Rural Population Aging and the Hospital Utilization in Cities: The Rise of Medical Tourism in China

Abstract
:1. Introduction
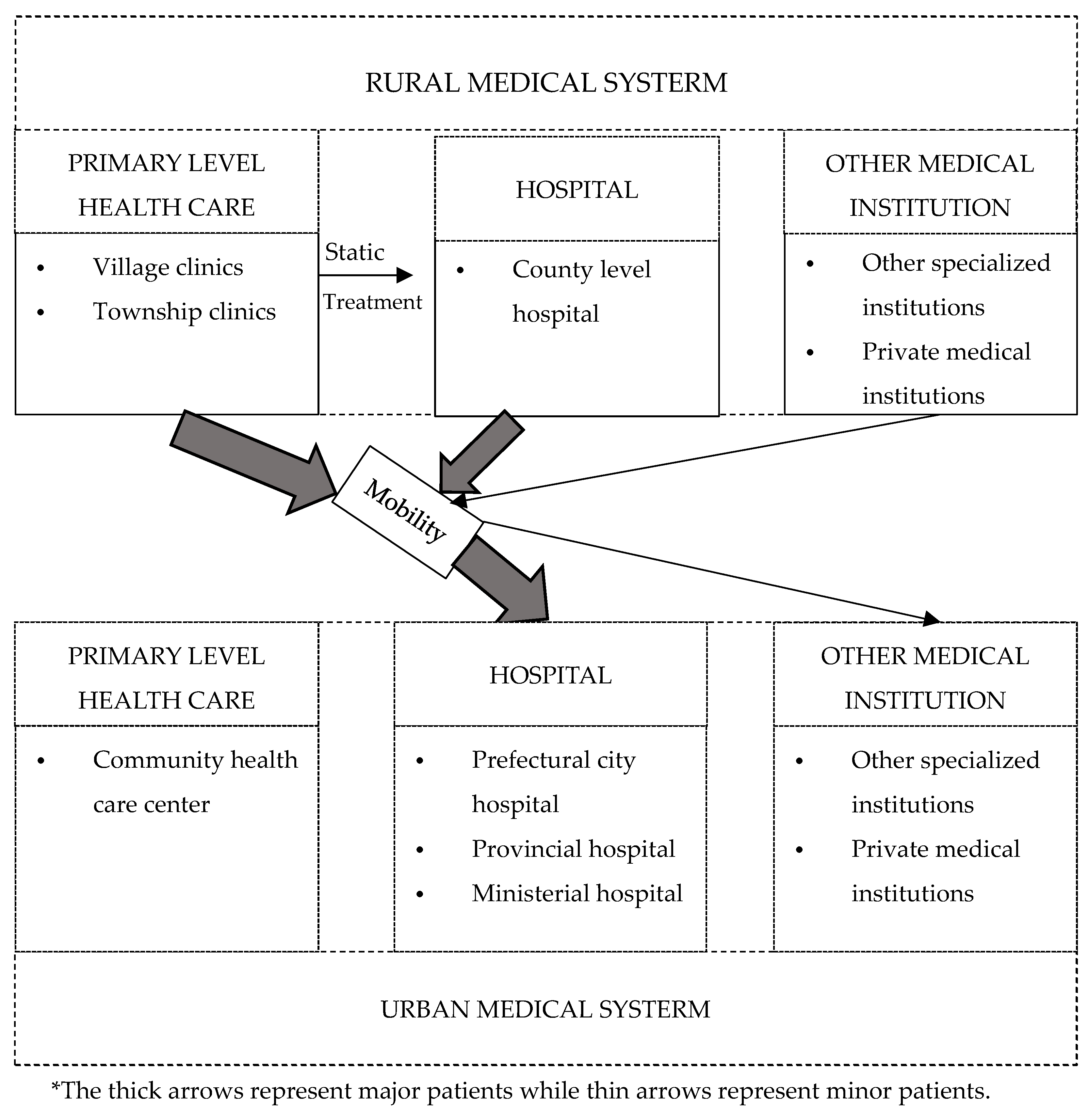
1.1. The Medical System in Rural and Urban China
1.2. Aging and Healthcare Utilization
1.3. Medical Tourism with an Ecological Approach
2. Methods
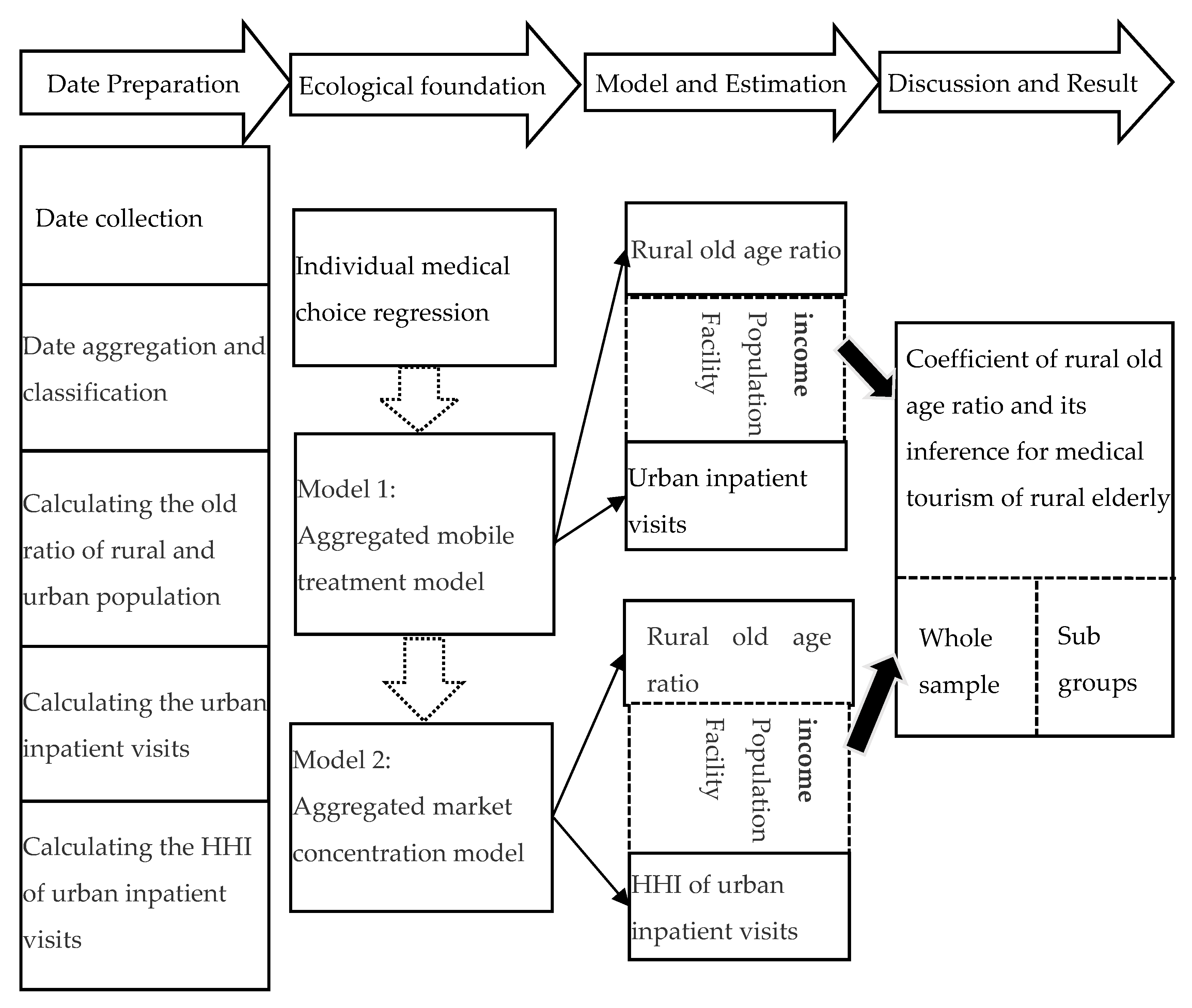
2.1. Study Design
2.2. Data Source
2.3. Variables
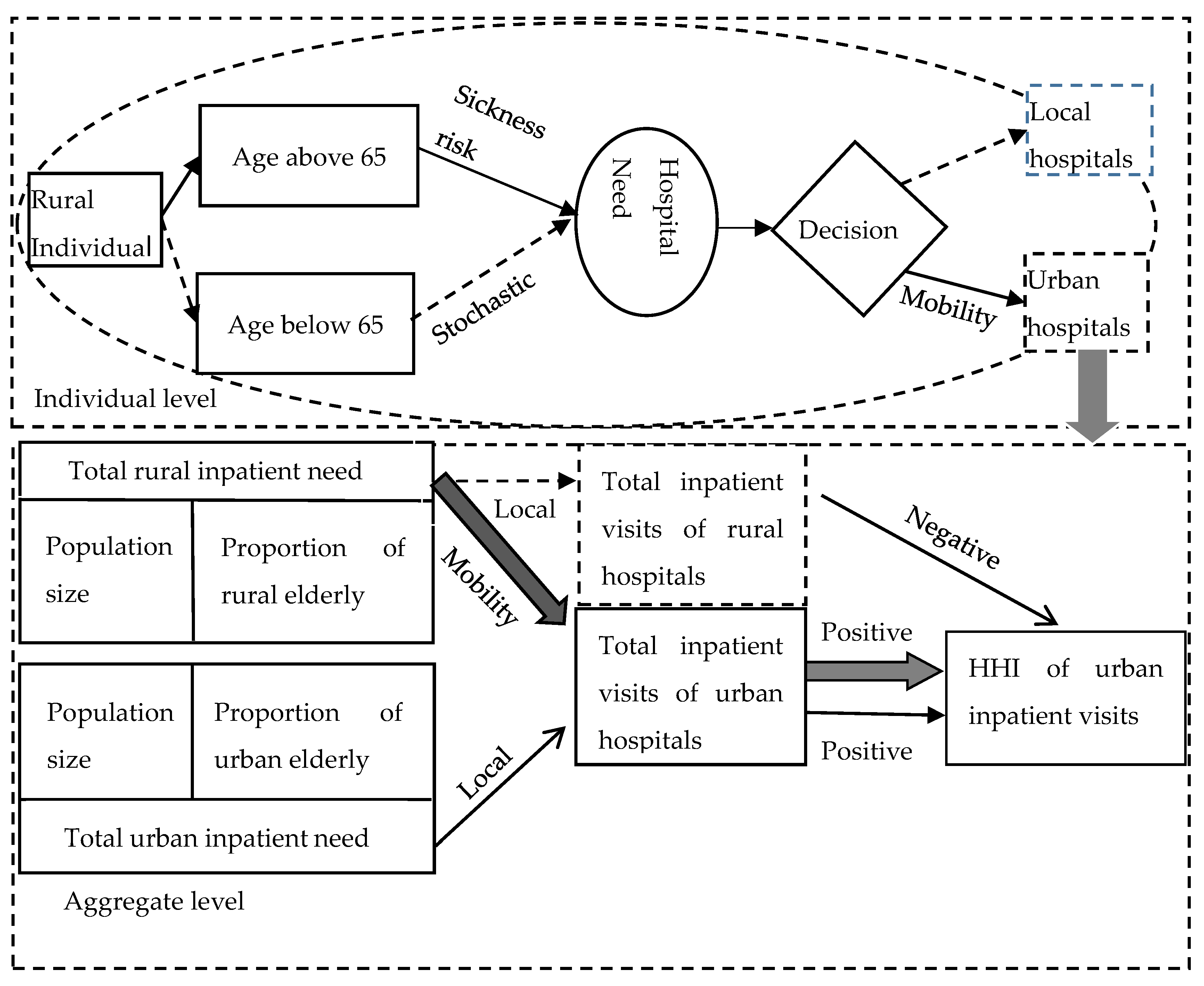
2.4. Ecological Foundation
2.5. Mobile Treatment Model
2.6. Market Concentration Model
2.7. Availability of Data and Materials
2.8. Ethics Approval and Consent to Participate
3. Results
3.1. Descriptive Statistics
3.2. Mobile Treatment Regression
3.3. Market Concentration Model Regression
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Newhouse, J.P. Medical Care Costs: How Much Welfare Loss? J. Econ. Perspect. 1992, 6, 3–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chandra, A.; Skinner, J. Technology Growth and Expenditure Growth in Health Care. J. Econ. Lit. 2012, 50, 645–680. [Google Scholar] [CrossRef] [Green Version]
- Wagstaff, A.; Yip, W.; Lindelow, M.; Hsiao, W.C. China’s health system and its reform: A review of recent studies. Health Econ. 2009, 18, S7–S23. [Google Scholar] [CrossRef]
- Finkelstein, A.; Gentzkow, M.; Williams, H. Sources of Geographic Variation in Health Care: Evidence from Patient Migration. Q. J. Econ. 2016, 131, 1681–1726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rittenberg, L.; Tregarthen, T.D. Principles of Microeconomics; Flat World Knowledge: Boston, MA, USA, 2009. [Google Scholar]
- Torres, J.M.; Waldinger, R. Civic Stratification and the Exclusion of Undocumented Immigrants from Cross-border Health Care. J. Health Soc. Behav. 2015, 56, 438–459. [Google Scholar] [CrossRef] [Green Version]
- De Jesus, M.; Xiao, C. Cross-border health care utilization among the Hispanic population in the United States: Implications for closing the health care access gap. Ethic Health. 2013, 18, 297–314. [Google Scholar] [CrossRef]
- Glinos, I.A.; Baeten, R.; Helble, M.; Maarse, H. A typology of cross-border patient mobility. Health Place. 2010, 16, 1145–1155. [Google Scholar] [CrossRef] [PubMed]
- Qian, D.; Pong, R.W.; Yin, A.; Nagarajan, K.V.; Meng, Q. Determinants of health care demand in poor, rural China: The case of Gansu Province. Health Policy Plan. 2009, 24, 324–334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goodman, L.A. Ecological Regressions and Behavior of Individuals. Am. Sociol. Rev. 1953, 18, 663. [Google Scholar] [CrossRef]
- Schuessler, A.A. Ecological inference. Proc. Natl. Acad. Sci. USA 1999, 96, 10578–10581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siegel, J.S. Applied Demography: Applications to Business, Government, Law and Public Policy; Emerald Publishing: London, UK, 2002; p. 557. [Google Scholar]
- Cai, M.; Liu, E.; Tao, H.; Qian, Z.; Lin, X.; Cheng, Z. Does Level of Hospital Matter? A Study of Mortality of Acute Myocardial Infarction Patients in Shanxi, China. Am. J. Med. Qual. 2017, 33, 185–192. [Google Scholar] [CrossRef]
- Andersen, R.; Newman, J.F. Societal and Individual Determinants of Medical Care Utilization in the United States. Milbank Meml. Fund Q. Health Soc. 1973, 51, 95–124. [Google Scholar] [CrossRef] [Green Version]
- Freund, D.; Smeeding, T. The Future Costs of Health Care in Ageing Societies: Is the Glass Half Full or Half Empty? Ageing in Advanced Industrial States; Springer: Dordrecht, The Netherlands, 2010; pp. 173–193. [Google Scholar]
- Cutler, D.M.; Poterba, J.M.; Sheiner, L.M.; Summers, L.H.; Akerlof, G.A. An Aging Society: Opportunity or Challenge? Brook. Pap. Econ. Act. 1990, 1–73. [Google Scholar] [CrossRef] [Green Version]
- Wong, A.; Wouterse, B.; Slobbe, L.C.; Boshuizen, H.C.; Polder, J.J. Medical innovation and age-specific trends in health care utilization: Findings and implications. Soc. Sci. Med. 2012, 74, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Barer, M.L.; Evans, R.G.; Hertzman, C.; Lomas, J. Aging and health care utilization: New evidence on old fallacies. Soc. Sci. Med. 1987, 24, 851–862. [Google Scholar] [CrossRef]
- Palangkaraya, A.; Yong, J. Population ageing and its implications on aggregate health care demand: Empirical evidence from 22 OECD countries. Int. J. Health Care Financ. Econ. 2009, 9, 391–402. [Google Scholar] [CrossRef]
- Gaynor, M.; Anderson, G.F. Uncertain demand, the structure of hospital costs, and the cost of empty hospital beds. J. Health Econ. 1995, 14, 291–317. [Google Scholar] [CrossRef] [Green Version]
- Wu, F.; Guo, Y.; Kowal, P.; Jiang, Y.; Yu, M.; Li, X.; Zheng, Y.; Xu, J. Prevalence of Major Chronic Conditions among Older Chinese Adults: The Study on Global AGEing and Adult Health (SAGE) Wave 1. PLoS ONE. 2013, 8, e74176. [Google Scholar] [CrossRef] [Green Version]
- Gao, Y.; Chen, G.; Tian, H.; Lin, L.; Lu, J.; Weng, J.; Jia, W.; Ji, L.; Xiao, J.; Zhou, Z.; et al. Prevalence of Hypertension in China: A Cross-Sectional Study. PLoS ONE. 2013, 8, e65938. [Google Scholar] [CrossRef] [Green Version]
- Roberts, K.C.; Rao, D.P.; Bennett, T.L.; Loukine, L.; Jayaraman, G.C. Prevalence and patterns of chronic disease multimorbidity and associated determinants in Canada. Health Promot. Chronic Dis. Prev. Can. 2015, 35, 87–94. [Google Scholar] [CrossRef] [Green Version]
- Corder, L.S.; Woodbury, M.A.; Manton, K.G. Proxy response patterns among the aged: Effects on estimates of health status and medical care utilization from the 1982–1984 long-term care surveys. J. Clin. Epidemiol. 1996, 49, 173–182. [Google Scholar] [CrossRef]
- McFadden, E.; Luben, R.N.; Bingham, S.; Wareham, N.; Kinmonth, A.L.; Khaw, K.-T. Social inequalities in self-rated health by age: Cross-sectional study of 22 457 middle-aged men and women. BMC Public Health. 2008, 8, 230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zavras, D.; Tsiantou, V.; Pavi, E.; Mylona, K.; Kyriopoulos, J. Impact of economic crisis and other demographic and socio-economic factors on self-rated health in Greece. Eur. J. Public Health 2012, 23, 206–210. [Google Scholar] [CrossRef] [Green Version]
- Zweifel, P.; Felder, S.; Werblow, A. Population Ageing and Health Care Expenditure: New Evidence on the “Red Herring”. Geneva Pap. Risk Insur. Issues Pract. 2004, 29, 652–666. [Google Scholar] [CrossRef]
- Seshamani, M.; Gray, A. A longitudinal study of the effects of age and time to death on hospital costs. J. Health Econ. 2004, 23, 217–235. [Google Scholar] [CrossRef] [PubMed]
- Arcury, T.A.; Gesler, W.M.; Preisser, J.S.; Sherman, J.; Spencer, J.; Perin, J. The Effects of Geography and Spatial Behavior on Health Care Utilization among the Residents of a Rural Region. Health Serv. Res. 2005, 40, 135–156. [Google Scholar] [CrossRef] [Green Version]
- Baltagi, B.H.; Yen, Y.-F. Hospital treatment rates and spillover effects: Does ownership matter? Reg. Sci. Urban Econ. 2014, 49, 193–202. [Google Scholar] [CrossRef] [Green Version]
- Eom, T.; Yu, J.; Han, H. Medical tourism in Korea–recent phenomena, emerging markets, potential threats, and challenge factors: A review. Asia Pac. J. Tour. Res. 2019, 24, 563–573. [Google Scholar] [CrossRef]
- Hong, Y.-R.; Samuels, S.; Huo, J.; Lee, N.; Mansoor, H.; Duncan, R. Patient-centered care factors and access to care: A path analysis using the Andersen behavior model. Public Health. 2019, 171, 41–49. [Google Scholar] [CrossRef]
- Moscelli, G.; Siciliani, L.; Gutacker, N.; Cookson, R. Socioeconomic inequality of access to healthcare: Does choice explain the gradient? J. Health Econ. 2018, 57, 290–314. [Google Scholar] [CrossRef]
- Baicker, K.; Chandra, A.; Skinner, J.S. Geographic Variation in Health Care and the Problem of Measuring Racial Disparities. Perspect. Boil. Med. 2005, 48, 42. [Google Scholar] [CrossRef]
- Han, H.; Hwang, J. Growing competition in the healthcare tourism market and customer retention in medical clinics: New and experienced travellers. Curr. Issues Tour. 2015, 21, 680–702. [Google Scholar] [CrossRef]
- Ye, B.H.; Qiu, H.; Yuen, P. Motivations and experiences of Mainland Chinese medical tourists in Hong Kong. Tour. Manag. 2011, 32, 1125–1127. [Google Scholar] [CrossRef]
- Slatin, G.T. Ecological Analysis of Delinquency: Aggregation Effects. Am. Sociol. Rev. 1969, 34, 894. [Google Scholar] [CrossRef] [PubMed]
- Ranney, A. The utility and limitations of aggregate data. In Essays on the Behavioral Study of Politics; University of Illinois Press: Urbana, IL, USA, 1962; pp. 99–101. [Google Scholar]
- Shively, W.P. “Ecological” Inference: The Use of Aggregate Data to Study Individuals. Am. Polit. Sci. Rev. 1969, 63, 1183–1196. [Google Scholar] [CrossRef]
- King, G. A Solution to the Ecological Inference Problem: Reconstructing individual Behavior from Aggregate Data; Princeton University Press: Princeton, NJ, USA, 2013. [Google Scholar]
- Markus, G.B. Electoral Coalitions and Senate Roll Call Behavior: An Ecological Analysis. Am. J. Polit. Sci. 1974, 18, 595. [Google Scholar] [CrossRef]
- Firebaugh, G. A Rule for Inferring Individual-Level Relationships from Aggregate Data. Am. Sociol. Rev. 1978, 43, 557. [Google Scholar] [CrossRef]
- Goodman, L.A. Some Alternatives to Ecological Correlation. Am. J. Sociol. 1959, 64, 610–625. [Google Scholar] [CrossRef]
- Health Care Commission of China. China Health Statistical Yearbook; China Union Medical University Press: Beijing, China, 2018; pp. 76–77, 129–179, 190–192. [Google Scholar]
- Deng, C.; Pan, J. Hospital competition and the expenses for treatments of acute and non-acute common diseases: Evidence from China. BMC Health Serv. Res. 2019, 19, 739. [Google Scholar] [CrossRef]
- Gaynor, M.; Propper, C.; Moreno-Serra, R. Death by Market Power: Reform, Competition and Patient Outcomes in the National Health Service. SSRN Electron. J. 2010, 5, 134–166. [Google Scholar] [CrossRef] [Green Version]
- Reschovsky, J.D.; Staiti, A.B. Access and Quality: Does Rural America Lag Behind? Health Aff. 2005, 24, 1128–1139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Briscoe, J. Water supply and health in developing countries: Selective primary health care revisited. Am. J. Public Health 1984, 74, 1009–1013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fink, G.; Günther, I.; Hill, K. The effect of water and sanitation on child health: Evidence from the demographic and health surveys 1986–2007. Int. J. Epidemiol. 2011, 40, 1196–1204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bradley, E.H.; Canavan, M.; Rogan, E.; Talbert-Slagle, K.; Ndumele, C.; Taylor, L.; Curry, L.A. Variation in Health Outcomes: The Role of Spending on Social Services, Public Health, And Health Care, 2000–2009. Health Aff. 2016, 35, 760–768. [Google Scholar] [CrossRef] [Green Version]
- Wagstaff, A.; Van Doorslaer, Y.; Paci, P. On the measurement of horizontal inequity in the delivery of health care. J. Health Econ. 1991, 10, 169–205. [Google Scholar] [CrossRef] [Green Version]
- O′Donnell, O.; Van Doorslaer, E.; Wagstaff, A.; Lindelow, M. Analyzing Health Equity Using Household Survey Data: A guide to techniques and their implementation. World Bank. 2008, 15, 177–185. [Google Scholar] [CrossRef]
- Brekke, K.R.; Gravelle, H.; Siciliani, L.; Straume, O. Patient Choice, Mobility and Competition among Health Care Providers. In Health Care Provision and Patient Mobility; Springer Science and Business Media LLC: Berlin, Germany, 2014; pp. 1–26. [Google Scholar]
- Victoor, A.; Delnoij, D.M.; Friele, R.; Maindal, J.R.C.H.T. Determinants of patient choice of healthcare providers: A scoping review. BMC Health Serv. Res. 2012, 12, 272. [Google Scholar] [CrossRef] [Green Version]
- Yin, P.; Zhang, M.; Li, Y.; Jiang, Y.; Zhao, W. Prevalence of COPD and its association with socioeconomic status in China: Findings from China Chronic Disease Risk Factor Surveillance 2007. BMC Public Health 2011, 11, 586. [Google Scholar] [CrossRef] [Green Version]
- Kunna, R.; Sebastian, M.S.; Williams, J.S. Measurement and decomposition of socioeconomic inequality in single and multimorbidity in older adults in China and Ghana: Results from the WHO study on global AGEing and adult health (SAGE). Int. J. Equity Health 2017, 16, 79. [Google Scholar] [CrossRef] [Green Version]
- Grossman, M. On the Concept of Health Capital and the Demand for Health. J. Polit. Econ. 1972, 80, 223–255. [Google Scholar] [CrossRef] [Green Version]
- Chetty, R.; Stepner, M.; Abraham, S.; Lin, S.; Scuderi, B.; Turner, N.; Bergeron, A.; Cutler, D. The Association Between Income and Life Expectancy in the United States, 2001–2014. JAMA 2016, 315, 1750–1766. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Whole Sample | Low Income | Middle Income n = 198 Mean(SD) | High Income n = 55 Mean(SD) |
| n = 319 | n = 66 | |||
| Mean(SD) | Mean(SD) | |||
| Total inpatient visits to urban hospitals | 242.4 (200.2) | 111.723 (91.80) | 246.62 (168.50) | 383.86 (284.54) |
| HHI of urban inpatient visits | 0.22 (0.16) | 0.13 (0.08) | 0.20 (0.13) | 0.38 (0.21) |
| Explanatory variables: | ||||
| Rural old-age ratio | 9.36 (2.20) | 7.82 (1.62) | 9.56 (2.18) | 10.48 (1.94) |
| Urban old-age ratio | 8.79 (1.98) | 8.72 (2.04) | 8.99 (1.74) | 8.18 (2.55) |
| Rural population size | 3183.62 (1985.97) | 2095.1 (1331.82) | 3461.57 (2096.00) | 3489.27 (1797.58) |
| Urban population size | 1287.19 (990.06) | 497.27 (300.33) | 1284.63 (679.80) | 2244.32 (1510.73) |
| Rural per capita income | 6795.53 (2978.51) | 4516.34 (1549.57) | 6484.89 (2077.33) | 11000.00 (3432.84) |
| Urban per capita income | 19,000.00 (5585.50) | 16,000.0 (3892.70) | 18,000.0 (4538.57) | 25,000.00 (5600.00) |
| HHI of urban population | 0.09 (0.07) | 0.04 (0.02) | 0.09 (0.06) | 0.16 (0.08) |
| No. of beds per 100 rural persons | 0.30 (0.10) | 0.31 (0.10) | 0.30 (0.10) | 0.29 (0.11) |
| Ratio of rural water improvement | 72.76 (20.95) | 55.8 (26.69) | 72.72 (15.76) | 93.25 (6.45) |
| Urban road per capita | 14.63 (3.93) | 12.60 (3.21) | 14.84 (3.89) | 16.29 (3.89) |
| Urban road total length | 11,000 (9941.08) | 3217.83 (2152.96) | 10000.0 (7505.53) | 21,000.00 (14000.00) |
| Column | (1) | (2) | (3) | (4) |
|---|---|---|---|---|
| VARIABLES | Whole sample | Low income | Middle income | High income |
| Rural old-age ratio | 13.8546 *** | 9.8501 ** | 9.4859 *** | 23.0236 *** |
| (lagged) | (2.9218) | (4.9354) | (3.3429) | (8.7183) |
| Rural pop size | 0.0610 ** | –0.0569 | –0.0926 *** | 0.4098 *** |
| (lagged) | (0.0270) | (0.0561) | (0.0288) | (0.0284) |
| Urban old-age ratio | –0.4892 | 1.0131 | –0.9211 | –19.3115** |
| (lagged) | (1.5256) | (1.2210) | (1.8979) | (7.5315) |
| Urban pop. size | 0.2814 *** | –0.1169 | 0.1758 *** | 0.4842 *** |
| (lagged) | (0.0391) | (0.0792) | (0.0408) | (0.0420) |
| Rural per capita income | –0.0000 | 0.0068 | 0.0259 *** | –0.0831 *** |
| (0.0050) | (0.0152) | (0.0097) | (0.0148) | |
| Urban per capita income | 0.0002 | 0.0191 *** | -0.0001 | 0.0639 *** |
| (0.0009) | (0.0052) | (0.0008) | (0.0109) | |
| Rural water | –1.0554 *** | –0.9739 ** | –3.7604 *** | –11.0880 *** |
| Improvement | (0.3889) | (0.4079) | (0.4140) | (3.0258) |
| Urban total road | 0.0187 *** | 0.0462 *** | 0.0152 *** | 0.0001 |
| Length | (0.0023) | (0.0058) | (0.0032) | (0.0028) |
| Beds per 100 | –103.5130 | 211.0686 * | 81.1574 | –365.1136 * |
| Rural persons | (70.3831) | (115.1104) | (80.0862) | (212.7333) |
| Constant | –300.7799 *** | –89.7935 | 343.6834 | 193.1557 |
| (67.3026) | (209.6316) | (217.2397) | (419.4906) | |
| Fixed Effect | YES | YES | YES | YES |
| Time Effect | YES | YES | YES | YES |
| Observations | 319 | 66 | 198 | 55 |
| Column | (1) | (2) | (3) | (4) |
|---|---|---|---|---|
| VARIABLES | Whole sample | Low income | Middle income | High income |
| Rural old-age ratio | 0.0071 *** | –0.0010 | 0.0084 ** | 0.0295 ** |
| (lagged) | (0.0028) | (0.0051) | (0.0037) | (0.0120) |
| HHI of urban | 0.5508 *** | 2.0938 *** | 0.8174 *** | 0.4603 * |
| population | (0.1375) | (0.3537) | (0.2226) | (0.2774) |
| Rural per capita income | 0.0000 *** | –0.0000 | 0.0000 | 0.0000 * |
| (0.0000) | (0.0000) | (0.0000) | (0.0000) | |
| Urban per capita income | –0.0000 | 0.0000** | 0.0000 | –0.0000 ** |
| (0.0000) | (0.0000) | (0.0000) | (0.0000) | |
| Urban old-age ratio | –0.0054 *** | 0.0012 | –0.0048 *** | –0.0185 ** |
| (lagged) | (0.0014) | (0.0014) | (0.0018) | (0.0091) |
| Urban Road | 0.0021 | 0.0076 *** | 0.0031 * | 0.0050 |
| Per capita | (0.0013) | (0.0018) | (0.0016) | (0.0073) |
| Rural water | –0.0009 *** | –0.0004 | –0.0010 ** | –0.0014 |
| Improvement | (0.0003) | (0.0005) | (0.0004) | (0.0035) |
| Beds per 100 | –0.2297 *** | –0.3388 ** | –0.2217 *** | –0.1049 |
| Rural persons | (0.0643) | (0.1445) | (0.0786) | (0.2691) |
| Constant | 0.4023 *** | –0.1387 * | 0.0242 | 0.7037 |
| (0.0605) | (0.0824) | (0.0520) | (0.5572) | |
| Fixed effect | Yes | Yes | Yes | Yes |
| Time effect | Yes | Yes | Yes | Yes |
| Observations | 319 | 66 | 198 | 55 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, B.; Peng, D.; Zhang, Y.; Yu, J. Rural Population Aging and the Hospital Utilization in Cities: The Rise of Medical Tourism in China. Int. J. Environ. Res. Public Health 2020, 17, 4790. https://doi.org/10.3390/ijerph17134790
Hu B, Peng D, Zhang Y, Yu J. Rural Population Aging and the Hospital Utilization in Cities: The Rise of Medical Tourism in China. International Journal of Environmental Research and Public Health. 2020; 17(13):4790. https://doi.org/10.3390/ijerph17134790
Chicago/Turabian StyleHu, Bing, Daiyan Peng, Yuedong Zhang, and Jiyu Yu. 2020. "Rural Population Aging and the Hospital Utilization in Cities: The Rise of Medical Tourism in China" International Journal of Environmental Research and Public Health 17, no. 13: 4790. https://doi.org/10.3390/ijerph17134790