Changes in Metabolites During an Oral Glucose Tolerance Test in Early and Mid-Pregnancy: Findings from the PEARLS Randomized, Controlled Lifestyle Trial

 ,
,
Abstract
:1. Introduction
2. Results
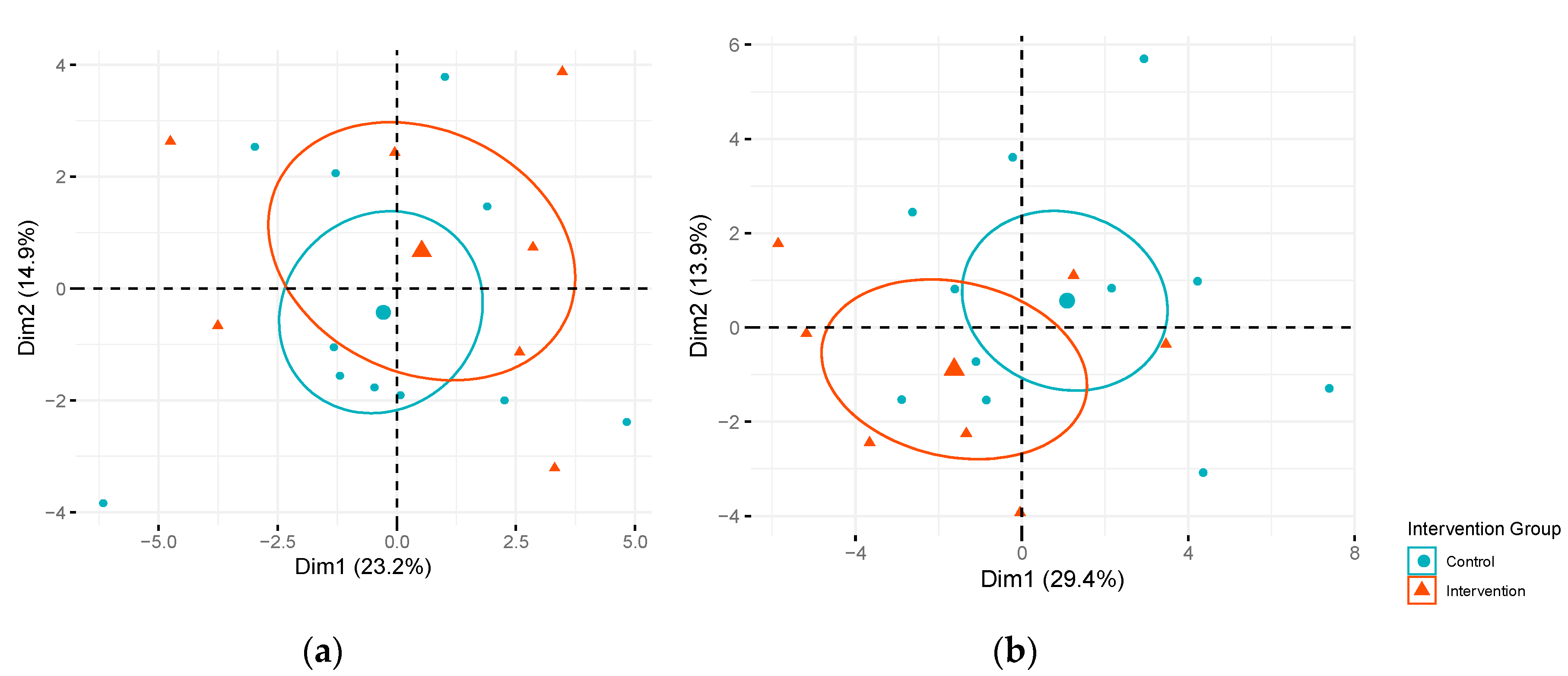
2.1. Influence of Intervention on Changes in Metabolites during an OGTT Among Pregnant Women
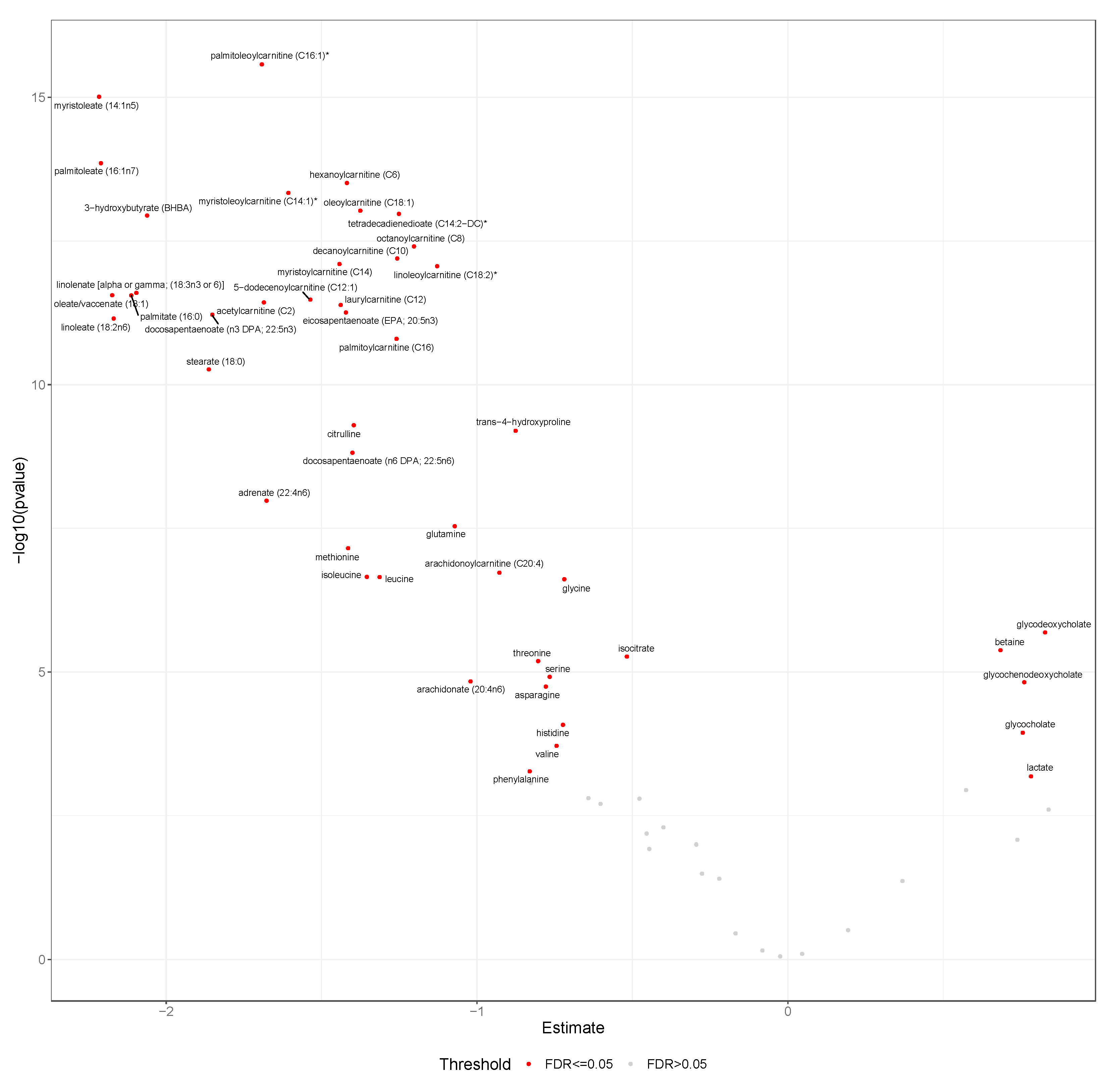
2.2. Changes in Metabolites during an OGTT
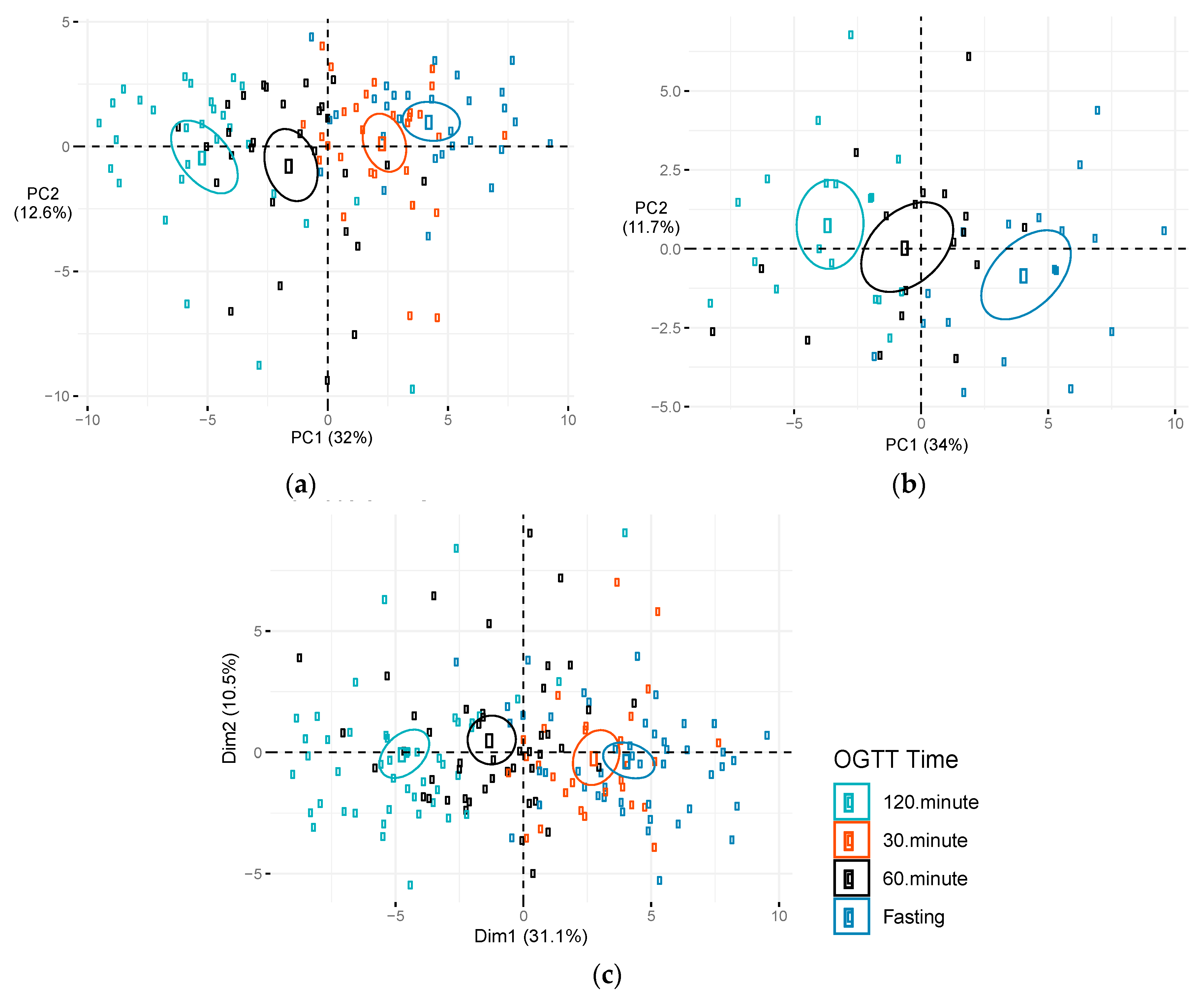
2.3. Differences in Changes in Metabolites during OGTT at Early Versus Mid-Pregnancy
2.4. Sensitivity Analyses
3. Discussion
3.1. Changes in Metabolites during an OGTT at Early Versus Mid-Pregnancy
3.2. Influence of Intervention on Changes in Metabolites during OGTT Among Pregnant Women
3.3. Study Strengths and Limitations
4. Materials and Methods
4.1. Study Population
4.2. Metabolomics Profiling
4.3. Participant Characteristics
4.4. Statistical Analysis
5. Conclusions and Future Perspectives
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- American Cancer Society. Cancer facts and figures. 2020. Available online: Https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2020/cancer-facts-and-figures-2020.pdf (accessed on 6 July 2020).
- Barr, E.L.; Zimmet, P.Z.; Welborn, T.A.; Jolley, D.; Magliano, D.J.; Dunstan, D.W.; Cameron, A.J.; Dwyer, T.; Taylor, H.R.; Tonkin, A.M.; et al. Risk of Cardiovascular and All-Cause Mortality in Individuals With Diabetes Mellitus, Impaired Fasting Glucose, and Impaired Glucose Tolerance. Circulation 2007, 116, 151–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anonymous. Glucose tolerance and mortality: Comparison of WHO and American Diabetic Association diagnostic criteria. Lancet 1999, 354, 617–621. [Google Scholar] [CrossRef]
- Bellamy, L.; Casas, J.-P.; Hingorani, A.D.; Williams, D. Type 2 diabetes mellitus after gestational diabetes: A systematic review and meta-analysis. Lancet 2009, 373, 1773–1779. [Google Scholar] [CrossRef]
- Szmuilowicz, E.D.; Josefson, J.L.; Metzger, B.E. Gestational Diabetes Mellitus. Endocrinol. Metab. Clin. N. Am. 2019, 48, 479–493. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Zhang, C. Prevalence of Gestational Diabetes and Risk of Progression to Type 2 Diabetes: A Global Perspective. Curr. Diabetes Rep. 2016, 16, 7. [Google Scholar] [CrossRef] [PubMed]
- Homko, C.J.; Sivan, E.; Reece, E.A.; Boden, G. Fuel metabolism during pregnancy. Semin. Reprod. Endocrinol. 1999, 17, 119–125. [Google Scholar] [CrossRef]
- Barbour, L.A.; McCurdy, C.E.; Hernandez, T.L.; Kirwan, J.P.; Catalano, P.M.; Friedman, J.E. Cellular Mechanisms for Insulin Resistance in Normal Pregnancy and Gestational Diabetes. Diabetes Care 2007, 30, S112–S119. [Google Scholar] [CrossRef] [Green Version]
- Kampmann, U.; Knorr, S.; Fuglsang, J.; Ovesen, P. Determinants of Maternal Insulin Resistance during Pregnancy: An Updated Overview. J. Diabetes Res. 2019, 2019, 5320156. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association. Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 2012, 35, S64–S71. [Google Scholar] [CrossRef] [Green Version]
- Institute of Medicine (US) and National Research Council (US) Committee to Reexamine IOM Pregnancy Weight Guidelines. Weight Gain During Pregnancy: Reexamining the Guidelines; Rasmussen, K.M., Yaktine, A.L., Eds.; The National Academies Collection: Reports funded by National Institutes of Health; National Academies Press: Washington, DC, USA, 2009; ISBN 978-0-309-13113-1. [Google Scholar]
- Nowak, C.; Hetty, S.; Salihovic, S.; Castillejo-Lopez, C.; Ganna, A.; Cook, N.L.; Broeckling, C.D.; Prenni, J.E.; Shen, X.; Giedraitis, V.; et al. Glucose challenge metabolomics implicates medium-chain acylcarnitines in insulin resistance. Sci. Rep. 2018, 8, 8691. [Google Scholar] [CrossRef] [PubMed]
- Miki, T.; Lee, E.Y.; Eguchi, A.; Sakurai, K.; Sawabe, Y.; Yoshida, T.; Saito, K.; Yokoh, H.; Ishikawa, K.; Yokote, K.; et al. Accelerated oligosaccharide absorption and altered serum metabolites during oral glucose tolerance test in young Japanese with impaired glucose tolerance. J. Diabetes Investig. 2018, 9, 512–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bentley-Lewis, R.; Xiong, G.; Lee, H.; Yang, A.; Huynh, J.; Kim, C. Metabolomic analysis reveals amino-acid responses to an oral glucose tolerance test in women with prior history of gestational diabetes mellitus. J. Clin. Transl. Endocrinol. 2014, 1, 38–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ho, J.E.; Larson, M.G.; Vasan, R.S.; Ghorbani, A.; Cheng, S.; Rhee, E.P.; Florez, J.C.; Clish, C.B.; Gerszten, R.E.; Wang, T.J. Metabolite Profiles During Oral Glucose Challenge. Diabetes 2013, 62, 2689–2698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, X.; Peter, A.; Fritsche, J.; Elcnerova, M.; Fritsche, A.; Häring, H.-U.; Schleicher, E.D.; Xu, G.; Lehmann, R. Changes of the plasma metabolome during an oral glucose tolerance test: Is there more than glucose to look at? Am. J. Physiol. Endocrinol. Metab. 2009, 296, E384–E393. [Google Scholar] [CrossRef] [PubMed]
- Wildberg, C.; Masuch, A.; Budde, K.; Kastenmüller, G.; Artati, A.; Rathmann, W.; Adamski, J.; Kocher, T.; Völzke, H.; Nauck, M.; et al. Plasma Metabolomics to Identify and Stratify Patients With Impaired Glucose Tolerance. J. Clin. Endocrinol. Metab. 2019, 104, 6357–6370. [Google Scholar] [CrossRef] [PubMed]
- Shaham, O.; Wei, R.; Wang, T.J.; Ricciardi, C.; Lewis, G.D.; Vasan, R.S.; Carr, S.A.; Thadhani, R.; Gerszten, R.E.; Mootha, V.K. Metabolic profiling of the human response to a glucose challenge reveals distinct axes of insulin sensitivity. Mol. Syst. Biol. 2008, 4, 214. [Google Scholar] [CrossRef] [PubMed]
- Gelaye, B.; Clish, C.B.; Denis, M.; Larrabure, G.; Tadesse, M.G.; Deik, A.; Pierce, K.; Bullock, K.; Dennis, C.; Enquobahrie, D.A.; et al. Metabolomics signatures associated with an oral glucose challenge in pregnant women. Diabetes Metab. 2019, 45, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Scholtens, D.M.; Bain, J.R.; Reisetter, A.C.; Muehlbauer, M.J.; Nodzenski, M.; Stevens, R.D.; Ilkayeva, O.; Lowe, L.P.; Metzger, B.E.; Newgard, C.B.; et al. Metabolic Networks and Metabolites Underlie Associations Between Maternal Glucose During Pregnancy and Newborn Size at Birth. Diabetes 2016, 65, 2039–2050. [Google Scholar] [CrossRef] [Green Version]
- Wang, T.J.; Ngo, D.; Psychogios, N.; Dejam, A.; Larson, M.G.; Vasan, R.S.; Ghorbani, A.; O’Sullivan, J.; Cheng, S.; Rhee, E.P.; et al. 2-Aminoadipic acid is a biomarker for diabetes risk. J. Clin. Investig. 2013, 123, 4309–4317. [Google Scholar] [CrossRef]
- Lehmann, R.; Friedrich, T.; Krebiehl, G.; Sonntag, D.; Häring, H.-U.; Fritsche, A.; Hennige, A.M. Metabolic profiles during an oral glucose tolerance test in pregnant women with and without gestational diabetes. Exp. Clin. Endocrinol. Diabetes 2015, 123, 438–483. [Google Scholar] [CrossRef]
- Jovanovic, L.; Metzger, B.E.; Knopp, R.H.; Conley, M.R.; Park, E.; Lee, Y.J.; Simpson, J.L.; Holmes, L.; Aarons, J.H.; Mills, J.L. The Diabetes in Early Pregnancy Study: Beta-hydroxybutyrate levels in type 1 diabetic pregnancy compared with normal pregnancy. NICHD-Diabetes in Early Pregnancy Study Group (DIEP). National Institute of Child Health and Development. Diabetes Care 1998, 21, 1978–1984. [Google Scholar] [CrossRef] [PubMed]
- Jovanovic, L. Nutrition and pregnancy: The link between dietary intake and diabetes. Curr. Diabetes Rep. 2004, 4, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Nahavandi, S.; Seah, J.; Shub, A.; Houlihan, C.; Ekinci, E.I. Biomarkers for Macrosomia Prediction in Pregnancies Affected by Diabetes. Front. Endocrinol. 2018, 9, 407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryckman, K.K.; Donovan, B.M.; Fleener, D.K.; Bedell, B.; Borowski, K.S. Pregnancy-Related Changes of Amino Acid and Acylcarnitine Concentrations: The Impact of Obesity. AJP Rep. 2016, 6, e329–e336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schoderbeck, M.; Auer, B.; Legenstein, E.; Genger, H.; Sevelda, P.; Salzer, H.; Marz, R.; Lohninger, A. Pregnancy-related changes of carnitine and acylcarnitine concentrations of plasma and erythrocytes. J. Perinat. Med. 1995, 23, 477–485. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.; Sun, Q.; Liang, L.; Clash, C.; Zhang, C.; Hong, X.; Ji, Y.; Radovick, S.; Pearson, C.; Bartell, T.R.; et al. Inter-generational link of obesity in term and preterm births: Role of maternal plasma acylcarnitines. Int. J. Obes. 2019, 43, 1967–1977. [Google Scholar] [CrossRef]
- Zhu, Y.; Li, M.; Rahman, M.L.; Hinkle, S.N.; Wu, J.; Weir, N.L.; Lin, Y.; Yang, H.; Tsai, M.Y.; Ferrara, A.; et al. Plasma phospholipid n-3 and n-6 polyunsaturated fatty acids in relation to cardiometabolic markers and gestational diabetes: A longitudinal study within the prospective NICHD Fetal Growth Studies. PLoS Med. 2019, 16, e1002910. [Google Scholar] [CrossRef]
- Pusl, T.; Beuers, U. Intrahepatic cholestasis of pregnancy. Orphanet J. Rare Dis. 2007, 2, 26. [Google Scholar] [CrossRef] [Green Version]
- Brites, D. Intrahepatic cholestasis of pregnancy: Changes in maternal-fetal bile acid balance and improvement by ursodeoxycholic acid. Ann. Hepatol. 2002, 1, 20–28. [Google Scholar] [CrossRef]
- Gottlieb, A.; Canbay, A. Why Bile Acids Are So Important in Non-Alcoholic Fatty Liver Disease (NAFLD) Progression. Cells 2019, 8, 1358. [Google Scholar] [CrossRef]
- Mantovani, A.; Byrne, C.D.; Bonora, E.; Targher, G. Nonalcoholic Fatty Liver Disease and Risk of Incident Type 2 Diabetes: A Meta-analysis. Diabetes Care 2018, 41, 372–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huynh, J.; Xiong, G.; Bentley-Lewis, R. Systematic review A systematic review of metabolite profiling in gestational diabetes mellitus. Diabetologia 2014, 57, 2453–2464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trak-Fellermeier, M.A.; Campos, M.; Meléndez, M.; Pomeroy, J.; Palacios, C.; Rivera-Viñas, J.; Méndez, K.; Febo, I.; Willett, W.; Gillman, M.W.; et al. PEARLS randomized lifestyle trial in pregnant Hispanic women with overweight/obesity: Gestational weight gain and offspring birthweight. Diabetes Metab. Syndr. Obes. 2019, 12, 225–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lagiou, P.; Tamimi, R.M.; Mucci, L.A.; Adami, H.-O.; Hsieh, C.-C.; Trichopoulos, D. Diet during pregnancy in relation to maternal weight gain and birth size. Eur. J. Clin. Nutr. 2004, 58, 231–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olson, C.M.; Strawderman, M.S.; Reed, R.G. Efficacy of an intervention to prevent excessive gestational weight gain. Am. J. Obstet. Gynecol. 2004, 191, 530–536. [Google Scholar] [CrossRef] [PubMed]
- Stuebe, A.M.; Oken, E.; Gillman, M.W. Associations of diet and physical activity during pregnancy with risk for excessive gestational weight gain. Am. J. Obstet. Gynecol. 2009, 201, 58.e1–58.e8. [Google Scholar] [CrossRef] [Green Version]
- Izadi, V.; Tehrani, H.; Haghighatdoost, F.; Dehghan, A.; Surkan, P.J.; Azadbakht, L. Adherence to the DASH and Mediterranean diets is associated with decreased risk for gestational diabetes mellitus. Nutrition 2016, 32, 1092–1096. [Google Scholar] [CrossRef]
- Assaf-Balut, C.; Garcia de la Torre, N.; Durán, A.; Fuentes, M.; Bordiú, E.; del Valle, L.; Valerio, J.; Familiar, C.; Jiménez, I.; Herraiz, M.A.; et al. Medical nutrition therapy for gestational diabetes mellitus based on Mediterranean Diet principles: A subanalysis of the St Carlos GDM Prevention Study. BMJ Open Diabetes Res. Care 2018, 6, e000550. [Google Scholar] [CrossRef] [Green Version]
- Torres, R.; Soltero, S.; Trak, M.A.; Tucker, C.M.; Mendez, K.; Campos, M.; Willett, W.; Melendez, M.; Gillman, M.W.; Franks, P.W.; et al. Lifestyle modification intervention for overweight and obese Hispanic pregnant women: Development, implementation, lessons learned and future applications. Contemp. Clin. Trials Commun. 2016, 3, 111–116. [Google Scholar] [CrossRef] [Green Version]
- Clifton, R.G.; Evans, M.; Cahill, A.G.; Franks, P.W.; Gallagher, D.; Phelan, S.; Pomeroy, J.; Redman, L.M.; Van Horn, L. LIFE-Moms Research Group Design of lifestyle intervention trials to prevent excessive gestational weight gain in women with overweight or obesity. Obesity 2016, 24, 305–313. [Google Scholar] [CrossRef]
- Metzger, B.E.; Gabbe, S.G.; Persson, B.; Lowe, L.P.; Dyer, A.R.; Oats, J.J.N.; Buchanan, T.A. International Association of Diabetes and Pregnancy Study Groups Recommendations on the Diagnosis and Classification of Hyperglycemia in Pregnancy: Response to Weinert. Diabetes Care 2010, 33, e98. [Google Scholar] [CrossRef] [Green Version]
- Tucker, K.L.; Maras, J.; Champagne, C.; Connell, C.; Goolsby, S.; Weber, J.; Zaghloul, S.; Carithers, T.; Bogle, M.L. A regional food-frequency questionnaire for the US Mississippi Delta. Public Health Nutr. 2005, 8, 87–96. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Z.; Liu, F.; Li, S. Metabolic Adaptations in Pregnancy: A Review. Ann. Nutr. Metab. 2017, 70, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Rodrigo, N.; Glastras, S.J. The Emerging Role of Biomarkers in the Diagnosis of Gestational Diabetes Mellitus. J. Clin. Med. 2018, 7, 120. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Intervention (N = 13) | Standard Care (N = 16) |
|---|---|---|
| Age at randomization, years | * 30.7 ± 5.3 | * 25.6 ± 4.8 |
| Body mass index, kg/m2 | 34.2 ± 7.5 | 36.2 ± 6.8 |
| Educational level | ||
| High school education/diploma or less | 6 (46) | 8 (50) |
| College education | 7 (54) | 8 (50) |
| Total annual family income | ||
| ≤$9999 | 5 (38.5) | 8 (50) |
| $10,000–$19,999 | 5 (38.5) | 5 (31) |
| ≥$20,000 | 3 (23) | 3 (19) |
| Marital Status | ||
| Married/living with a partner | 8 (62) | 14 (87.5) |
| Single/separated/divorced/widowed | 5 (38) | 2 (12.5) |
| Current Smoking | 0 (0) | 0 (0) |
| Any alcohol intake during pregnancy | 1 (7.7) | 0 (0) |
| Parous | 9 (69) | 11 (69) |
| Gestational Diabetes at 24 weeks | 2 (15) | 3 (19) |
| Fasting glucose (mg/dL) | * 95.5 ± 7.6 | * 90.5 ± 4.5 |
| Total energy intake, kcal/day 2 | 2501 ± 873 | 2523 ± 945 |
| Metabolite | HMDB ID | Biological Description | Early Pregnancy 1 | Mid-Pregnancy 2 | ||||
|---|---|---|---|---|---|---|---|---|
| Intervention Mean (SD) | Control Mean (SD) | p-Value | Intervention Mean (SD) | Control Mean (SD) | p-Value | |||
| myristoleoylcarnitine (C14:1) * | NA | Fatty Acid Metabolism (Acyl Carnitine, Monounsaturated) | −1.7 (0.7) | −1.5 (0.5) | 0.50 | −1.7 (0.4) | −0.9 (0.4) | ** 0.0003 |
| palmitoleoylcarnitine (C16:1) * | HMDB00641 | Fatty Acid Metabolism (Acyl Carnitine, Monounsaturated) | −1.6 (0.4) | −1.5 (0.5) | 0.67 | −1.8 (0.4) | −1.0 (0.4) | ** 0.0008 |
| leucine | NA | Leucine, Isoleucine and Valine Metabolism | −1.2 (1.0) | −1.6 (0.3) | 0.31 | −1.8 (0.2) | −1.3 (0.3) | 0.004 |
| linoleoylcarnitine (C18:2) * | HMDB06469 | Fatty Acid Metabolism (Acyl Carnitine, Polyunsaturated) | −1.0 (0.5) | −1.2 (0.5) | 0.51 | −1.4 (0.6) | −0.6 (0.4) | 0.009 |
| 5-dodecenoylcarnitine (C12:1) | HMDB13326 | Fatty Acid Metabolism (Acyl Carnitine, Monounsaturated) | −1.7 (0.5) | −1.5 (0.8) | 0.52 | −1.7 (0.7) | −0.8 (0.4) | 0.01 |
| myristoylcarnitine (C14) | HMDB05066 | Fatty Acid Metabolism (Acyl Carnitine, Long Chain Saturated) | −1.4 (0.6) | −1.3 (0.6) | 0.68 | −1.6 (0.5) | −0.9 (0.7) | 0.02 |
| palmitoylcarnitine (C16) | HMDB00222 | Fatty Acid Metabolism (Acyl Carnitine, Long Chain Saturated) | −1.1 (0.5) | −1.2 (0.7) | 0.60 | −1.4 (0.7) | −0.6 (0.5) | 0.02 |
| 3-hydroxybutyrate (BHBA) | HMDB00929 | Ketone Bodies | −2.2 (0.6) | −2.0 (0.6) | 0.40 | −2.0 (0.6) | −1.3 (0.5) | 0.02 |
| oleoylcarnitine (C18:1) | HMDB05065 | Fatty Acid Metabolism (Acyl Carnitine, Monounsaturated) | −1.2 (0.5) | −1.3 (0.7) | 0.81 | −1.5 (0.8) | −0.6 (0.4) | 0.02 |
| asparagine | HMDB00168 | Alanine and Aspartate Metabolism | −0.7 (0.8) | −1.1 (0.6) | 0.31 | −1.4 (0.5) | −0.7 (0.7) | 0.02 |
| glycodeoxycholate | HMDB00631 | Secondary Bile Acid Metabolism | 0.5 (1.0) | 0.8 (0.6) | 0.53 | 0.6 (0.4) | −0.04 (0.7) | 0.03 |
| tryptophan | HMDB00357 | Tryptophan Metabolism | −0.3 (0.9) | −0.9 (0.7) | 0.23 | −0.5 (0.4) | −0.9 (0.4) | 0.03 |
| glutamine | NA | Glutamate Metabolism | −1.2 (0.4) | −1.1 (0.8) | 0.62 | −1.2 (0.4) | −0.7 (0.6) | 0.04 |
| adrenate (22:4n6) | HMDB02226 | Long Chain Polyunsaturated Fatty Acid (n3 and n6) | −2.2 (1.3) | −1.6 (0.8) | 0.24 | −1.7 (0.3) | −0.9 (1.2) | 0.07 |
| isoleucine | HMDB00172 | Leucine, Isoleucine and Valine Metabolism | −1.4 (0.9) | −1.6 (0.3) | 0.56 | −1.7 (0.3) | −1.4 (0.3) | 0.07 |
| linoleate (18:2n6) | HMDB00673 | Long Chain Polyunsaturated Fatty Acid (n3 and n6) | −2.4 (1.3) | −2.2 (0.5) | 0.61 | −2.0 (0.5) | −1.4 (0.8) | 0.08 |
| ornithine | HMDB03374 | Urea cycle; Arginine and Proline Metabolism | −0.4 (0.8) | −0.3 (0.5) | 0.85 | −0.7 (0.4) | −0.4 (0.5) | 0.08 |
| glycocholate | HMDB00138 | Primary Bile Acid Metabolism | 0.8 (0.6) | 0.6 (0.7) | 0.51 | 0.5 (0.8) | −0.2 (0.6) | 0.09 |
| linolenate [alpha or gamma; (18:3n3 or 6)] | HMDB03073 | Long Chain Polyunsaturated Fatty Acid (n3 and n6) | −2.4 (1.1) | −2.1 (0.5) | 0.63 | −1.9 (0.4) | −1.4 (0.8) | 0.09 |
| pyruvate | HMDB00243 | Glycolysis, Gluconeogenesis, and Pyruvate Metabolism | 0.7 (1.2) | 0.5 (0.9) | 0.81 | 0.6 (0.6) | 0.1 (0.5) | 0.09 |
| hexanoylcarnitine (C6) | HMDB00705 | Fatty Acid Metabolism (Acyl Carnitine, Medium Chain) | −1.5 (0.4) | −1.6 (0.5) | 0.66 | −1.4 (0.5) | −1.0 (0.5) | 0.10 |
| oleate/vaccenate (18:1) | NA | Long Chain Monounsaturated Fatty Acid | −2.4 (1.1) | −2.2 (0.6) | 0.66 | −2.0 (0.6) | −1.4 (0.8) | 0.10 |
| acetylcarnitine (C2) | HMDB00201 | Fatty Acid Metabolism (Acyl Carnitine, Short Chain) | −1.6 (0.6) | −1.6 (0.6) | 0.93 | −1.5 (0.5) | −1.2 (0.4) | 0.12 |
| glycochenodeoxycholate | HMDB00637 | Primary Bile Acid Metabolism | 1.0 (1.0) | 0.8 (0.7) | 0.62 | 0.6 (0.5) | 0.1 (0.7) | 0.12 |
| palmitoleate (16:1n7) | HMDB03229 | Long Chain Monounsaturated Fatty Acid | −2.4 (1.2) | −2.2 (0.6) | 0.65 | −1.8 (0.5) | −1.4 (0.6) | 0.12 |
| laurylcarnitine (C12) | HMDB02250 | Fatty Acid Metabolism (Acyl Carnitine, Medium Chain) | −1.6 (0.6) | −1.5 (0.8) | 0.87 | −1.2 (0.6) | −0.8 (0.4) | 0.13 |
| tetradecadienedioate (C14:2-DC) * | NA | Fatty Acid, Dicarboxylate | −1.7 (0.5) | −1.1 (0.4) | 0.02 | −1.0 (0.2) | −0.7 (0.5) | 0.13 |
| myristoleate (14:1n5) | HMDB02000 | Long Chain Monounsaturated Fatty Acid | −2.3 (0.9) | −2.2 (0.7) | 0.77 | −1.8 (0.6) | −1.3 (0.7) | 0.17 |
| valine | HMDB00883 | Leucine, Isoleucine and Valine Metabolism | −0.5 (0.8) | −1.1 (0.6) | 0.15 | −1.1 (0.4) | −0.8 (0.6) | 0.18 |
| methionine | HMDB00696 | Methionine, Cysteine, SAM and Taurine Metabolism | −1.3 (1.0) | −1.7 (0.6) | 0.27 | −1.7 (0.4) | −1.4 (0.4) | 0.19 |
| lactate | HMDB00190 | Glycolysis, Gluconeogenesis, and Pyruvate Metabolism | 0.9 (1.2) | 0.7 (1.4) | 0.70 | 0.3 (0.8) | 0.8 (1.0) | 0.21 |
| decanoylcarnitine (C10) | HMDB00651 | Fatty Acid Metabolism (Acyl Carnitine, Medium Chain) | −1.3 (0.4) | −1.3 (0.5) | 0.92 | −1.1 (0.7) | −0.7 (0.6) | 0.21 |
| dimethylarginine (SDMA + ADMA) | HMDB01539 | Urea cycle; Arginine and Proline Metabolism | −0.3 (0.8) | −0.6 (0.8) | 0.57 | −1.2 (0.3) | −0.9 (0.5) | 0.22 |
| octanoylcarnitine (C8) | HMDB00791 | Fatty Acid Metabolism (Acyl Carnitine, Medium Chain) | −1.3 (0.4) | −1.3 (0.5) | 0.98 | −1.1 (0.6) | −0.7 (0.5) | 0.23 |
| alanine | HMDB00161 | Alanine and Aspartate Metabolism | 0.3 (0.8) | −0.3 (0.7) | 0.11 | 0.1 (0.6) | −0.2 (0.5) | 0.24 |
| arginine | HMDB00517 | Urea cycle; Arginine and Proline Metabolism | −0.2 (1.4) | −0.9 (0.6) | 0.27 | −0.4 (0.7) | −0.8 (0.6) | 0.25 |
| phenylalanine | HMDB00159 | Phenylalanine Metabolism | −0.7 (1.4) | −1.2 (0.6) | 0.45 | −1.4 (0.4) | −1.1 (0.6) | 0.25 |
| docosapentaenoate (n6 DPA; 22:5n6) | HMDB01976 | Long Chain Polyunsaturated Fatty Acid (n3 and n6) | −2.0 (0.7) | −1.3 (0.5) | 0.06 | −1.3 (0.5) | −1.0 (0.8) | 0.33 |
| isocitrate | HMDB00193 | TCA Cycle | −0.6 (0.6) | −0.6 (0.5) | 0.89 | −0.2 (0.4) | 0.2 (1.1) | 0.35 |
| threonine | HMDB00167 | Glycine, Serine and Threonine Metabolism | −0.6 (0.8) | −1.1 (0.4) | 0.21 | −0.9 (0.3) | −0.8 (0.2) | 0.37 |
| eicosapentaenoate (EPA; 20:5n3) | HMDB01999 | Long Chain Polyunsaturated Fatty Acid (n3 and n6) | −1.7 (0.7) | −1.3 (0.6) | 0.32 | −1.5 (0.5) | −1.2 (0.9) | 0.37 |
| lysine | HMDB00182 | Lysine Metabolism | −0.5 (0.6) | −0.5 (0.6) | 0.90 | −0.8 (0.3) | −0.7 (0.4) | 0.39 |
| uridine | HMDB00296 | Pyrimidine Metabolism, Uracil containing | −0.2 (0.7) | 0.6 (0.6) | 0.03 | 0.4 (0.5) | 0.1 (0.7) | 0.39 |
| palmitate (16:0) | HMDB00220 | Long Chain Saturated Fatty Acid | −2.4 (1.2) | −2.1 (0.6) | 0.58 | −1.8 (0.7) | −1.5 (0.9) | 0.41 |
| glycine | HMDB00123 | Glycine, Serine and Threonine Metabolism | −0.4 (0.8) | −0.8 (0.5) | 0.28 | −0.9 (0.6) | −0.7 (0.8) | 0.45 |
| stearoylcarnitine (C18) | HMDB00848 | Fatty Acid Metabolism (Acyl Carnitine, Long Chain Saturated) | −0.5 (0.8) | −0.6 (1.2) | 0.78 | −0.6 (0.8) | −0.3 (0.7) | 0.46 |
| betaine | HMDB00043 | Glycine, Serine and Threonine Metabolism | 1.1 (0.7) | 0.5 (0.6) | 0.08 | 0.1 (0.4) | 0.3 (0.6) | 0.46 |
| stearate (18:0) | HMDB00827 | Long Chain Saturated Fatty Acid | −2.1 (1.1) | −1.9 (0.5) | 0.80 | −1.7 (1.1) | −1.3 (1.0) | 0.47 |
| 2-aminoadipate | HMDB00510 | Lysine Metabolism | −0.7 (0.7) | −0.1 (1.1) | 0.20 | −0.6 (1.0) | −0.2 (0.9) | 0.50 |
| aspartate | HMDB00191 | Alanine and Aspartate Metabolism | 0.3 (1.4) | 0.001 (0.8) | 0.60 | −0.3 (0.8) | −0.1 (0.8) | 0.51 |
| quinolinate | HMDB00232 | Nicotinate and Nicotinamide Metabolism | −0.1 (0.6) | −0.3 (0.6) | 0.54 | −0.4 (0.3) | −0.3 (0.4) | 0.52 |
| histidine | HMDB00177 | Histidine Metabolism | −0.8 (0.7) | −1.0 (0.8) | 0.51 | −1.1 (0.7) | −0.9 (0.3) | 0.54 |
| docosapentaenoate (n3 DPA; 22:5n3) | HMDB06528 | Long Chain Polyunsaturated Fatty Acid (n3 and n6) | −2.4 (0.9) | −1.8 (0.6) | 0.18 | −1.6 (0.6) | −1.4 (0.8) | 0.55 |
| citrulline | HMDB00094 | Urea cycle; Arginine and Proline Metabolism | −1.5 (0.4) | −1.4 (0.7) | 0.78 | −1.6 (0.7) | −1.4 (0.5) | 0.59 |
| urate | HMDB00289 | Purine Metabolism, (Hypo)Xanthine/Inosine containing | −0.1 (0.4) | −0.3 (0.6) | 0.35 | −0.1 (0.7) | −0.2 (0.6) | 0.64 |
| fructose | HMDB00660 | Fructose, Mannose and Galactose Metabolism | 1.1 (1.3) | 0.2 (1.8) | 0.21 | 0.8 (0.8) | 0.6 (1.0) | 0.64 |
| tyrosine | HMDB00158 | Tyrosine Metabolism | −1.0 (1.4) | −1.0 (0.8) | 0.98 | −0.9 (1.1) | −1.1 (1.0) | 0.66 |
| proline | HMDB00162 | Urea cycle; Arginine and Proline Metabolism | −0.2 (1.0) | −0.8 (0.5) | 0.17 | −0.7 (0.3) | −0.7 (0.2) | 0.68 |
| hypoxanthine | HMDB00157 | Purine Metabolism, (Hypo)Xanthine/Inosine containing | 1.4 (1.7) | 0.5 (1.5) | 0.30 | 0.2 (0.8) | 0.02 (1,0) | 0.69 |
| arachidonate (20:4n6) | HMDB01043 | Long Chain Polyunsaturated Fatty Acid (n3 and n6) | −1.4 (1.1) | −1.0 (0.7) | 0.37 | −1.1 (0.8) | −0.9 (1.0) | 0.75 |
| taurine | HMDB00251 | Methionine, Cysteine, SAM and Taurine Metabolism | 0.4 (1.3) | 0.3 (0.8) | 0.85 | −0.1 (1.2) | 0.1 (1.1) | 0.78 |
| trans-4-hydroxyproline | HMDB00725 | Urea cycle; Arginine and Proline Metabolism | −0.8 (0.3) | −0.9 (0.4) | 0.65 | −0.4 (0.6) | −0.4 (0.5) | 0.80 |
| glutamate | HMDB00148 | Glutamate Metabolism | 0.1 (1.3) | −0.2 (0.9) | 0.59 | −0.3 (0.9) | −0.3 (0.8) | 0.87 |
| serine | HMDB00187 | Glycine, Serine and Threonine Metabolism | −0.6 (1.1) | −0.8 (0.7) | 0.64 | −0.9 (1.0) | −1.0 (0.6) | 0.89 |
| arachidonoylcarnitine (C20:4) | NA | Fatty Acid Metabolism (Acyl Carnitine, Polyunsaturated) | −0.6 (0.4) | −0.9 (0.9) | 0.39 | −0.8 (1.0) | −0.7 (0.6) | 0.91 |
| Fasting | 30 min | 60 min | 120 min | ||||
|---|---|---|---|---|---|---|---|
| β (SE) | p Value | β (SE) | p Value | β (SE) | p Value | ||
| Early pregnancy | |||||||
| PC1 | Ref. | −1.9 (0.7) | 0.005 | −5.8 (0.7) | <0.001 | −9.4 (0.7) | <0.001 |
| PC2 | Ref. | −0.9 (0.7) | 0.24 | −1.8 (0.7) | 0.02 | −1.4 (0.7) | 0.05 |
| Mid-Pregnancy | |||||||
| PC1 | Ref. | - | - | −4.7 (1.0) | <0.001 | −7.7 (1.0) | <0.001 |
| PC2 | Ref. | - | - | 0.9 (0.8) | 0.29 | 1.6 (0.8) | 0.06 |
| Early and Mid-Pregnancy | |||||||
| PC1 | Ref. | −1.2 (0.6) | 0.04 | −5.4 (0.5) | <0.001 | −8.8 (0.5) | <0.001 |
| PC2 | Ref. | 0.1 (0.6) | 0.85 | 0.8 (0.5) | 0.10 | 0.3 (0.5) | 0.60 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haslam, D.E.; Li, J.; Liang, L.; Martinez, M.; Palacios, C.; Trak-Fellermeier, M.A.; Franks, P.W.; Joshipura, K.; Bhupathiraju, S.N. Changes in Metabolites During an Oral Glucose Tolerance Test in Early and Mid-Pregnancy: Findings from the PEARLS Randomized, Controlled Lifestyle Trial. Metabolites 2020, 10, 284. https://doi.org/10.3390/metabo10070284
Haslam DE, Li J, Liang L, Martinez M, Palacios C, Trak-Fellermeier MA, Franks PW, Joshipura K, Bhupathiraju SN. Changes in Metabolites During an Oral Glucose Tolerance Test in Early and Mid-Pregnancy: Findings from the PEARLS Randomized, Controlled Lifestyle Trial. Metabolites. 2020; 10(7):284. https://doi.org/10.3390/metabo10070284
Chicago/Turabian StyleHaslam, Danielle E., Jun Li, Liming Liang, Marijulie Martinez, Cristina Palacios, Maria A. Trak-Fellermeier, Paul W. Franks, Kaumudi Joshipura, and Shilpa N. Bhupathiraju. 2020. "Changes in Metabolites During an Oral Glucose Tolerance Test in Early and Mid-Pregnancy: Findings from the PEARLS Randomized, Controlled Lifestyle Trial" Metabolites 10, no. 7: 284. https://doi.org/10.3390/metabo10070284