38.06 | 0.172 |
| hsCRP, mg/L | 7.01 ± 4.98 | 29.38 | 10.4 ± 5.81 | 41.29 | 0.015 * |
| INR | 1.76 ± 0.52 | 17.93 | 1.85 ± 0.49 | 19.65 | 0.638 |
| Variable | Without MTHFR C677T Mutation (n = 41) | With MTHFR C677T Mutation (n = 26) | pT |
|---|---|---|---|
| n (%) | n (%) | ||
| Sex (male) | 20 (48.8%) | 7 (26.9%) | 0.124 |
| Carotid Atheromatosis | 23 (56.1%) | 16 (61.5%) | 0.660 |
| CAD | 34 (82.9%) | 25 (96.2%) | 0.138 |
| PAD | 12 (29.3%) | 1 (3.8%) | 0.051 |
| T2DM | 16 (39.0%) | 11 (42.3%) | 0.804 |
| Ischemic CES: | 0.002 * | ||
| Sylvian territory | 39 (95.1%) | 16 (61.5%) | |
| Vertebrobasilar territory | 1 (2.4%) | 6 (23.1%) | |
| Hemorrhagic conversion of CES: | |||
| Hemorrhagic infarction | 0 (0%) | 4 (15.4%) | 0.020 * |
| Parenchymal hematoma | 1 (2.4%) | 0(0%) | 0.612 |
| Previous lacunar stroke | 8 (19.5%) | 15 (57.7%) | 0.003 * |
| Recurrent stroke | 10 (24.4%) | 18 (69.2%) | <0.001 * |
| Variable | Without MTHFR A1298C Mutation (n = 40) | With MTHFR A1298C Mutation (n = 27) | pT | ||
|---|---|---|---|---|---|
| Mean + Std. Deviation (Median) | Mean Rank | Mean + Std. Deviation (Median) | Mean Rank | ||
| Age, y | 72.38 ± 8.43 | 31.45 | 75.85 ± 8.21 | 37.78 | 0.192 |
| BMI, kg/m2 | 30.95 ± 3.99 | 31.46 | 31.95 ± 3.04 | 37.76 | 0.194 |
| NIHSS | (10) | 28.61 | (14) | 41.98 | 0.006 * |
| mRS | (3) | 29.58 | (3) | 40.56 | 0.020 * |
| CHA2DS2VASC | (6) | 32.80 | (6) | 35.78 | 0.534 |
| HASBLED | (4) | 30.85 | (4) | 38.67 | 0.090 |
| HTN grade, n(%) | (2) | 30.78 | (2) | 36.18 | 0.173 |
| HF NYHA, n(%) | (0) | 29.04 | (2) | 37.35 | 0.070 |
| DBP, mmHg | 84.85 ± 11.64 | 31.63 | 86.83 ± 10.88 | 35.60 | 0.408 |
| SBP, mmHg | 162.73 ± 23.13 | 32.20 | 168.07 ± 20.74 | 36.67 | 0.356 |
| TC, mg/dL | 173.07 ± 41.09 | 24.59 | 222 ± 60.09 | 40.35 | 0.001 * |
| LDLc, mg/dL | 107.04 ± 41.76 | 21.63 | 158.78 ± 43.22 | 42.35 | <0.001 * |
| HDLc, mg/dL | 49.78 ± 16.65 | 43.54 | 36.9 ± 13.43 | 27.56 | 0.001 * |
| HbA1c,% | 5.83 ± 1.47 | 29.39 | 6.05 ± 0.86 | 37.11 | 0.111 |
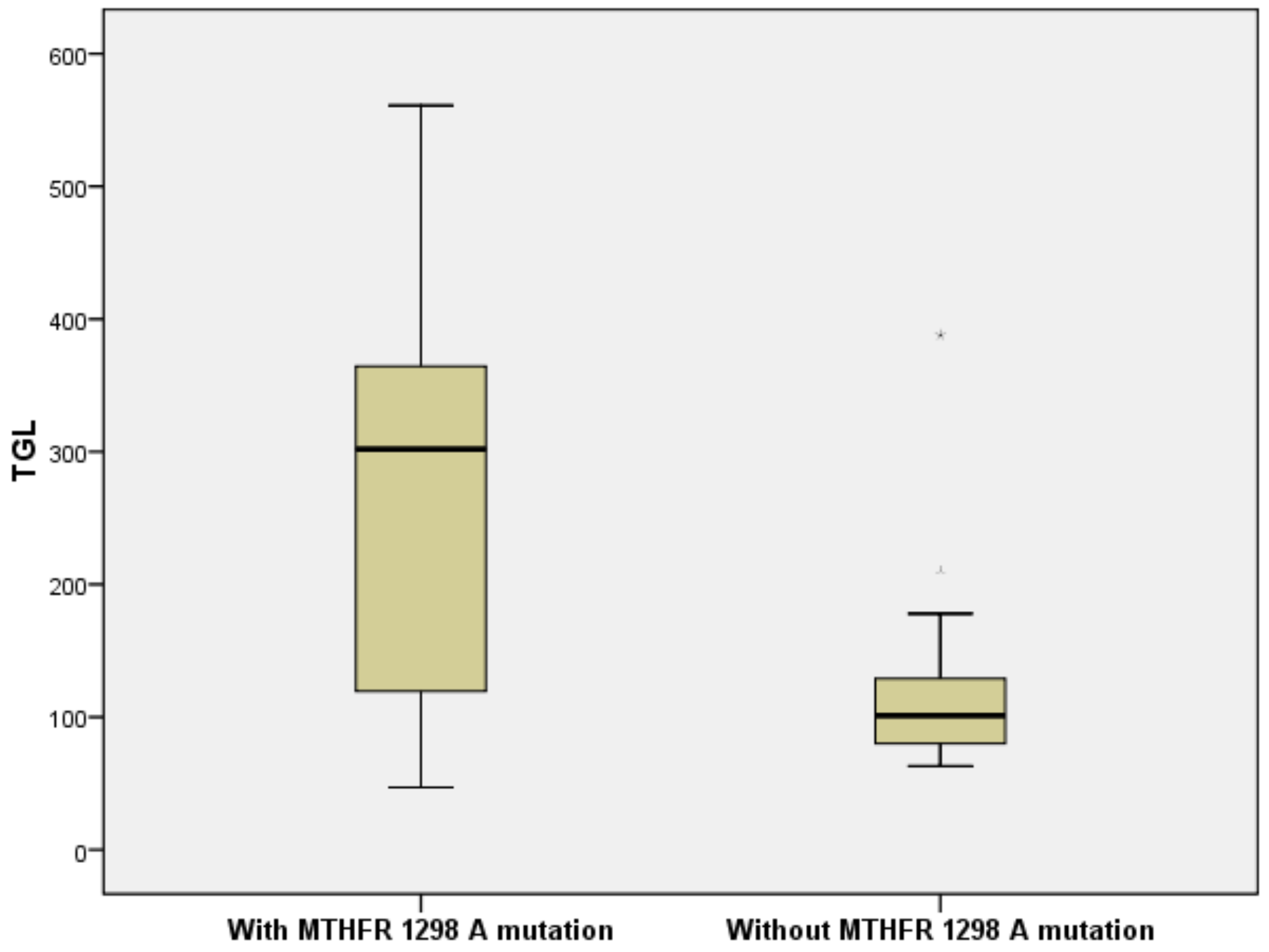
| TGL, mg/dL | 115.7 ± 65.45 | 22.06 | 268.83 ± 146.58 | 42.06 | <0.001 * |
| LAV, mL | 80.37 ± 26.33 | 33.08 | 84.15 ± 27.72 | 35.37 | 0.636 |
| LVEDV, mL | 123.84 ± 30.64 | 32.09 | 133.13 ± 38.19 | 36.83 | 0.328 |
| LVEF, mL | 45.7 ± 12.48 | 32.28 | 48.43 ± 9.12 | 35.16 | 0.552 |
| IMT, mm | 0.92 ± 0.29 | 30.71 | 1.04 ± 0.29 | 38.87 | 0.091 |
| hsCRP, mg/L | 8.06 ± 6.3 | 31.48 | 8.51 ± 5.02 | 35.70 | 0.385 |
| INR | 1.7 ± 0.49 | 16.72 | 1.91 ± 0.5 | 20.74 | 0.263 |
| Variable | Without MTHFR A1298C Mutation (n = 40) | With MTHFR A1298C Mutation (n = 27) | pT |
|---|---|---|---|
| n (%) | n (%) | ||
| Sex (male) | 14 (35.0%) | 13 (48.1%) | 0.318 |
| Carotid atheromatosis | 23 (57.5%) | 16 (59.3%) | 0.886 |
| CAD | 34 (85.0%) | 25 (92.6%) | 0.459 |
| PAD | 11 (27.5%) | 2 (7.4%) | 0.059 |
| T2DM | 15 (37.5%) | 12 (44.4%) | 0.618 |
| Ischemic CES: | 0.161 | ||
| Sylvian territor | 35 (87.5%) | 20 (74.1%) | |
| Vertebrobasilar territory | 4 (10%) | 3 (11.1%) | |
| Hemorrhagic conversion of CES: | |||
| Hemorrhagic infarction | 1 (2.5%) | 3 (11.1%) | 0.295 |
| Parenchymal hematoma | 0 (0%) | 1 (3.7%) | 0.403 |
| Lacunar stroke | 9 (22.5%) | 14 (51.9%) | 0.019 * |
| Recurrent stroke | 12 (30%) | 16 (59.3%) | 0.024 * |
| Variables in the Equation | ||||||||
|---|---|---|---|---|---|---|---|---|
| B | S.E. | Wald | df | Sig. | Exp(B) | 95% C.I. for EXP(B) | ||
| Lower | Upper | |||||||
| BMI | 0.221 | 0.113 | 3.836 | 1 | 0.050 | 1.802 | 1.643 | 2.950 |
| DBP | 0.127 | 0.046 | 7.607 | 1 | 0.006 * | 1.881 | 1.804 | 4.964 |
| HbA1c | 0.937 | 0.364 | 6.629 | 1 | 0.010 * | 1.392 | 1.192 | 7.799 |
| TGL | 0.018 | 0.006 | 8.565 | 1 | 0.003 * | 1.982 | 1.171 | 3.994 |
| Constant | 24.067 | 7.119 | 11.429 | 1 | 0.001 | 2.833E10 | ||
| Variables in the Equation | ||||||||
|---|---|---|---|---|---|---|---|---|
| B | S.E. | Wald | df | Sig. | Exp(B) | 95% C.I. for EXP(B) | ||
| Lower | Upper | |||||||
| TGL | 0.017 | 0.006 | 9.553 | 1 | 0.002 * | 2.983 | 1.972 | 7.994 |
| Constant | 8.430 | 4.261 | 3.914 | 1 | 0.048 | 4583.188 | ||
| n | Minimum | Maximum | Mean | Std. Error | Std. Deviation | |
|---|---|---|---|---|---|---|
| INR | 37 | 1.04 | 2.87 | 1.82 | 0.082 | 0.499 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chita, D.S.; Tudor, A.; Christodorescu, R.; Buleu, F.N.; Sosdean, R.; Deme, S.M.; Mercea, S.; Pop Moldovan, A.; Pah, A.M.; Docu Axelerad, A.; et al. MTHFR Gene Polymorphisms Prevalence and Cardiovascular Risk Factors Involved in Cardioembolic Stroke Type and Severity. Brain Sci. 2020, 10, 476. https://doi.org/10.3390/brainsci10080476
Chita DS, Tudor A, Christodorescu R, Buleu FN, Sosdean R, Deme SM, Mercea S, Pop Moldovan A, Pah AM, Docu Axelerad A, et al. MTHFR Gene Polymorphisms Prevalence and Cardiovascular Risk Factors Involved in Cardioembolic Stroke Type and Severity. Brain Sciences. 2020; 10(8):476. https://doi.org/10.3390/brainsci10080476
Chicago/Turabian StyleChita, Dana Simona, Anca Tudor, Ruxandra Christodorescu, Florina Nicoleta Buleu, Raluca Sosdean, Sanda Maria Deme, Simona Mercea, Adina Pop Moldovan, Ana Maria Pah, Any Docu Axelerad, and et al. 2020. "MTHFR Gene Polymorphisms Prevalence and Cardiovascular Risk Factors Involved in Cardioembolic Stroke Type and Severity" Brain Sciences 10, no. 8: 476. https://doi.org/10.3390/brainsci10080476