Examining Trans-Provincial Diagnosis of Rare Diseases in China: The Importance of Healthcare Resource Distribution and Patient Mobility


Abstract
:1. Introduction
2. Materials and Methods
3. Results
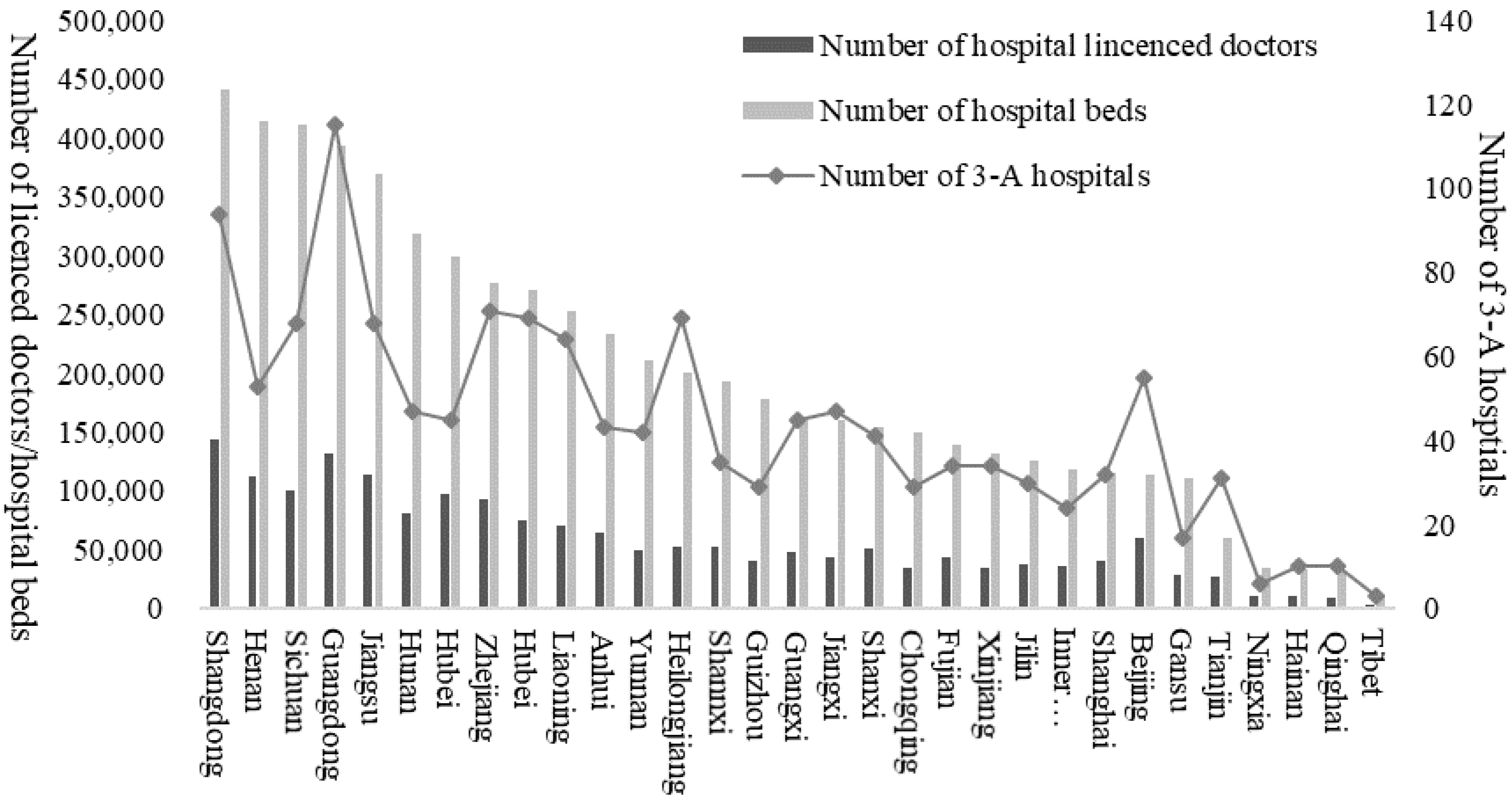
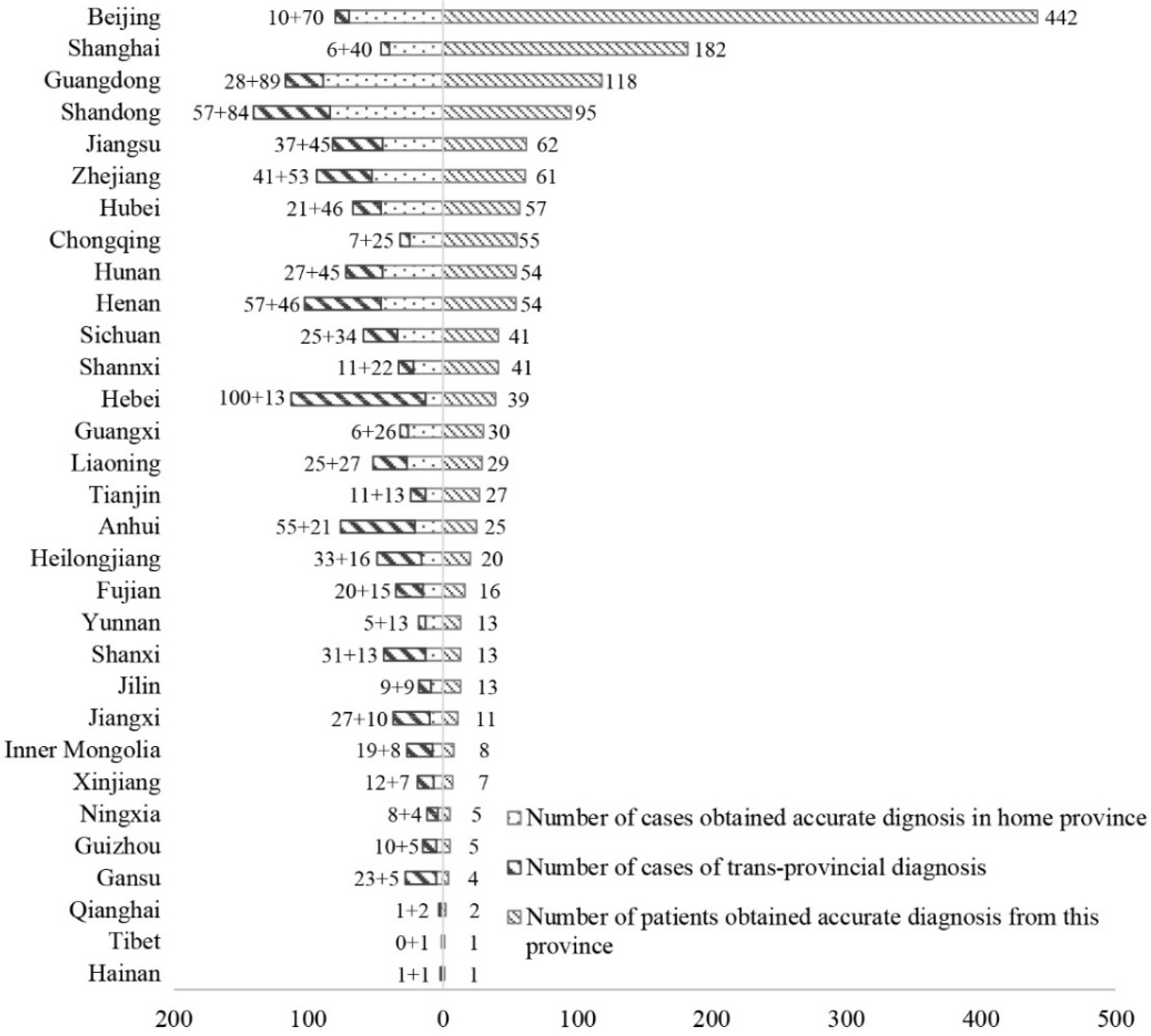
3.1. Descriptive Analysis
3.2. Factors Affecting the Trans-Provincial Diagnosis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Disease | Prevalence | Data Source of Prevalence | |
|---|---|---|---|
| Extremely Rare (Prevalence < 1/100,000) | |||
| 1 | 1q44 microdeletion syndrome | <1/1,000,000 | orpha.net |
| 2 | Acute transverse myelitis | 1/1,000,000 ~ 1/250,000 | orpha.net |
| 3 | Alexander disease | 1/2,700,000 | orpha.net |
| 4 | Atypical hemolytic uremic syndrome-AHUS | 1–9/1,000,000 | orpha.net |
| 5 | Bartter syndrome | 1/1,000,000 | orpha.net |
| 6 | Erythrokeratoderma | 200 cases reported | orpha.net |
| 7 | GM1 gangliosidosis | 1/100,000–1/200,000 in live births | orpha.net |
| 8 | Growth hormone deficiency | 1–9/1,000,000 | Stanley T. (2012). Diagnosis of growth hormone deficiency in childhood. Current opinion in endocrinology, diabetes, and obesity, 19(1), 47–52. doi:10.1097/MED.0b013e32834ec952 |
| 9 | Lymphangioleio-myomatosis | 1–9 /1,000,000 | orpha.net |
| 10 | Massive osteolysis/Gorham-Stout disease | 300 cases reported | orpha.net |
| 11 | Metachromatic leukodystrophy | 1–9 /1,000,000 | orpha.net |
| 12 | Mitochondrial encephalopathy | 1–9/1,000,000 | orpha.net |
| 13 | Niemann-Pick disease | <1/1,000,000 | orpha.net |
| 14 | Peutz–Jeghers syndrome | 1–9/1,000,000 | orpha.net |
| 15 | Spondyloepiphyseal Dysplasia Congenita | 1 per 100,000 live births | orpha.net |
| 16 | Triple-A syndrome (Allgrove syndrome) | <1/1,000,000 | orpha.net |
| Rare (1/10,000 < Prevalence < 1/100,000) | |||
| 17 | Acromegaly | 1–9/100,000 | orpha.net |
| 18 | Adrenal Hypoplasia Congenita | less than 1/12,500 births | AvRuskin, T., Krishnan, N., & Juan, C. (2004). Congenital Adrenal Hypoplasia and Male Pseudohermaphroditism Due to DAX1 Mutation, SF1 Mutation or Neither: A Patient Report. Journal of Pediatric Endocrinology and Metabolism, 17(8), 1125–1132. |
| 19 | Albinism | 1/10,000–1/20,000 | Mártinez-García, M. and Montoliu, L. (2013), Albinism in Europe. J Dermatol, 40: 319–324. doi:10.1111/1346-8138.12170 |
| 20 | Amyotrophic lateral sclerosis | 1–9/100,000 | orpha.net |
| 21 | Angelman syndrome | 1–9/100,000 | orpha.net |
| 22 | Anti-Neutrophil cytoplasmic antibody-associated vasculitis | 4.6–18.4/100,000 | Watts, R., Mahr, A., Mohammad, A., Gatenby, P., Basu, N., & Flores-Suárez, L. (2015). Classification, epidemiology and clinical subgrouping of antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis. Nephrology Dialysis Transplantation, 30(Suppl1), I14–I22. |
| 23 | Behcet’s disease | 1–9/100,000 | orpha.net |
| 24 | Cerebral palsy | 1.5–4/1000 in live births | Stavsky, M., Mor, O., Mastrolia, S., Greenbaum, S., Than, N., & Erez, O. (2017). Cerebral Palsy-Trends in Epidemiology and Recent Development in Prenatal Mechanisms of Disease, Treatment, and Prevention. Frontiers in Pediatrics, 5, 21. |
| 25 | Congenital Adrenal Hyperplasia | 1–9/100,000 | orpha.net |
| 26 | Cri-du-chat syndrome | 1/20,000-1/50,000 newborns | orpha.net |
| 27 | Crohn’s disease | 1.2-21.2/100,000 | Prideaux, L., Kamm, M. A., De Cruz, P. P., Chan, F. K., & Ng, S. C. (2012). Inflammatory bowel disease in Asia: a systematic review. Journal of gastroenterology and hepatology, 27(8), 1266–1280. |
| 28 | Duchenne Muscular Dystrophy | 1–9/100,000 | orpha.net |
| 29 | Eisenmenger’s syndrome | 1–9/1,000,000 | orpha.net |
| 30 | Epidermolysis bullosa | 1–9 /1,000,000 | orpha.net |
| 31 | Fabry disease | 1/100,000 | Branton, M. H., Schiffmann, R., Sabnis, etc. (2002). Natural history of Fabry renal disease: influence of α-galactosidase A activity and genetic mutations on clinical course. Medicine, 81(2), 122–138. |
| 32 | Gaucher disease | 1–9/100,000 | orpha.net |
| 33 | Glycogen storage disease due to acid maltase deficiency | 1–9/100,000 | orpha.net |
| 34 | Granulomatosis with Polyangiitis | 1–9/100,000 | orpha.net |
| 35 | Hemophilia | 1–9/100,000 | orpha.net |
| 36 | Hepatolenticular degeneration/Wilson disease | 1–9/100,000 | orpha.net |
| 37 | Huntington’s disease | 1–9/100,000 | orpha.net |
| 38 | Ichthyosis | average of subtypes | orpha.net |
| 39 | Idiopathic Hypogonadotropic Hypogonadism | 1/4000–1/10,000 in males, and 2 to 5 times less frequent in females | Silveira, L. G., & Latronico, A. C. (2013). Approach to the Patient With Hypogonadotropic Hypogonadism. The Journal of Clinical Endocrinology & Metabolism, 98(5), 1781–1788. |
| 40 | Immunologic thrombocytopenic purpura | 5/100,000 | Fogarty, P. F., & Segal, J. B. (2007). The epidemiology of immune thrombocytopenic purpura. Current opinion in hematology, 14(5), 515–519. |
| 41 | Kallmann Syndrome, KS | 1–9/100,000 | orpha.net |
| 42 | Mucolipidosis type IV | 1/40,000 births | orpha.net |
| 43 | Mucopolysaccharidosis | 1–9/100,000 | orpha.net |
| 44 | Multiple Sclerosis | 1–2/100,000 | Cheng, Q, Cheng, X-J, & Jiang, G-X. (2009). Multiple sclerosis in China—history and future. Multiple Sclerosis, 15(6), 655–660. |
| 45 | Myasthenia Gravis | 1–9/100,000 | orpha.net |
| 46 | Neuromyelitis optica | 1–9/100,000 | orpha.net |
| 47 | Noonan syndrome | 1/1000–1/2500 live births | orpha.net |
| 48 | Ornithine transcarbamylase deficiency | 1–9/100,000 | orpha.net |
| 49 | Prader-Willi syndrome | 1–9/100,000 | orpha.net |
| 50 | Pseudoachondroplasia | 1–9/100,000 | orpha.net |
| 51 | Pseudomyxoma peritonei | 1–9/100,000 | orpha.net |
| 52 | Pulmonary hypertension | 1–9/100,000 | orpha.net |
| 53 | Spinal muscular atrophy | 1–9/100,000 | orpha.net |
| 54 | Spinocerebellar ataxias | 1–9/100,000 | orpha.net |
| 55 | Systemic Vasculitis | 1–2/100,000 | Lane, S., Watts, E., & Scott, R. (2005). Epidemiology of systemic vasculitis. Current Rheumatology Reports, 7(4), 270–275. |
| 56 | Takayasu arteritis | 1–9/100,000 | orpha.net |
| Somewhat rare (Prevalence >1/10,000) | |||
| 57 | Charcot-Marie-Tooth disease | 1–5/10,000 | orpha.net |
| 58 | Fuchs’ syndrome | 3.7–9.2% in patients over 50 years of age | Pilger, Daniel, Brockmann, Claudia, Maier, Anna-Karina B., & Bertelmann, Eckart. (2019). Predictive Factors for Clinical Outcomes after Primary Descemet’s Membrane Endothelial Keratoplasty for Fuchs’ Endothelial Dystrophy. Current Eye Research, 44(2), 147–153. |
| 59 | Hereditary hemorrhagic telangiectasia | 1–5/10,000 | orpha.net |
| 60 | Hyperammonemia | 1–5/10,000 | orpha.net |
| 61 | Hypopituitarism | 4.5/10,000 | Aimaretti G, Kreitschmann-Andermahr I, Stalla GK, Ghigo E (2007). Hypopituitarism. Lancet. 369 (9571): 1461–70. |
| 62 | Isolated spina bifida | 1–5/10,000 | orpha.net |
| 63 | Keratoconus | 5.4/10,000 | Gokhale N. S. (2013). Epidemiology of keratoconus. Indian journal of ophthalmology, 61(8), 382–383. doi:10.4103/0301-4738.116054 |
| 64 | Klinefelter syndrome | 1/1,000 | Wattendorf DJ, Muenke M. (2005) Klinefelter syndrome. Am Fam Physician. 72(11):2259–62. |
| 65 | Marfan Syndrome | 1–5/10,000 | orpha.net |
| 66 | Neurofibromatosis | 1–5/10,000 | orpha.net |
| 67 | Osteogenesis imperfecta | 1–5/10,000 | orpha.net |
| 68 | Pemphigus vulgaris | 1–5/10,000 | orpha.net |
| 69 | Primary adrenal insufficiency/Addison’s disease | 1–5/10,000 | orpha.net |
| 70 | Stargardt disease | 1–5/10,000 | orpha.net |
| 71 | Systemic lupus erythematosus | 1–5/10,000 | orpha.net |
| 72 | Systemic sclerosis | 1–5/10,000 | orpha.net |
| 73 | Tuberous sclerosis complex | 1–5/10,000 | orpha.net |
| 74 | Turner syndrome | 1–5/10,000 | orpha.net |
| 75 | Uveitis | 1–5/10,000 | orpha.net |
References
- Austin, C.P.; Cutillo, C.M.; Lau, L.P.L.; Jonker, A.H.; Rath, A.; Julkowska, D.; Thomson, D.; Terry, S.F.; de Montleau, B.; Ardigò, D.; et al. Future of Rare Diseases Research 2017–2027: An IRDiRC Perspective. Clin. Transl. Sci. 2018, 11, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Esquivel-Sada, D.; Nguyen, M.T. Diagnosis of rare diseases under focus: Impacts for Canadian patients. J. Community Genet. 2018, 9, 37–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dawkins, H.J.; Draghia-Akli, R.; Lasko, P.; Lau, L.P.L.; Jonker, A.H.; Cutillo, C.M.; Rath, A.; Boycott, K.M.; Baynam, G.; Lochmuller, H.; et al. Progress in rare diseases research 2010–2016: An IRDiRC perspective. Clin. Transl. Sci. 2018, 11, 11. [Google Scholar] [CrossRef] [PubMed]
- Boycott, K.M.; Hartley, T.; Biesecker, L.G.; Gibbs, R.A.; Innes, A.M.; Riess, O.; Belmont, J.; Dunwoodie, S.L.; Jojic, N.; Lassmann, T.; et al. A Diagnosis for All Rare Genetic Diseases: The Horizon and the Next Frontiers. Cell 2019, 177, 32–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andersen, R.M. Revisiting the behavioral model and access to medical care: Does it matter? J. Health Soc. Behav. 1995, 36, 1–10. [Google Scholar] [CrossRef]
- Andersen, R.M. National health surveys and the behavioral model of health services use. Med. Care 2008, 46, 647–653. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.J.; Wang, Y.O.; Li, L.; Guo, J.J.; Wang, J.B. China’s first rare-disease registry is under development. Lancet 2011, 378, 769–770. [Google Scholar] [CrossRef]
- Han, J.; Cui, Y.; Zhou, X. Rare diseases research in China: Opportunities, challenges, and solutions. Intractable Rare Dis. Res. 2012, 1, 10–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feng, S.; Liu, S.; Zhu, C.; Gong, M.; Zhu, Y.; Zhang, S. National Rare Diseases Registry System of China and Related Cohort Studies: Vision and Roadmap. Hum. Gene Ther. 2018, 29, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.B.; Guo, J.J.; Yang, L.; Zhang, Y.D.; Sun, Z.Q.; Zhang, Y.J. Rare diseases and legislation in China. Lancet 2010, 375, 708–709. [Google Scholar] [CrossRef]
- Dong, D.; Wang, Y. Challenges of rare diseases in China. Lancet 2016, 387, 1906. [Google Scholar] [CrossRef] [Green Version]
- Yu, M.; He, S.; Wu, D.; Zhu, H.; Webster, C. Examining the Multi-Scalar Unevenness of High-Quality Healthcare Resources Distribution in China. Int. J. Environ. Res. Public Health 2019, 16, 2813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, J.; Shallcross, D. Geographic distribution of hospital beds throughout China: A county-level econometric analysis. Int. J. Equity Health 2016, 15, 179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.; Wan, G. Income polarization in China: Trends and changes. China Econ. Rev. 2015, 36, 58–72. [Google Scholar] [CrossRef]
- Ling, R.E.; Liu, F.; Lu, X.; Wang, W. Emerging issues in public health: A perspective on China’s healthcare system. Public Health 2011, 125, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Müller, A. Hukou and health insurance coverage for migrant workers. J. Curr. Chin. Aff. 2016, 45, 53–82. [Google Scholar] [CrossRef] [Green Version]
- Burns, L.R.; Liu, G.G. China’s Healthcare System and Reform; Cambridge University Press: Cambridge, UK, 2017. [Google Scholar]
- Balia, S.; Brau, R.; Marrocu, E. Interregional patient mobility in a decentralized healthcare system. Reg. Stud. 2018, 52, 388–402. [Google Scholar] [CrossRef]
- Eurordis. The Voice of 12,000 Patients. Experiences and Expectations of Rare Disease Patients on Diagnosis and Care in Europe; Eurordis: Paris, France, 2009. [Google Scholar]
- Glinos, I.A.; Baeten, R.; Helble, M.; Maarse, H. A typology of cross-border patient mobility. Health Place 2010, 16, 1145–1155. [Google Scholar] [CrossRef] [PubMed]
- Rosenmöller, M.; McKee, M.; Baeten, R. Patient Mobility in the European Union: Learning from Experience; World Health Organization: Copenhagen, Denmark, 2006. [Google Scholar]
- Lunt, N.; Mannion, R. Patient mobility in the global marketplace: A multidisciplinary perspective. Int. J. Health Policy Manag. 2014, 2, 155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asclepius. Annual Report on China’s Hospitals Competitiveness (2018–2019); Social Sciences Academic Press: Beijing, China, 2019. [Google Scholar]


| Adult | Child | |
|---|---|---|
| Trans-Provincial diagnosis | 47.6% | 46.5% |
| Age | 35.5(11.1) 1 | 6.0(4.7) |
| Female | 53.6% | 35.7% |
| Ethnic minority | 4.6% | 7.2% |
| Rarity of disease | ||
| Somewhat rare | 15.8% | 22.0% |
| Rare | 75.5% | 74.2% |
| Extremely rare | 8.7% | 3.8% |
| Level of patient’s family income in local city | ||
| Far below average | 24.3% | 27.9% |
| Below average | 39.7% | 41.9% |
| Average level | 32.6% | 26.9% |
| Above average | 3.2% | 3.4% |
| Far above average | 0.2% | 0.0% |
| City level | ||
| Centrally Administered cities | 12.9% | 9.8% |
| Provincial-Level cities 2 | 24.5% | 25.7% |
| Other common cities | 62.6% | 64.5% |
| Urban Hukou | 57.0% | 51.3% |
| Covered by UEBMI | 35.5% | — |
| Covered by BMIRUP | 53.6% | 78.8% |
| Patient’s dependency on assistive devices | ||
| No need | 8.6% | 15.6% |
| Occasionally | 7.5% | 9.8% |
| Sometimes | 10.2% | 11.4% |
| Usually | 18.6% | 12.0% |
| Always | 55.1% | 51.1% |
| Married patients | 62.0% | — |
| Number of other family members | 3.3(1.5) | 4.06(1.5) |
| Longest education years among family members | 12.0(4.2) | 11.18(4.6) |
| Time to Diagnosis (Years) | Number of Hospitals Visited Prior to Diagnosis | Presence of Misdiagnosis | |
|---|---|---|---|
| Adult | 0.092 ** | 0.081 ** | 0.080 ** |
| Child | 0.289 *** | 0.118 ** | 0.239 *** |
| Adult | Child | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | P | OR | 95% CI | P | |
| Demographic Characteristics of Patients | ||||||
| Age | 0.986 | 0.972–1.001 | 0.060 | 1.103 | 1.054–1.154 | <0.001 |
| Female | 0.856 | 0.657–1.116 | 0.251 | 0.703 | 0.466–1.062 | 0.094 |
| Ethnic minority | 1.087 | 0.571–2.069 | 0.799 | 0.942 | 0.430–2.064 | 0.881 |
| Rarity of disease | 1.410 | 1.070–1.858 | 0.015 | 1.335 | 0.876–2.034 | 0.178 |
| Healthcare Resources in Home Province | ||||||
| Number of 3-A hospitals | 0.973 | 0.963–0.983 | <0.001 | 0.973 | 0.956–0.990 | 0.003 |
| Number of hospital beds | 0.994 | 0.957–1.033 | 0.764 | 1.007 | 0.952–1.065 | 0.814 |
| Number of licensed doctors | 1.065 | 0.974–1.165 | 0.166 | 1.027 | 0.882–1.196 | 0.733 |
| Patient Mobility | ||||||
| Affordability | ||||||
| Level of patient’s family income in local city | 1.349 | 1.079–1.686 | 0.009 | 1.136 | 0.814–1.585 | 0.455 |
| Level of patient’s family income in local city Level of city | 0.739 | 0.671–0.812 | <0.001 | 0.658 | 0.559–0.775 | <0.001 |
| Urban Hukou | 1.467 | 1.061–2.028 | 0.020 | 1.436 | 0.908–2.271 | 0.121 |
| Covered by UEBMI | 0.906 | 0.602–1.363 | 0.636 | — | — | — |
| Covered by BMIRUP | 1.037 | 0.703–1.529 | 0.856 | 0.714 | 0.423–1.206 | 0.208 |
| Physical Disability | ||||||
| Patient’s dependency on assistive devices | 0.869 | 0.781–0.966 | 0.009 | 0.970 | 0.854–1.103 | 0.645 |
| Support by Caregivers | ||||||
| Patient’s marital status (Married as ref) | 0.884 | 0.637–1.226 | 0.461 | — | — | — |
| Number of other family members | 0.914 | 0.834–1.002 | 0.056 | 0.907 | 0.791–1.040 | 0.161 |
| Education Level | ||||||
| Most education years among family members | 1.009 | 0.971–1.049 | 0.644 | 1.019 | 0.970–1.070 | 0.463 |
| Constant | 3.870 | 0.031 | 3.695 | 0.107 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yan, X.; Dong, D.; He, S.; Webster, C. Examining Trans-Provincial Diagnosis of Rare Diseases in China: The Importance of Healthcare Resource Distribution and Patient Mobility. Sustainability 2020, 12, 5444. https://doi.org/10.3390/su12135444
Yan X, Dong D, He S, Webster C. Examining Trans-Provincial Diagnosis of Rare Diseases in China: The Importance of Healthcare Resource Distribution and Patient Mobility. Sustainability. 2020; 12(13):5444. https://doi.org/10.3390/su12135444
Chicago/Turabian StyleYan, Xiang, Dong Dong, Shenjing He, and Chris Webster. 2020. "Examining Trans-Provincial Diagnosis of Rare Diseases in China: The Importance of Healthcare Resource Distribution and Patient Mobility" Sustainability 12, no. 13: 5444. https://doi.org/10.3390/su12135444