Importance of Maximal Strength and Muscle-Tendon Mechanics for Improving Force Steadiness in Persons with Parkinson’s Disease

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Participants
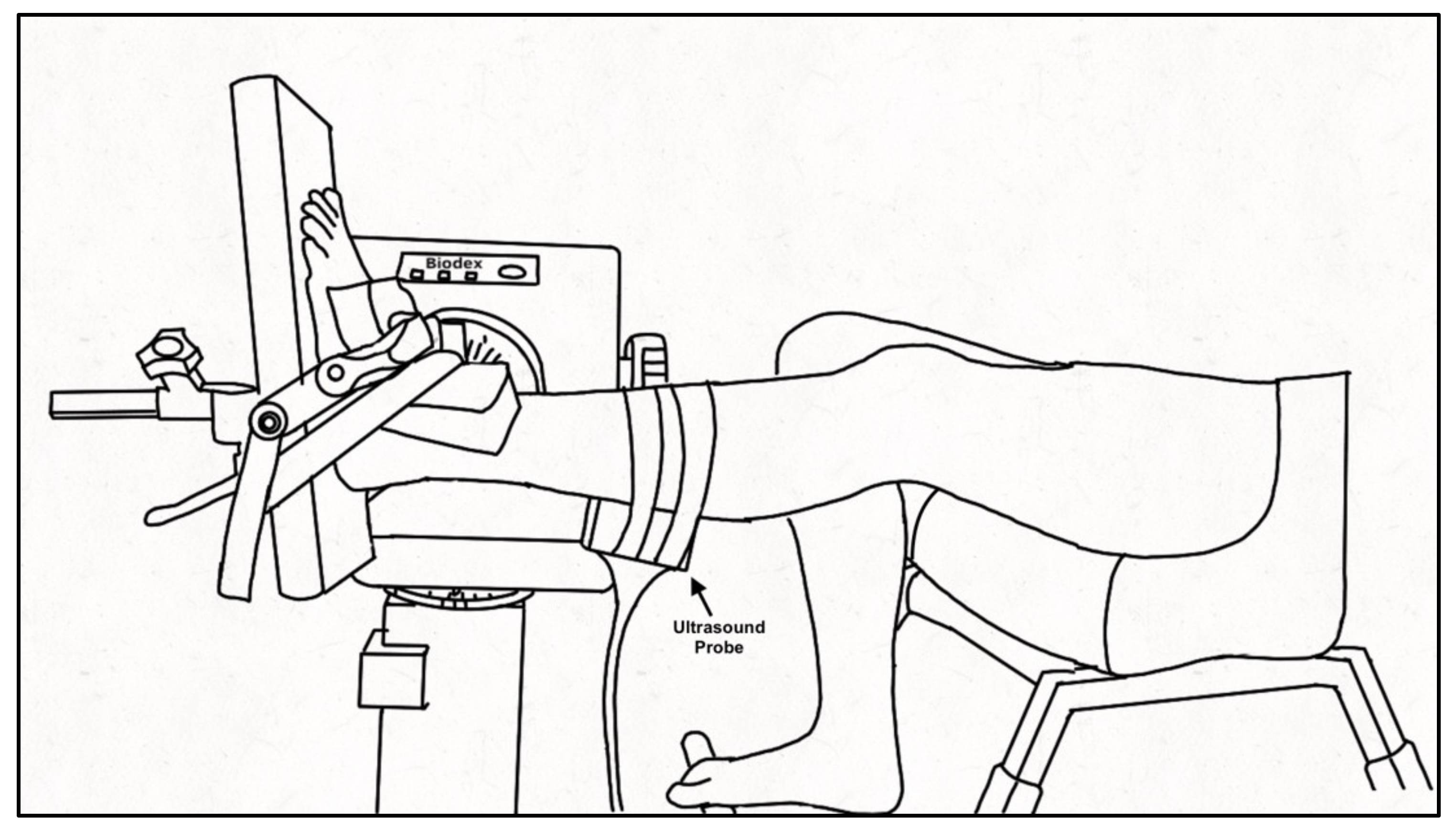
2.3. Experimental Setup and Protocol
2.4. Anatomical Measures
2.5. MVC and Force Steadiness
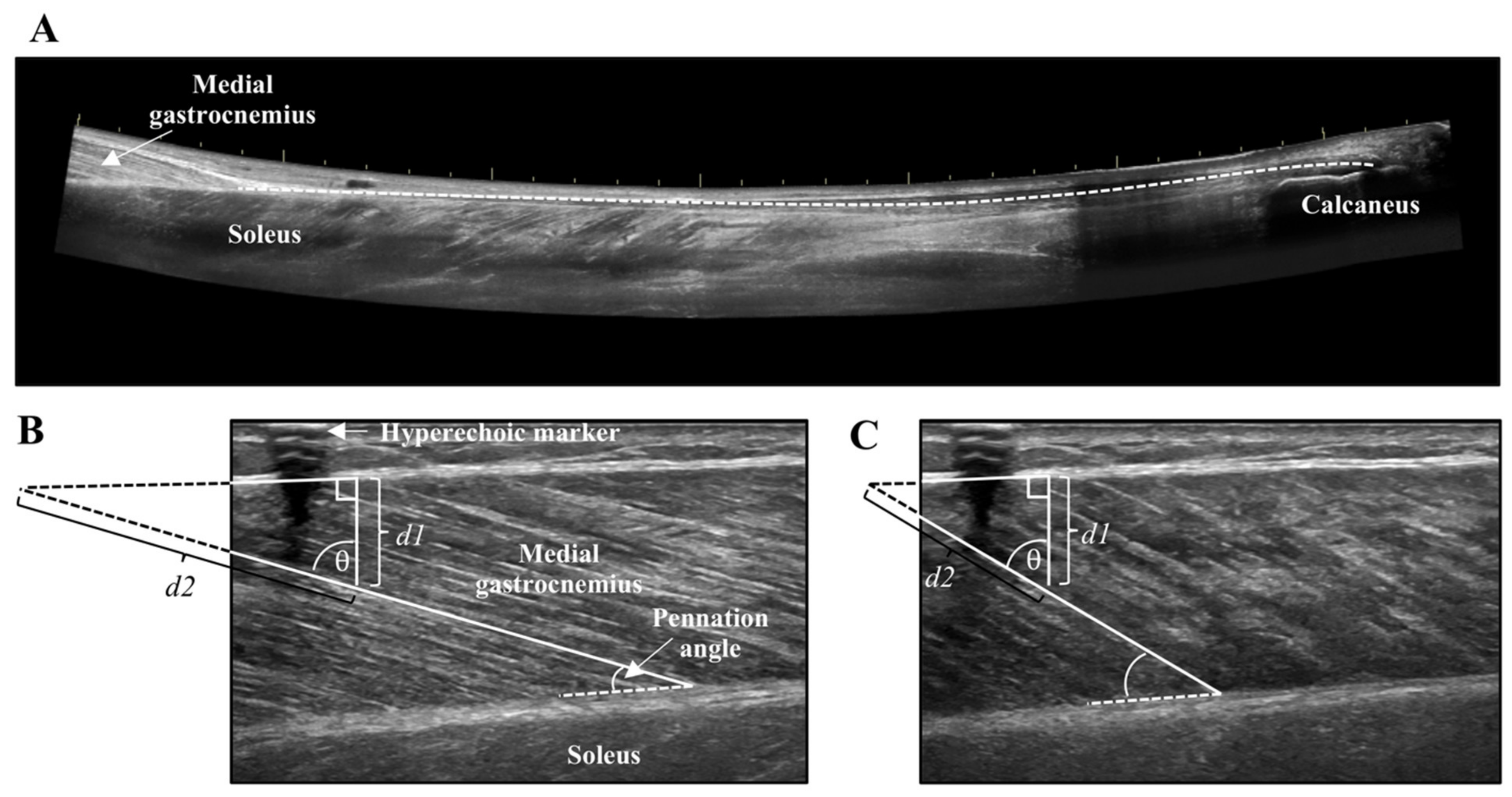
2.6. Ultrasound Analysis
2.7. Tendon Mechanics
2.8. Statistical Analysis
3. Results
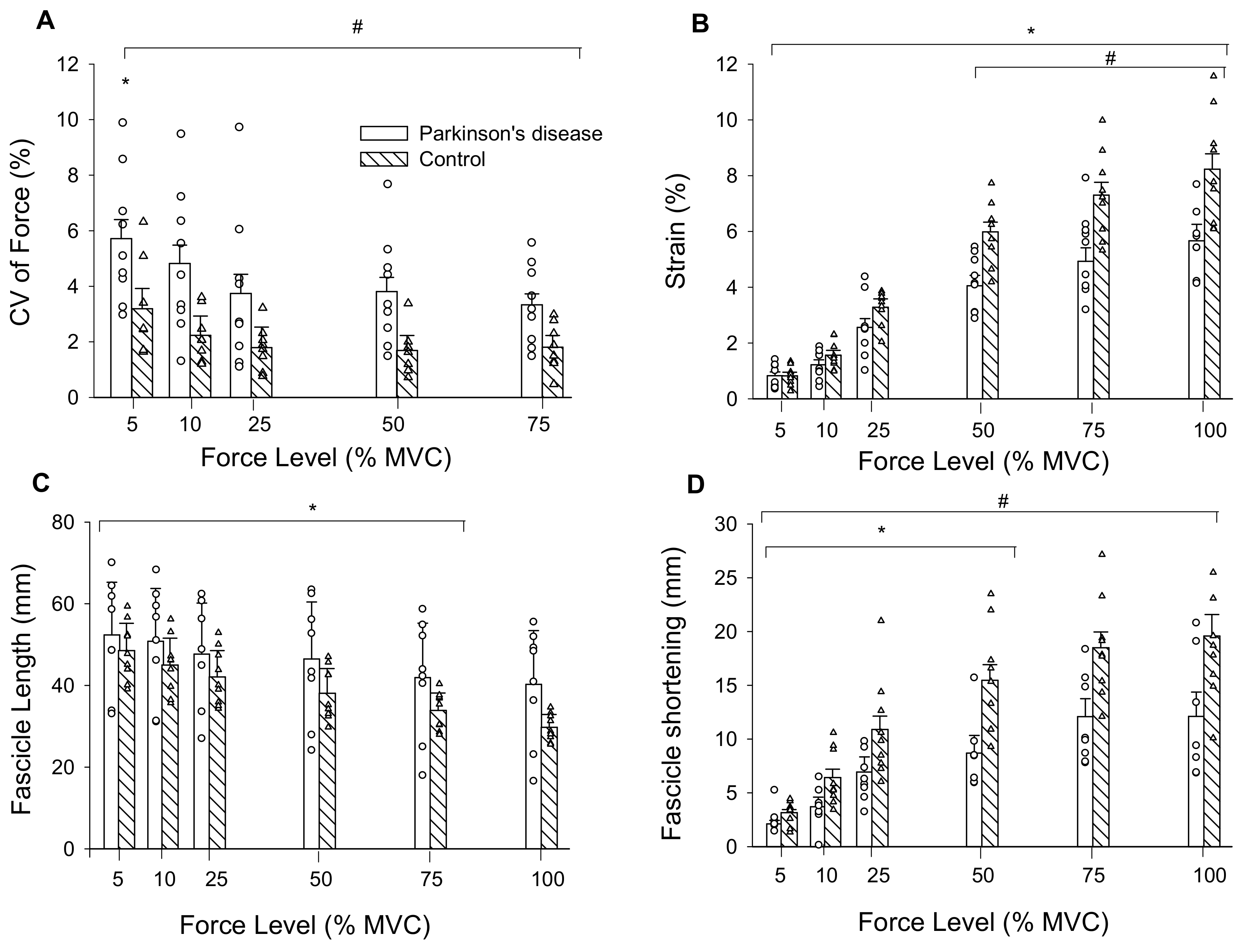
3.1. Tendon Mechanics
3.2. Muscle Fascicles
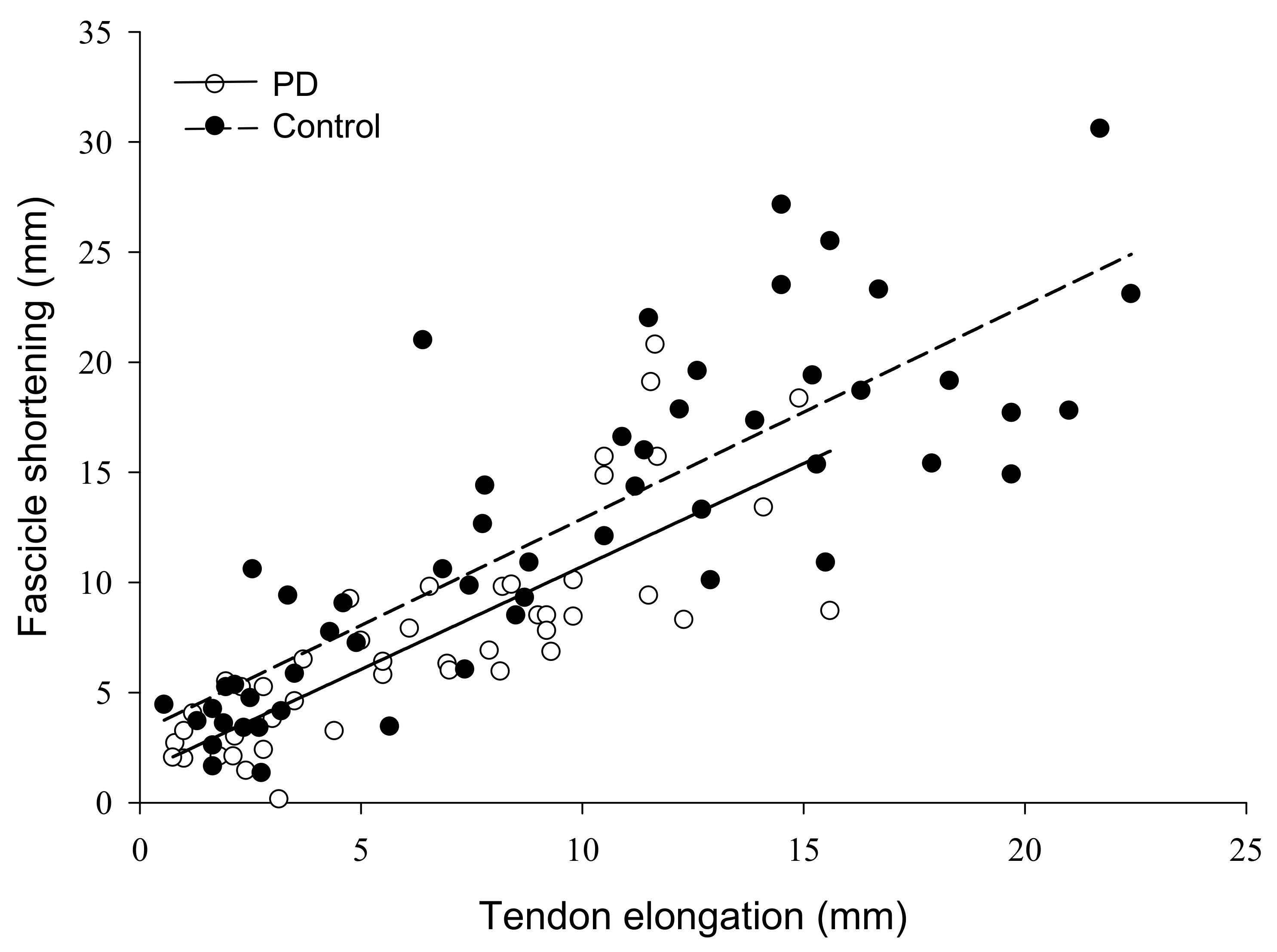
3.3. Correlation and Multiple Regression Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Jankovic, J. Parkinson’s disease clinical features and diagnosis. J. Neurol. Neurosurg. Psychiatry 2008, 79, 368–376. [Google Scholar] [CrossRef] [Green Version]
- Almuklass, A.M.; Price, R.C.; Gould, J.R.; Enoka, R.M. Force steadiness as a predictor of time to complete a pegboard test of dexterity in young men and women. J. Appl. Physiol. 2016, 120, 1410–1417. [Google Scholar] [CrossRef] [Green Version]
- Jones, G.R.; Roland, K.P.; Neubauer, N.A.; Jakobi, J.M. Handgrip Strength Related to Long-Term Electromyography. Arch. Phys. Med. Rehabil. 2016, 98, 347–352. [Google Scholar] [CrossRef]
- Roland, K.P.; Cornett, K.M.D.; Theou, O.; Jakobi, J.M.; Jones, G.R. Concurrence of Frailty and Parkinson’s Disease. J. Frailty Aging 2012, 1, 123–127. [Google Scholar]
- Roland, K.P.; Jones, G.R.; Jakobi, J.M. Daily electromyography in females with Parkinson’s disease: A potential indicator of frailty. Arch. Gerontol. Geriatr. 2014, 58, 80–87. [Google Scholar] [CrossRef]
- Seynnes, O.; Hue, O.A.; Garrandes, F.; Colson, S.S.; Bernard, P.L.; Legros, P.; Fiatarone Singh, M.A. Force steadiness in the lower extremities as an independent predictor of functional performance in older women. J. Aging Phys. Act. 2005, 13, 395–408. [Google Scholar] [CrossRef]
- Oshita, K.; Yano, S. Relationship between Force Fluctuation in the Plantar Flexor and Sustainable Time for Single-leg Standing. J. Physiol. Anthropol. 2010, 29, 89–93. [Google Scholar] [CrossRef] [Green Version]
- Skinner, J.W.; Christou, E.A.; Hass, C.J. Lower Extremity Muscle Strength and Force Variability in Persons With Parkinson Disease. J. Neurol. Phys. Ther. 2019, 43, 56–62. [Google Scholar] [CrossRef]
- Rose, M.H.; Løkkegaard, A.; Sonne-Holm, S.; Jensen, B.R. Tremor irregularity, torque steadiness and rate of force development in Parkinson’s disease. Motor. Control. 2013, 17, 203–216. [Google Scholar] [CrossRef] [Green Version]
- Brown, P.; Corcos, D.M.; Rothwell, J.C. Does parkinsonian action tremor contribute to muscle weakness in Parkinson’s disease? Brain 1997, 120, 401–408. [Google Scholar] [CrossRef] [Green Version]
- Ko, N.H.; Laine, C.M.; Fisher, B.E.; Valero-Cuevas, F.J. Force variability during dexterous manipulation in individuals with mild to moderate Parkinson’s disease. Front. Aging Neurosci. 2015, 7, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Enoka, R.M.; Christou, E.A.; Hunter, S.K.; Kornatz, K.W.; Semmler, J.G.; Taylor, A.M.; Tracy, B.L. Mechanisms that contribute to differences in motor performance between young and old adults. J. Electromyogr. Kinesiol. 2003, 13, 1–12. [Google Scholar] [CrossRef]
- Farina, D.; Negro, F. Common synaptic input to motor neurons, motor unit synchronization, and force control. Exerc. Sport Sci. Rev. 2015, 43, 23–33. [Google Scholar] [CrossRef]
- Jakobi, J.M.; Haynes, E.M.K.; Smart, R.R. Is there sufficient evidence to explain the cause of sexually dimorphic behaviour in force steadiness? Appl. Physiol. Nutr. Metab. 2018, 43, 1207–1214. [Google Scholar] [CrossRef] [Green Version]
- Johannsson, J.; Jakobi, J.; Duchateau, J.; Baudry, S. Do mechanical properties of Achilles tendon influence torque steadiness? Comput. Methods Biomech. Biomed. Eng. 2015, 18, 1958–1959. [Google Scholar] [CrossRef]
- Smart, R.R.; Baudry, S.; Fedorov, A.; Kuzyk, S.L.; Jakobi, J.M. Influence of biceps brachii tendon mechanical properties on elbow flexor force steadiness in young and old males. Scand. J. Med. Sci. Sport 2018, 28, 983–991. [Google Scholar] [CrossRef]
- Smart, R.R.; Kohn, S.; Richardson, C.M.; Jakobi, J.M. Influence of forearm orientation on biceps brachii tendon mechanics and elbow flexor force steadiness. J. Biomech. 2018, 76, 129–135. [Google Scholar] [CrossRef]
- Feeney, D.F.; Mani, D.; Enoka, R.M. Variability in common synaptic input to motor neurons modulates both force steadiness and pegboard time in young and older adults. J. Physiol. 2018, 596, 3793–3806. [Google Scholar] [CrossRef] [Green Version]
- Onambélé, G.L.; Narici, M.V.; Maganaris, C.N. Calf Muscle-Tendon Properties and Postural Balance in Old Age. J. Appl. Physiol. 2006, 100, 2048–2056. [Google Scholar] [CrossRef]
- Marusiak, J.; Jaskólska, A.; Budrewicz, S.; Koszewicz, M.; Jaskólski, A. Increased Muscle Belly and Tendon Stiffness in Patients with Parkinson’s Disease, as Measured by Myotonometry. Mov. Disord. 2011, 26, 2119–2122. [Google Scholar] [CrossRef]
- Koh, S.; Roh, J.; Kim, J.; Oh, K.; Kim, B.; Kim, G.; Park, B.; Kim, S.; Yoon, J. Ultrasonographic findings of shoulder disorders in patients with Parkinson’s disease. Mov. Disord. 2008, 23, 1772–1776. [Google Scholar] [CrossRef] [PubMed]
- Tan, B.; Double, K.L.; Burne, J.; Diong, J. Tension-referenced measures of gastrocnemius slack length and stiffness in Parkinson’s disease. Mov. Disord. 2016, 31, 1914–1918. [Google Scholar] [CrossRef] [PubMed]
- Orselli, M.I.V.; Franz, J.R.; Thelen, D.G. The effects of Achilles tendon compliance on triceps surae mechanics and energetics in walking. J. Biomech. 2017, 60, 227–231. [Google Scholar] [CrossRef]
- Csapo, R.; Maganaris, C.N.; Seynnes, O.R.; Narici, M.V. On muscle, tendon and high heels. J. Exp. Biol. 2010, 213, 2582–2588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bohm, S.; Mersmann, F.; Arampatzis, A. Human tendon adaptation in response to mechanical loading: A systematic review and meta-analysis of exercise intervention studies on healthy adults. Sport Med. Open 2015, 1, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stevens-Lapsley, J.; Kluger, B.M.; Schenkman, M. Quadriceps muscle weakness, activation deficits, and fatigue with parkinson Disease. Neurorehabil. Neural Repair 2012, 26, 533–541. [Google Scholar] [CrossRef]
- Ryan, E.D.; Rosenberg, J.G.; Scharville, M.J.; Sobolewski, E.J.; Thompson, B.J.; King, G.E. Test-Retest Reliability and the Minimal Detectable Change for Achilles Tendon Length: A Panoramic Ultrasound Assessment. Ultrasound Med. Biol. 2013, 39, 2488–2491. [Google Scholar] [CrossRef]
- Kuzyk, S.L.; Smart, R.R.; Simpson, C.L.; Fedorov, A.; Jakobi, J.M. Influence of fascicle length on twitch potentiation of the medial gastrocnemius across three ankle angles. Eur. J. Appl. Physiol. 2018, 118, 1199–1207. [Google Scholar] [CrossRef]
- Simpson, C.L.; Kim, B.D.H.; Bourcet, M.R.; Jones, G.R.; Jakobi, J.M. Stretch training induces unequal adaptation in muscle fascicles and thickness in medial and lateral gastrocnemii. Scand. J. Med. Sci. Sport 2017, 27, 1597–1604. [Google Scholar] [CrossRef]
- Arampatzis, A.; Mademli, L.; De Monte, G.; Walsh, M. Changes in fascicle length from rest to maximal voluntary contraction affect the assessment of voluntary activation. J. Biomech. 2007, 40, 3193–3200. [Google Scholar] [CrossRef]
- Lichtwark, G.A.; Wilson, A.M. Optimal muscle fascicle length and tendon stiffness for maximising gastrocnemius efficiency during human walking and running. J. Theor. Biol. 2008, 252, 662–673. [Google Scholar] [CrossRef] [Green Version]
- Stelmach, G.; Tesdale, N.; Phillips, J.; Worringham, C. Force production characteristics in Parkinson’s diease. Exp. Brain Res. 1989, 76, 165–172. [Google Scholar] [CrossRef] [Green Version]
- Hammond, K.G.; Pfeiffer, R.F.; LeDoux, M.S.; Schilling, B.K. Neuromuscular rate of force development deficit in Parkinson disease. Clin. Biomech. 2017, 45, 14–18. [Google Scholar] [CrossRef] [PubMed]
- Folland, J.P.; Haas, B.; Castle, P. Strength and activation of the knee musculature in Parkinson’s disease: Effect of medication. NeuroRehabilitation 2011, 29, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Shulman, L.M.; Gruber-Baldini, A.L.; Anderson, K.E.; Fishman, P.S.; Reich, S.G.; Weiner, W.J. The clinically important difference on the unified parkinson’s disease rating scale. Arch. Neurol. 2010, 67, 64–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laine, C.M.; Valero-Cuevas, F.J. Parkinson’s Disease Exhibits Amplified Intermuscular Coherence During Dynamic Voluntary Action. Front. Neurol. 2020, 11, 204. [Google Scholar] [CrossRef]
- Milner-Brown, H.; Fisher, M.; Weiner, W.J. Electrical Properties of Motor Units in Parkinsonism and a Possible Relationship With Bradykinesia. J. Neurol. Neurosurg. Psychiatry 1979, 42, 35–41. [Google Scholar] [CrossRef] [Green Version]
- Glendinning, D.; Enoka, R.M. Motor Unit Behavior in Parkinson’s Disease. Phys. Ther. 1994, 74, 61–70. [Google Scholar] [CrossRef]
- Agapaki, O.; Christakos, C.; Anastasopoulos, D. Characteristics of rest and postural tremors in Parkinson’s disease: An analysis of motor unit firing synchrony and patterns. Front. Hum. Neurosci. 2018, 12, 179. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Controls (n = 9, 6 Females) | PD (n = 9, 6 Females) | 95% CI of Difference | ||
|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Lower | Upper | |
| Age (years) | 70 ± 7 | 70 ± 5 | −6.48 | 6.25 |
| Height (cm) | 163.3 ± 7.1 | 166.0 ± 9.8 | −6.52 | 6.29 |
| Body Mass (kg) | 66.8 ± 14.6 | 65.8 ± 10.8 | −11.21 | 5.88 |
| MDS-UPDRS Motor Score | N/A | 12.7 ± 6.7 | ||
| Duration of PD (years) | N/A | 6 ± 3 | ||
| Controls (n = 9, 6 Females) | PD (n = 9, 6 Females) | 95% CI of Difference | ||
|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Lower | Upper | |
| Standing ankle angle (°) | 99 ± 4 | 94 ± 8 | −1.75 | 11.53 |
| MVC (N) | 429.2 ± 105.8 * | 318.9 ± 99.4 | 7.70 | 212.94 |
| Resting tendon length (mm) | 207.4 ± 18.3 | 204.0 ± 30.4 | −21.67 | 28.45 |
| Resting tendon CSA (mm2) | 38.8 ± 13.5 | 36.3 ± 14.8 | −11.68 | 16.57 |
| MG and LG Muscle CSA (mm2) | 1509.7 ± 614.2 | 1175.3 ± 347.7 | −164.37 | 833.03 |
| Fascicle Length (mm) | 48.5 ± 7.1 | 52.3 ± 13.7 | −15.73 | 8.25 |
| Fascicle Pennation Angle (°) | 21.78 ± 5.28 | 20.81 ± 4.08 | −3.96 | 5.90 |
| Low Forces (5, 10% MVC) | |||||
| MVC | Strain (%) | Stress | Stiffness | MLR | |
| (N) | (MPa) | (N mm−1) | |||
| PD | −0.787 * | −0.633 * | −0.570 * | n/a | y = 11.805 − 0.017a − 0.802b |
| ß = −0.671 | ß = −0.345 | r2 = 0.725, adjusted r2 = 0.688 | |||
| Controls | −0.641 * | −0.293 | −0.429 * | n/a | y = 8.299 − 0.012a |
| ß = −0.641 | r2 = 0.410, adjusted r2 = 0.368 | ||||
| High Forces (25, 50, 75% MVC) | |||||
| MVC | Strain (%) | Stress | Stiffness | MLR | |
| (N) | (MPa) | (N mm−1) | |||
| PD | −0.591 * | −0.446 * | −0.433 * | −0.132 | y = 7.829 − 0.013a |
| ß = −0.591 | r2 = 0.349, adjusted r2 = 0.319 | ||||
| Controls | −0.655 * | 0.067 | −0.007 | −0.351 # | y = 5.133 − 0.006a − 0.009c |
| ß = −0.669 | ß = −0.376 | r2 = 0.570, adjusted r2 = 0.522 | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smart, R.R.; Richardson, C.M.; Wile, D.J.; Dalton, B.H.; Jakobi, J.M. Importance of Maximal Strength and Muscle-Tendon Mechanics for Improving Force Steadiness in Persons with Parkinson’s Disease. Brain Sci. 2020, 10, 471. https://doi.org/10.3390/brainsci10080471
Smart RR, Richardson CM, Wile DJ, Dalton BH, Jakobi JM. Importance of Maximal Strength and Muscle-Tendon Mechanics for Improving Force Steadiness in Persons with Parkinson’s Disease. Brain Sciences. 2020; 10(8):471. https://doi.org/10.3390/brainsci10080471
Chicago/Turabian StyleSmart, Rowan R., Cydney M. Richardson, Daryl J. Wile, Brian H. Dalton, and Jennifer M. Jakobi. 2020. "Importance of Maximal Strength and Muscle-Tendon Mechanics for Improving Force Steadiness in Persons with Parkinson’s Disease" Brain Sciences 10, no. 8: 471. https://doi.org/10.3390/brainsci10080471