A Review on the Prevalence of Toxoplasma gondii in Humans and Animals Reported in Malaysia from 2008–2018

 , , , ,
, , , ,
Abstract
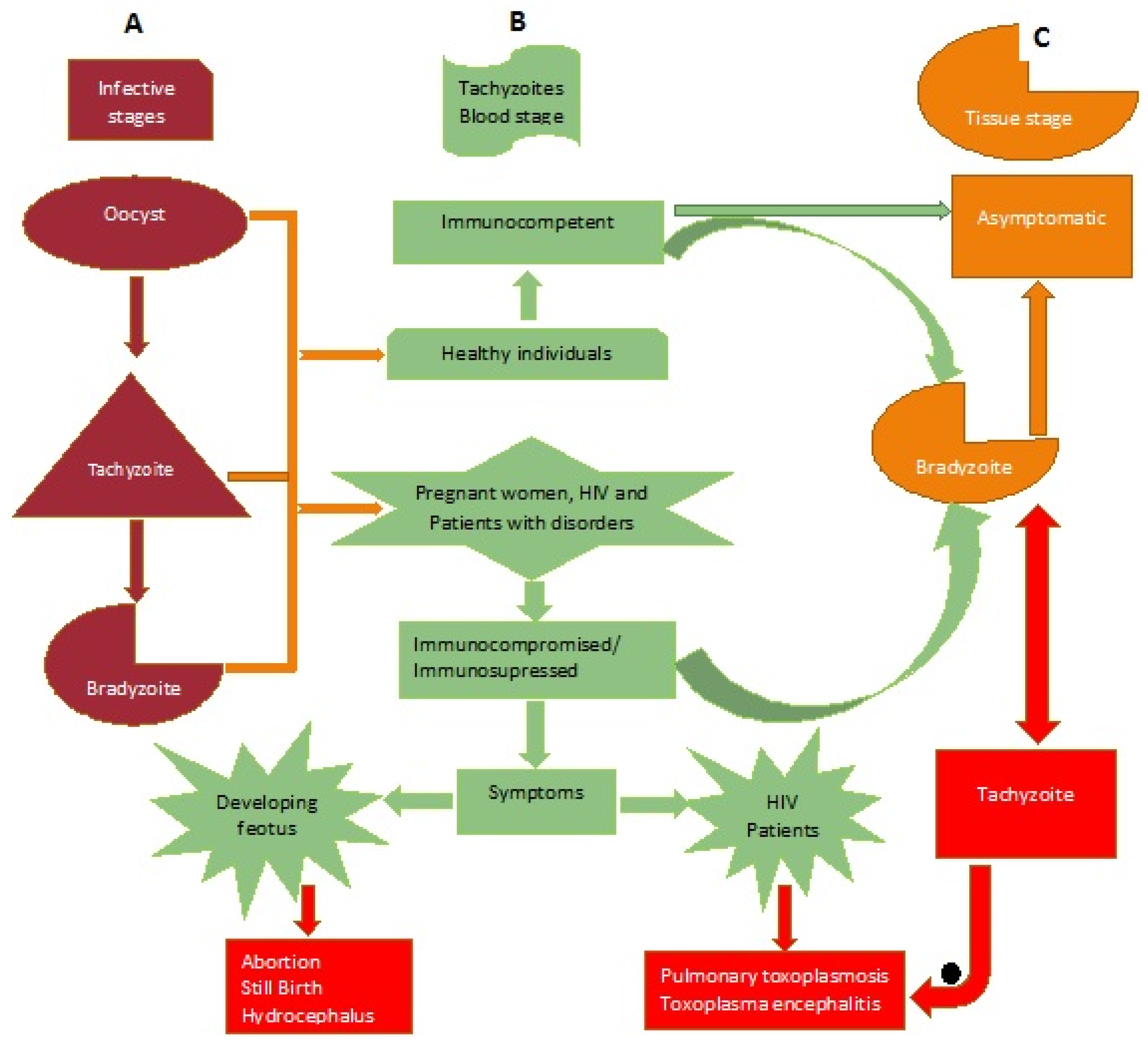
:1. Introduction
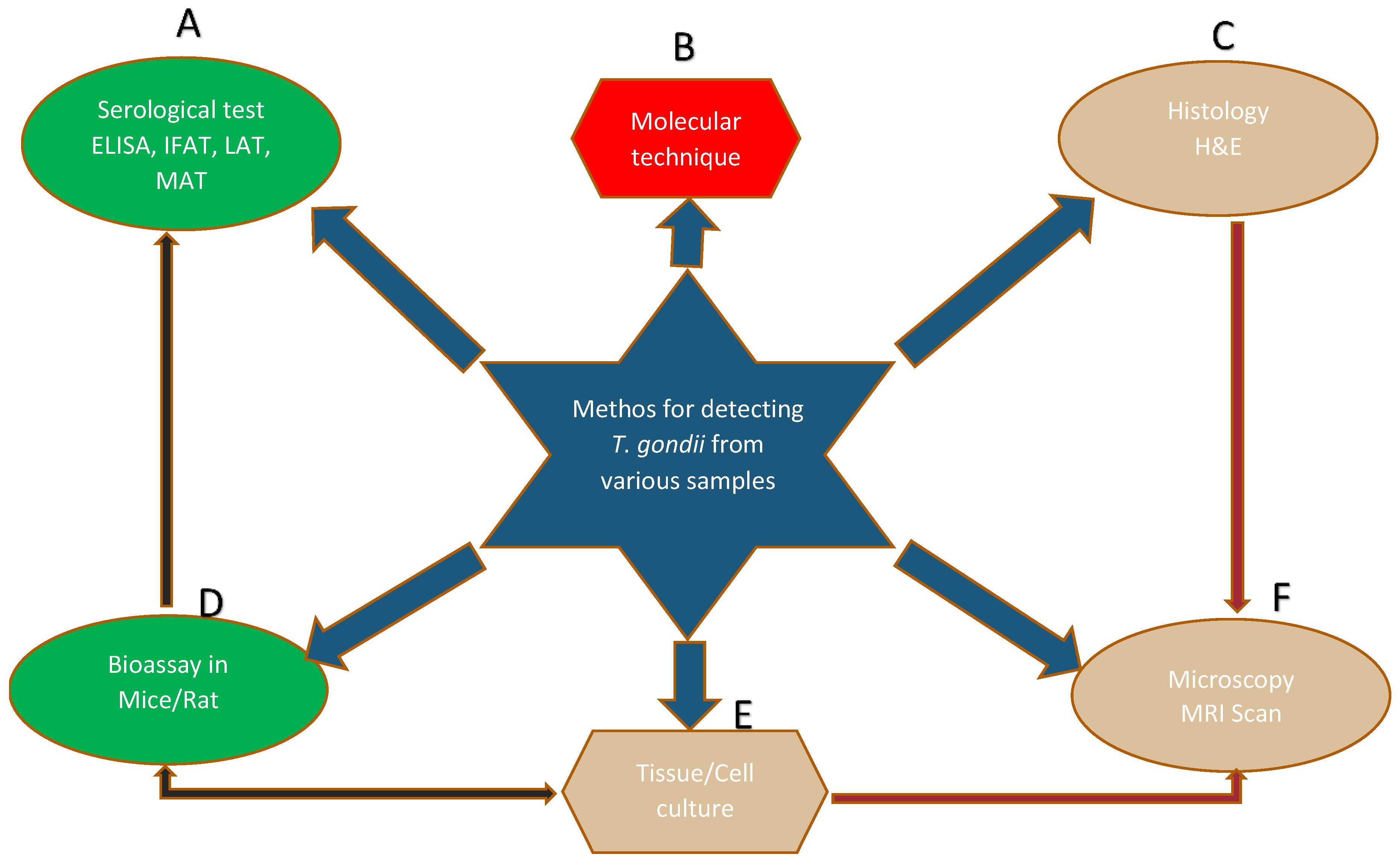
2. Methods for the Detection of T. gondii in Different Samples
3. Comparison of Serological Methods for the Detection of T. gondii Antibodies in Malaysia
4. Human Seroprevalence of Toxoplasmosis in Malaysia
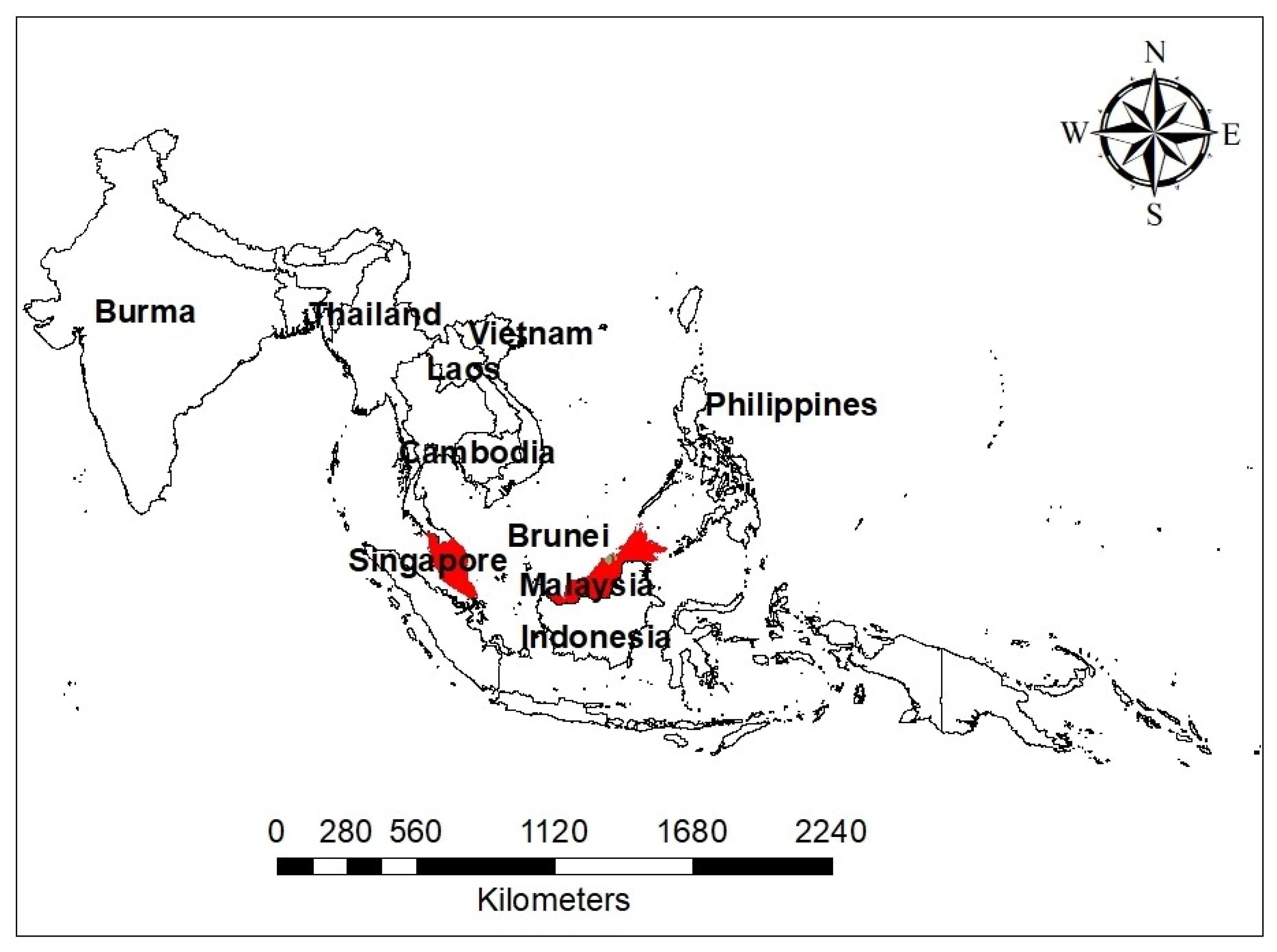
4.1. Toxoplasmosis among Pregnant Women in Malaysia and a Link with Other Neighboring Countries
4.2. Toxoplasmosis among Human Patients Presenting with Various Disorders in Malaysia
4.3. Toxoplasmosis among Migrant Workers in Malaysia
4.4. Toxoplasmosis among Healthy Community Members in Malaysia
4.5. Toxoplasmosis among Schizophrenics in Malaysia
4.6. HIV/AIDS Patients and Rare Toxoplasmosis in Malaysia—A Case Report
5. Animal Seroprevalence of Toxoplasmosis and a Risk of Zoonotic Diseases in Malaysia
5.1. Domestic Animals
5.2. Wild Animals
5.3. Rodents and Other Species
5.4. Wild and Domestic Cat
6. Innovative Diagnostic Approach and Vaccine Development for T. gondii in Malaysia
7. Genetic Diversity and Population Structure of T. gondii in Malaysia
8. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AIDS | Acquired immune deficiency syndrome |
| ELISA | Enzyme-linked immunosorbent assay |
| ESA | Excretory–secretory antigens |
| GRA | Dense granule proteins |
| H&E | Hematoxylin and eosin |
| HIV | Human immunodeficiency virus |
| IFAT | Indirect fluorescence antibody test |
| IgG | Immunoglobulin G |
| IgM | Immunoglobulin M |
| LAT | Latex agglutination test |
| LMAP | Loop-mediated amplification |
| MAT | Modified agglutination test |
| MRI | Magnetic resonance imaging |
| PCR | Polymerase chain reaction |
| PCR-RFLP | Polymerase chain reaction—restriction fragment length polymorphism |
| ROP | Rophtry antigens |
| SAG | Surface antigens |
| T. gondii | Toxoplasma gondii |
| qPCR | Quantitative-PCR |
References
- Abbas, I.E.; Villena, I.; Dubey, J.P. A review on toxoplasmosis in humans and animals from Egypt. Parasitology 2019, 1–81. [Google Scholar] [CrossRef] [PubMed]
- Dubey, J.; Jones, J. Toxoplasma gondii infection in humans and animals in the United States. Int. J. Parasitol. 2008, 38, 1257–1278. [Google Scholar] [CrossRef] [PubMed]
- Polley, L.; Thompson, R.C.A. Parasite zoonoses and climate change: Molecular tools for tracking shifting boundaries. Trends Parasitol. 2009, 25, 285–291. [Google Scholar] [CrossRef] [PubMed]
- Dubey, J.P. History of the discovery of the life cycle of Toxoplasma gondii. Int. J. Parasitol. 2009, 39, 877–882. [Google Scholar] [CrossRef] [PubMed]
- Nimir, A.; Othman, A.; Ee, S.; Musa, Z.; Majid, I.A.; Kamarudin, Z.; Xian, C.; Isa, N.H. Latent toxoplasmosis in patients with different malignancy: A hospital based study. J. Clin. Med. Res. 2010, 2, 117–120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carme, B.; Demar, M.; Ajzenberg, D.; Dardé, M.L. Severe Acquired Toxoplasmosis Caused by Wild Cycle of Toxoplasma gondii, French Guiana. Emerg. Infect. Dis. 2009, 15, 656–658. [Google Scholar] [CrossRef]
- Weiss, L.M.; Dubey, J.P. Toxoplasmosis: A history of clinical observations. Int. J. Parasitol. 2009, 39, 895–901. [Google Scholar] [CrossRef] [Green Version]
- Afonso, C.; Paixão, V.B.; Klaus, A.; Lunghi, M.; Piro, F.; Emiliani, C.; Cristina, M.D.; Costa, R.M. Toxoplasma -induced changes in host risk behaviour are independent of parasite-derived AaaH2 tyrosine hydroxylase. Sci. Rep. 2017, 7, 13822. [Google Scholar] [CrossRef] [Green Version]
- Dabritz, A.A.; Miller, M.A.; Atwill, E.R.; Gardner, I.A.; Leutenegger, C.M.; Melli, A.C.; Conrad, P.A. Detection of Toxoplasma gondii-like oocysts in cat feces and estimates of the environmental oocyst burden. J. Am. Vet. Med. Assoc. 2007, 231, 1676–1684. [Google Scholar] [CrossRef] [Green Version]
- Dubey, J.P. Comparative infectivity of oocysts and bradyzoites of Toxoplasma gondii for intermediate (mice) and definitive (cats) hosts. Vet. Parasitol. 2006, 140, 69–75. [Google Scholar] [CrossRef]
- Aubert, D.; Villena, I. Detection of Toxoplasma gondii oocysts in water: Proposition of a strategy and evaluation in Champagne-Ardenne Region, France. Mem. Inst. Oswaldo Cruz 2009, 104, 290–295. [Google Scholar] [CrossRef] [Green Version]
- Du, F.; Zhang, Q.; Yu, Q.; Hu, M.; Zhou, Y.; Zhao, J. Soil contamination of Toxoplasma gondii oocysts in pig farms in central China. Vet. Parasitol. 2012, 187, 53–56. [Google Scholar] [CrossRef]
- Lass, A.; Pietkiewicz, H.; Modzelewska, E.; Dumètre, A.; Szostakowska, B.; Myjak, P. Detection of Toxoplasma gondii oocysts in environmental soil samples using molecular methods. Eur. J. Clin. Microbiol. Infect. Dis. 2009, 28, 599–605. [Google Scholar] [CrossRef]
- Aspinall, T.V.; Marlee, D.; Hyde, J.E.; Sims, P.F.G. Prevalence of Toxoplasma gondii in commercial meat products as monitored by polymerase chain reaction—food for thought? Int. J. Parasitol. 2002, 32, 1193–1199. [Google Scholar] [CrossRef]
- Kijlstra, A.; Jongert, E. Control of the risk of human toxoplasmosis transmitted by meat. Int. J. Parasitol. 2008, 38, 1359–1370. [Google Scholar] [CrossRef] [PubMed]
- Torgerson, P.R.; Mastroiacovo, P. The global burden of congenital toxoplasmosis: A systematic review. Bull. World Health Organ. 2013, 91, 501–508. [Google Scholar] [CrossRef] [PubMed]
- Dubey, J.P.; Dubey, J.P. Toxoplasmosis of Animals and Humans, 2nd ed.; CRC Press: Boca Rato, FL, USA, 2010. [Google Scholar]
- Robert-Gangneux, F.; Dardé, M.-L. Epidemiology of and Diagnostic Strategies for toxoplasmosis. Clin. Microbiol. Rev. 2012, 25, 264–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hill, D.E.; Chirukandoth, S.; Dubey, J.P. Biology and epidemiology of Toxoplasma gondii in man and animals. Anim. Health Res. Rev. 2005, 6, 41–61. [Google Scholar] [CrossRef]
- Hajissa, K.; Zakaria, R.; Suppian, R.; Mohamed, Z. Immunogenicity of Multiepitope Vaccine Candidate against Toxoplasma gondii Infection in BALB/c Mice. Iran. J. Parasitol. 2018, 13, 215–224. [Google Scholar]
- Nissapatorn, V.; Abdullah, K.A. Review on human toxoplasmosis in Malaysia: The past, present and prospective future. Southeast Asian J. Trop. Med. Public Health 2004, 35, 7. [Google Scholar]
- Ajzenberg, D.; Yera, H.; Marty, P.; Paris, L.; Dalle, F.; Menotti, J.; Aubert, D.; Franck, J.; Bessières, M.-H.; Quinio, D. Genotype of 88 Toxoplasma gondii isolates associated with toxoplasmosis in immunocompromised patients and correlation with clinical findings. J. Infect. Dis. 2009, 199, 1155–1167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yahaya, N. Review of toxoplasmosis in Malaysia. Southeast Asian J. Trop. Med. Public Health 1991, 22, 102–106. [Google Scholar] [PubMed]
- Nissapatorn, V. Toxoplasmosis: A silent threat in Southeast Asia. Res. J. Parasitol. 2007, 2, 1–12. [Google Scholar]
- Cantlay, J.C.; Ingram, D.J.; Meredith, A.L. A Review of Zoonotic Infection Risks Associated with the Wild Meat Trade in Malaysia. EcoHealth 2017, 14, 361–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nissapatorn, V.; Lee, C.; Cho, S.; Rohela, M.; Anuar, A.K.; Quek, K.; Latt, H. Toxoplasmosis in HIV/AIDS patients in Malaysia. Southeast Asian J. Trop. Med. Public Health 2003, 34, 7. [Google Scholar]
- Emelia, O.; Zeehaida, M.; Sulaiman, O.; Rohela, M.; Saadatnia, G.; Yeng, C.; Rahmah, N. An Assay for Selection of Sera with Circulating Toxoplasma gondii Antigens. J. Immunoassay Immunochem. 2009, 31, 79–91. [Google Scholar] [CrossRef]
- Rahumatullah, A.; Khoo, B.Y.; Noordin, R. Triplex PCR using new primers for the detection of Toxoplasma gondii. Exp. Parasitol. 2012, 131, 231–238. [Google Scholar] [CrossRef] [Green Version]
- Lau, Y.L.; Meganathan, P.; Sonaimuthu, P.; Thiruvengadam, G.; Nissapatorn, V.; Chen, Y. Specific, Sensitive, and Rapid Diagnosis of Active Toxoplasmosis by a Loop-Mediated Isothermal Amplification Method Using Blood Samples from Patients. J. Clin. Microbiol. 2010, 48, 3698–3702. [Google Scholar] [CrossRef] [Green Version]
- Fazly, Z.; Nurulaini, R.; Shafarin, M.; Fariza, N.; Zawida, Z.; Muhamad, H.; Adnan, M.; Premaalatha, B.; Erwanas, A.; Zaini, C. Zoonotic parasites from exotic meat in Malaysia. Trop. Biomed. 2013, 30, 535–542. [Google Scholar]
- Puvanesuaran, V.R.; Ibrahim, N.; Noordin, R.; Balakrishnan, V. Isolation of viable Toxoplasma gondii cysts from brain samples for oral infection. Eur. Rev. Med. Pharmacol. Sci. 2012, 16, 1179–1183. [Google Scholar]
- Saadatnia, G.; Haj Ghani, H.; Khoo, B.Y.; Maimunah, A.; Rahmah, N. Optimization of Toxoplasma gondii cultivation in VERO cell line. Trop. Biomed. 2010, 27, 125–130. [Google Scholar] [PubMed]
- Dubremetz, J.F.; Ferguson, D.J.P. The role played by electron microscopy in advancing our understanding of Toxoplasma gondii and other apicomplexans. Int. J. Parasitol. 2009, 39, 883–893. [Google Scholar] [CrossRef] [PubMed]
- Casartelli-Alves, L.; Boechat, V.C.; Macedo-Couto, R.; Ferreira, L.C.; Nicolau, J.L.; Neves, L.B.; Millar, P.R.; Vicente, R.T.; Oliveira, R.V.C.; Muniz, A.G.; et al. Sensitivity and specificity of serological tests, histopathology and immunohistochemistry for detection of Toxoplasma gondii infection in domestic chickens. Vet. Parasitol. 2014, 204, 346–351. [Google Scholar] [CrossRef] [PubMed]
- Emelia, O.; Rahana, A.R.; Mohamad Firdaus, A.; Cheng, H.S.; Nursyairah, M.S.; Fatinah, A.S.; Azmawati, M.N.; Siti, N.A.; Aisah, M.Y. IgG avidity assay: A tool for excluding acute toxoplasmosis in prolonged IgM titer sera from pregnant women. Trop. Biomed. 2014, 31, 633–640. [Google Scholar] [PubMed]
- Andiappan, H.; Nissapatorn, V.; Sawangjaroen, N.; Nyunt, M.H.; Lau, Y.-L.; Khaing, S.L.; Aye, K.M.; Mon, N.C.N.; Tan, T.-C.; Kumar, T.; et al. Comparative study on Toxoplasma infection between Malaysian and Myanmar pregnant women. Parasit. Vectors 2014, 7. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, Z.; Hajissa, K. Seroprevalence of Toxoplasma gondii infection among patients in Hospital Universiti Sains Malaysia. Trop. Biomed. 2016, 33, 78–83. [Google Scholar]
- Nissapatorn, V.; Leong, T.H.; Lee, R.; Init, I.; Ibrahim, J.; Yen, T.S. Seroepidemiology of Toxoplasmosis in Renal Patients. Southeast Asian J. Trop. Med. Public Health 2011, 42, 237–247. [Google Scholar]
- Ngui, R.; Lim, Y.A.L.; Amir, N.F.H.; Nissapatorn, V.; Mahmud, R. Seroprevalence and sources of toxoplasmosis among Orang Asli (indigenous) communities in Peninsular Malaysia. Am. J. Trop. Med. Hyg. 2011, 85, 660–666. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, A.F.; Ngui, R.; Muhammad Aidil, R.; Lim, Y.A.; Rohela, M. Current status of parasitic infections among Pangkor Island community in Peninsular Malaysia. Trop. Biomed. 2014, 31, 836–843. [Google Scholar]
- Sahimin, N.; Lim, Y.A.L.; Ariffin, F.; Behnke, J.M.; Basáñez, M.-G.; Walker, M.; Lewis, J.W.; Noordin, R.; Abdullah, K.A.; Mohd Zain, S.N. Socio-demographic determinants of Toxoplasma gondii seroprevalence in migrant workers of Peninsular Malaysia. Parasit. Vectors 2017, 10, 238. [Google Scholar] [CrossRef] [Green Version]
- Chan, B.T.E.; Amal, R.N.; Noor Hayati, M.I.; Kino, H.; Anisah, N.; Norhayati, M.; Sulaiman, O.; Mohammed Abdullah, M.; Fatmah, M.S.; Roslida, A.R. Seroprevalence of toxoplasmosis among migrant workers from different Asian countries working in Malaysia. Southeast Asian J. Trop. Med. Public Health 2008, 39, 9. [Google Scholar] [PubMed]
- Juanah, L.Y.; Jalaludin, J.; Osman, M.; Osman, Z.J. Seroprevalence of Toxoplasma gondii Among Schizophrenics at Hospital Kajang. Am. J. Infect. Dis. 2013, 9, 11–16. [Google Scholar] [CrossRef] [Green Version]
- Omar, A.; Bakar, O.C.; Adam, N.F.; Osman, H.; Osman, A.; Suleiman, A.H.; Manaf, M.R.A.; Selamat, M.I. Seropositivity and serointensity of Toxoplasma gondii antibodies and DNA among patients with schizophrenia. Korean J. Parasitol. 2015, 53, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Nimir, A.R.; Osman, E.; Ibrahim, I.A.A.; Saliem, A.M. Is it toxoplasma encephalitis, HIV encephalopathy or brain tuberculoma? BMJ Case Rep. 2013, 2013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brandon-Mong, G.-J.; Che Mat Seri, N.A.A.; Sharma, R.S.-K.; Andiappan, H.; Tan, T.-C.; Lim, Y.A.-L.; Nissapatorn, V. Seroepidemiology of Toxoplasmosis among People Having Close Contact with Animals. Front. Immunol. 2015, 6, 143. [Google Scholar] [CrossRef] [Green Version]
- Rahman, W.A.; Manimegalai, V.; Chandrawathani, P.; Nurulaini, R.; Zaini, C.M.; Premaalatha, B. Seroprevalence of Toxoplasma gondii in Malaysian Cattle. Malays. J. Vet. Res. 2011, 2, 51–56. [Google Scholar]
- Chandrawathani, P.; Nurulaini, R.; Zanin, C.M.; Premaalatha, B.; Adnan, M. Jamnah Seroprevalence of Toxoplasma gondii antibodies in pigs, goats, cattle, dogs and cats in peninsular Malaysia. Trop. Biomed. 2008, 25, 257–258. [Google Scholar]
- Normaznah, Y.; Azizah, M.A.; Azuan, M.I.; Latifah, I.; Rahmat, S.; Nasir, M.A. Seroprevalence of Toxoplasma gondii in Rodents from Various Locations in Peninsular Malaysia. Southeast Asian J. Trop. Med. Public Health 2015, 46, 388–395. [Google Scholar]
- Chen, R.; Lu, S.; Lou, D.; Lin, A.; Zeng, X.; Ding, Z.; Wen, L.; Ohta, N.; Wang, J.; Fu, C. Evaluation of a rapid ELISA technique for detection of circulating antigens of Toxoplasma gondii. Microbiol. Immunol. 2008, 52, 180–187. [Google Scholar] [CrossRef]
- Naghili, B.; Abbasalizadeh, S.; Tabrizi, S.; Rajaii, M.; Akramiyan, M.; Alikhah, H.; Naghavi-Behzad, M.; Piri, R.; Karkon-Shayan, F.; Tehrani-Ghadim, S. Comparison of IIF, ELISA and IgG avidity tests for the detection of anti-Toxoplasma antibodies in single serum sample from pregnant women. Infez. Med. 2017, 1, 50–56. [Google Scholar]
- Kotresha, D.; Poonam, D.; Muhammad Aidil, Y.; Saadatnia, G.; Nurulhasanah, O. Recombinant proteins from new constructs of SAG1 and GRA7 sequences and their usefulness to detect acute toxoplasmosis. Trop. Biomed. 2012, 29, 129–137. [Google Scholar] [PubMed]
- Villard, O.; Cimon, B.; L’Ollivier, C.; Fricker-Hidalgo, H.; Godineau, N.; Houze, S.; Paris, L.; Pelloux, H.; Villena, I.; Candolfi, E. Serological diagnosis of Toxoplasma gondii infection. Diagn. Microbiol. Infect. Dis. 2016, 84, 22–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deshpande, P.S.; Kotresha, D.; Noordin, R.; Yunus, M.H.; Saadatnia, G.; Golkar, M.; Osman, S.; Karim, I.Z.A.; Ghaffarifar, F.; Deshpande, P.S.; et al. IgG avidity western blot using Toxoplasma gondii rGRA-7 cloned from nucleotides 39-711 for serodiagnosis of acute toxoplasmosis. Rev. Inst. Med. Trop. São Paulo 2013, 55, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Andiappan, H.; Nissapatorn, V.; Sawangjaroen, N.; Chemoh, W.; Lau, Y.L.; Kumar, T.; Onichandran, S.; Suwanrath, C.; Chandeying, V. Toxoplasma infection in pregnant women: A current status in Songklanagarind hospital, southern Thailand. Parasit. Vectors 2014, 7, 239. [Google Scholar] [CrossRef] [Green Version]
- Nissapatorn, V.; Suwanrath, C.; Sawangjaroen, N.; Ling, L.Y.; Chandeying, V. Toxoplasmosis-serological evidence and associated risk factors among pregnant women in southern Thailand. Am. J. Trop. Med. Hyg. 2011, 85, 243–247. [Google Scholar] [CrossRef]
- van Enter, B.J.D.; Lau, Y.-L.; Ling, C.L.; Watthanaworawit, W.; Sukthana, Y.; Lee, W.-C.; Nosten, F.; McGready, R. Seroprevalence of Toxoplasma gondii Infection in Refugee and Migrant Pregnant Women along the Thailand-Myanmar Border. Am. J. Trop. Med. Hyg. 2017, 97, 232–235. [Google Scholar] [CrossRef] [Green Version]
- Dubey, J.P. The Toxoplasma gondii oocyst from cat feces. J. Exp. Med. 1970, 132, 636–662. [Google Scholar] [CrossRef] [Green Version]
- Andiappan, H.; Nissapatorn, V.; Sawangjaroen, N.; Khaing, S.-L.; Salibay, C.C.; Cheung, M.M.M.; Dungca, J.Z.; Chemoh, W.; Xiao Teng, C.; Lau, Y.-L.; et al. Knowledge and practice on Toxoplasma infection in pregnant women from Malaysia, Philippines, and Thailand. Front. Microbiol. 2014, 5. [Google Scholar] [CrossRef]
- Carruthers, V.B.; Suzuki, Y. Effects of Toxoplasma gondii Infection on the Brain. Schizophr. Bull. 2007, 33, 745–751. [Google Scholar] [CrossRef] [Green Version]
- McConkey, G.A.; Martin, H.L.; Bristow, G.C.; Webster, J.P. Toxoplasma gondii infection and behaviour—location, location, location? J. Exp. Biol. 2013, 216, 113–119. [Google Scholar] [CrossRef] [Green Version]
- Vyas, A.; Kim, S.-K.; Giacomini, N.; Boothroyd, J.C.; Sapolsky, R.M. Behavioral changes induced by Toxoplasma infection of rodents are highly specific to aversion of cat odors. Proc. Natl. Acad. Sci. 2007, 104, 6442–6447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horacek, J.; Flegr, J.; Tintera, J.; Verebova, K.; Spaniel, F.; Novak, T.; Brunovsky, M.; Bubenikova-Valesova, V.; Holub, D.; Palenicek, T.; et al. Latent toxoplasmosis reduces gray matter density in schizophrenia but not in controls: Voxel-based-morphometry (VBM) study. World J. Biol. Psychiatry 2012, 13, 501–509. [Google Scholar] [CrossRef] [PubMed]
- Flegr, J. How and why Toxoplasma makes us crazy. Trends Parasitol. 2013, 29, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Fong, M.Y.; Wong, K.T.; Rohela, M.; Tan, L.H.; Adeeba, K.; Lee, Y.Y.; Lau, Y.L. Unusual manifestation of cutaneous toxoplasmosis in a HIV-positive patient. Trop. Biomed. 2010, 27, 447–450. [Google Scholar] [PubMed]
- Sánchez, A.; Prats-van der Ham, M.; Tatay-Dualde, J.; Paterna, A.; de la Fe, C.; Gómez-Martín, Á.; Corrales, J.C.; Contreras, A. Zoonoses in Veterinary Students: A Systematic Review of the Literature. PLoS ONE 2017, 12, e0169534. [Google Scholar] [CrossRef] [PubMed]
- Nimir, A.R.; Linn, T.C. Detection of toxoplasmosis in environmental samples at a wet market of a capital city centre. Acta Medica (Hradec Kralove) 2011, 54, 107–110. [Google Scholar] [CrossRef] [Green Version]
- Matsuda, I.; Tuuga, A.; Higashi, S. Clouded leopard (Neofelis diardi) predation on proboscis monkeys (Nasalis larvatus) in Sabah, Malaysia. Primates 2008, 49, 227–231. [Google Scholar] [CrossRef]
- Verma, S.K.; Sweeny, A.R.; Lovallo, M.J.; Calero-Bernal, R.; Kwok, O.C.; Jiang, T.; Su, C.; Grigg, M.E.; Dubey, J.P. Seroprevalence, isolation and co-infection of multiple Toxoplasma gondii strains in individual bobcats (Lynx rufus) from Mississippi, USA. Int. J. Parasitol. 2017, 47, 297–303. [Google Scholar] [CrossRef] [Green Version]
- Amerizadeh, A.; Khoo, B.Y.; Teh, A.Y.; Golkar, M.; Abdul Karim, I.Z.; Osman, S.; Yunus, M.H.; Noordin, R. Identification and real-time expression analysis of selected Toxoplasma gondii in-vivo induced antigens recognized by IgG and IgM in sera of acute toxoplasmosis patients. BMC Infect. Dis. 2013, 13, 287. [Google Scholar] [CrossRef] [Green Version]
- Ashwinder, K.; Kho, M.T.; Chee, P.M.; Lim, W.Z.; Yap, I.K.S.; Choi, S.B.; Yam, W.K. Targeting Heat Shock Proteins 60 and 70 of Toxoplasma gondii as a Potential Drug Target: In Silico Approach. Interdiscip. Sci. Comput. Life Sci. 2016, 8, 374–387. [Google Scholar] [CrossRef]
- Ching, X.T.; Fong, M.Y.; Lau, Y.L. Evaluation of Immunoprotection Conferred by the Subunit Vaccines of GRA2 and GRA5 against Acute Toxoplasmosis in BALB/c Mice. Front. Microbiol. 2016, 7, 609. [Google Scholar] [CrossRef] [PubMed]
- Hajissa, K.; Zakaria, R.; Suppian, R.; Mohamed, Z. Design and evaluation of a recombinant multi-epitope antigen for serodiagnosis of Toxoplasma gondii infection in humans. Parasit. Vectors 2015, 8, 315. [Google Scholar] [CrossRef] [Green Version]
- Hajissa, K.; Zakaria, R.; Suppian, R.; Mohamed, Z. An evaluation of a recombinant multiepitope based antigen for detection of Toxoplasma gondii specific antibodies. BMC Infect. Dis. 2017, 17, 807. [Google Scholar] [CrossRef] [PubMed]
- Ling Lau, Y.; Yik Fong, M. Toxoplasma gondii: Serological characterization and immunogenicity of recombinant surface antigen 2 (SAG2) expressed in the yeast Pichia pastoris. Exp. Parasitol. 2008, 119, 373–378. [Google Scholar] [CrossRef] [PubMed]
- Meganathan, P.; Singh, S.; Ling, L.Y.; Singh, J.; Subrayan, V.; Nissapatorn, V. Detection of Toxoplasma gondii DNA by PCR following microwave treatment of serum and whole blood. Southeast Asian J. Trop. Med. Public Health 2010, 41, 9. [Google Scholar]
- Saadatnia, G.; Ghaffarifar, F.; Khalilpour, A.; Amerizadeh, A.; Rahmah, N. A Toxoplasma gondii 10 kDa in vitro excretory secretory antigen reactive with human IgM and IgA antibodies. Trop. Biomed. 2011, 28, 606–614. [Google Scholar]
- Sonaimuthu, P.; Fong, M.Y.; Kalyanasundaram, R.; Mahmud, R.; Lau, Y.L. Sero-diagnostic evaluation of Toxoplasma gondii recombinant Rhoptry antigen 8 expressed in E. coli. Parasit. Vectors 2014, 7, 297. [Google Scholar] [CrossRef] [Green Version]
- Lim, S.S.-Y.; Othman, R.Y. Recent advances in Toxoplasma gondii immunotherapeutics. Korean J. Parasitol. 2014, 52, 581–593. [Google Scholar] [CrossRef]
- Lau, Y.L.; Ching, X.T.; Fong, M.Y. Evaluation of the Protective Effect of Deoxyribonucleic Acid Vaccines Encoding Granule Antigen 2 and 5 Against Acute Toxoplasmosis in BALB/c Mice. Am. J. Trop. Med. Hyg. 2017, 96, 1441–1447. [Google Scholar] [CrossRef]
- Lew, M.H.; Noordin, R.; Monsur Alam Khan, M.; Tye, G.J. Immune Stimulation of RAP domain binding protein (rTgRA15) from Toxoplasma gondii. Pathog. Glob. Health 2018, 1–7. [Google Scholar] [CrossRef]
- Parthasarathy, S.; Fong, M.Y.; Ramaswamy, K.; Lau, Y.L. Protective immune response in BALB/c mice induced by DNA vaccine of the ROP8 gene of Toxoplasma gondii. Am. J. Trop. Med. Hyg. 2013, 88, 883–887. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sonaimuthu, P.; Ching, X.T.; Fong, M.Y.; Kalyanasundaram, R.; Lau, Y.L. Induction of Protective Immunity against Toxoplasmosis in BALB/c Mice Vaccinated with Toxoplasma gondii Rhoptry-1. Front. Microbiol. 2016, 7, 808. [Google Scholar] [CrossRef] [PubMed]
- Lai, M.-Y.; Lau, Y.-L. Screening and identification of host proteins interacting with Toxoplasma gondii SAG2 by yeast two-hybrid assay. Parasit. Vectors 2017, 10, 456. [Google Scholar] [CrossRef] [PubMed]
- Ellen, T.; Glenn, M. Neurophysiological Changes Induced by Chronic Toxoplasma gondii Infection. Pathogens 2017, 6, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nissapatorn, V. Toxoplasma gondii and HIV: A never-ending story. Lancet HIV 2017, 4, e146–e147. [Google Scholar] [CrossRef]
- Sun, H.; Wang, Y.; Zhang, Y.; Ge, W.; Zhang, F.; He, B.; Li, Z.; Fan, Q.; Wang, W.; Tu, C.; et al. Prevalence and Genetic Characterization of Toxoplasma gondii in Bats in Myanmar. Appl. Environ. Microbiol. 2013, 79, 3526–3528. [Google Scholar] [CrossRef] [Green Version]
- Ajzenberg, D.; Bañuls, A.L.; Su, C.; Dumètre, A.; Demar, M.; Carme, B.; Dardé, M.L. Genetic diversity, clonality and sexuality in Toxoplasma gondii. Int. J. Parasitol. 2004, 34, 1185–1196. [Google Scholar] [CrossRef]
- Dardé, M.-L. Genetic analysis of the diversity in Toxoplasma gondii. Ann Ist Super Sanita 2004, 40, 57–63. [Google Scholar]
- Howe, D.K.; Sibley, L.D. Toxoplasma gondii Comprises Three Clonal Lineages: Correlation of Parasite Genotype with Human Disease. J. Infect. Dis. 1995, 172, 1561–1566. [Google Scholar] [CrossRef]
- Dubey, J.P. Bradyzoite-Induced Murine Toxoplasmosis: Stage Conversion, Pathogenesis, and Tissue Cyst Formation in Mice Fed Bradvzoites of - Different Strains of Toxoplasma gondii. J. Eukaryot. Microbiol. 2007, 44, 592–602. [Google Scholar] [CrossRef]
- Rajendran, C.; Su, C.; Dubey, J.P. Molecular genotyping of Toxoplasma gondii from Central and South America revealed high diversity within and between populations. Infect. Genet. Evol. 2012, 12, 359–368. [Google Scholar] [CrossRef] [PubMed]
- Abd El-Razik, K.A.; Barakat, A.M.A.; Hussein, H.A.; Younes, A.M.; Elfadaly, H.A.; Eldebaky, H.A.; Soliman, Y.A. Seroprevalence, isolation, molecular detection and genetic diversity of Toxoplasma gondii from small ruminants in Egypt. J. Parasit. Dis. 2018. [Google Scholar] [CrossRef]
- Chemoh, W.; Sawangjaroen, N.; Nissapatorn, V.; Sermwittayawong, N. Molecular investigation on the occurrence of Toxoplasma gondii oocysts in cat feces using TOX-element and ITS-1 region targets. Vet. J. 2016, 215, 118–122. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.W.; Gao, J.M.; Huo, X.X.; Wang, L.; Yu, L.; Halm-Lai, F.; Xu, Y.H.; Song, W.J.; Hide, G.; Shen, J.L.; et al. Genotyping of Toxoplasma gondii isolates from cats in different geographic regions of China. Vet. Parasitol. 2011, 183, 166–170. [Google Scholar] [CrossRef] [PubMed]
- Qian, W.-F.; Yan, W.-C.; Wang, T.-Q.; Zhai, K.; Han, L.-F.; Lv, C.-C. Prevalence and Genetic Characterization of Toxoplasma gondii in Pet Dogs in Central China. Korean J. Parasitol. 2015, 53, 125–128. [Google Scholar] [CrossRef] [PubMed]
- Tian, Y.-M.; Huang, S.-Y.; Miao, Q.; Jiang, H.-H.; Yang, J.-F.; Su, C.; Zhu, X.-Q.; Zou, F.-C. Genetic characterization of Toxoplasma gondii from cats in Yunnan Province, Southwestern China. Parasit. Vectors 2014, 7, 178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puvanesuaran, V.R.; Noordin, R.; Balakrishnan, V. Genotyping of Toxoplasma gondii Isolates from Wild Boars in Peninsular Malaysia. PLoS ONE 2013, 8, e61730. [Google Scholar] [CrossRef] [Green Version]
- Chaichan, P.; Mercier, A.; Galal, L.; Mahittikorn, A.; Ariey, F.; Morand, S.; Boumédiène, F.; Udonsom, R.; Hamidovic, A.; Murat, J.B.; et al. Geographical distribution of Toxoplasma gondii genotypes in Asia: A link with neighboring continents. Infect. Genet. Evol. 2017, 53, 227–238. [Google Scholar] [CrossRef]
- Howe, D.K.; Honoré, S.; Derouin, F.; Sibley, L.D. Determination of genotypes of Toxoplasma gondii strains isolated from patients with toxoplasmosis. J. Clin. Microbiol. 1997, 35, 1411–1414. [Google Scholar] [CrossRef] [Green Version]
- Khan, A. Genetic Divergence of Toxoplasma gondii Strains Associated with Ocular Toxoplasmosis, Brazil. Emerg. Infect. Dis. 2006, 12, 942–949. [Google Scholar] [CrossRef]
- Khan, A.; Su, C.; German, M.; Storch, G.A.; Clifford, D.B.; Sibley, L.D. Genotyping of Toxoplasma gondii Strains from Immunocompromised Patients Reveals High Prevalence of Type I Strains. J. Clin. Microbiol. 2005, 43, 5881–5887. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.; He, L.; Meng, D.; Chen, Z.; Wen, H.; Fang, G.; Luo, Q.; Huang, K.; Shen, J. Seroprevalence and genetic characterization of Toxoplasma gondii in cancer patients in Anhui Province, Eastern China. Parasit. Vectors 2015, 8. [Google Scholar] [CrossRef] [Green Version]
- Dubey, J.P.; Huong, L.T.T.; Lawson, B.W.L.; Subekti, D.T.; Tassi, P.; Cabaj, W.; Sundar, N.; Velmurugan, G.V.; Kwok, O.C.H.; Su, C. Seroprevalence and Isolation of Toxoplasma gondii from Free-Range Chickens in Ghana, Indonesia, Italy, Poland, and Vietnam. J. Parasitol. 2008, 94, 68–72. [Google Scholar] [CrossRef] [PubMed]
- Dubey, J.P.; Huong, L.T.T.; Sundar, N.; Su, C. Genetic characterization of Toxoplasma gondii isolates in dogs from Vietnam suggests their South American origin. Vet. Parasitol. 2007, 146, 347–351. [Google Scholar] [CrossRef] [PubMed]
- Puvanesuaran, V.R.; Noordin, R.; Balakrishnan, V. Isolation and Genotyping of Toxoplasma gondii from Free-Range Ducks in Malaysia. Avian Dis. 2013, 57, 128–132. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Host | Specimen | Sample Size | Test | Manufacturer | Interpretation of Results | Reference |
|---|---|---|---|---|---|---|
| Pregnant women | Blood | 281 | ELISA | BioRad, USA | IgG < 6 IU/mL negative, IgG < 6 IU/mL and 9 IU/mL equivocal, IgG > 9 IU/mL positive | [35] |
| Pregnant women | Blood | 215 | ELISA | IgG & IgM-NovaLisa Dietzenbach, Germany | IgG, IgM and Avidity High avidity past infection (4–5 months). Low avidity, recently acquired (4–5 month) | [36] |
| Patients with disorder | Blood | 102 | ELISA | Bio-Rad, USA | IgG < 0.80 negative, IgG ˃1.0 positive Avidity; <20% acute | [37] |
| Patients with disorder | Blood | 129 | IFAT | na | IgG > 51 IU/mL positive IgM > 51 IU/mL positive | [5] |
| Renal patient | Blood | 247 | ELISA | IgG-Trinity Biotech, New York, NY and IgM-Trinity Biotech, New York, NY) | IgG > 51 IU/mL positive IgM > 51 IU/mL positive Avidity; <40% latent | [38] |
| Healthy community members | Blood | 495 | ELISA | Trinity Biotech, New York, NY | IgG > 51 IU/mL positive IgM > 51 IU/mL positive Avidity; <40% latent | [39] |
| Healthy community members | Blood and stool | 345 | ELISA | Trinity Biotech, USA | IgG and IgM | [40] |
| Migrant workers | Blood Venous/plain | 484 | Trinity Biotech CaptiaTM, New York, USA | IgG ≥ 1.23, positive IgM ≥ 1.23, positive Avidity’ ˃40% latent and ≤40% acute | [41] | |
| Migrant workers | Blood | Migrants, 501 Control 198 | IFAT and ELISA (IgM) | na | 1:64 significant titers. Positive samples diluted two-fold, end point values. IgM dilution 1:100 | [42] |
| Schizophrenic | Blood | Schizophrenic (88) Control (88) | ELISA | RADIM, Italy | na | [43] |
| Schizophrenic | Blood | cases (101) control (55) | ELISA and qPCR | IBL company, Hamburg Germany | IgG and IgM positive more than IU/mL and 11 IU/mL | [44] |
| HIV patient | Blood | 1 | ELISA | na | IgG > 51 IU/mL as positive | [45] |
| Veterinary health professionals & students | Blood | 312 | ELISA | IgG-NovaLisa, Dietzenbach, Germany | ELISA-I, II and III Avidity >40%, chronic, <40% acute. Avidity of <15% (low avidity), acute primary infection Avidity between 15% and 30% (borderline) | [46] |
| Cattle | Blood | 116 | IFAT | na | 1:20 | [47] |
| Domestic animals | Blood | Cat (55), dog (135), goats (200) cattle (126) Pigs (100) | IFAT | na | na | [48] |
| Rats | Blood | 526 | IFAT | na | IgG ≥ 1.64 IgM ≥ 1.4 | [49] |
| Country | Year | G | Design | Subject | Sample Size | S | Test | Findings | Reference |
|---|---|---|---|---|---|---|---|---|---|
| Malaysia | 2014 | Female | Cross-sectional | Pregnant women | 281 | Sera | ELISA | IgG: 35.2%, IgM/IgG: 1.8%, IgG avidity: high and low. The Toxoplasma antibody was confirmed through IgG avidity index, and it was found to be accurate. | [35] |
| Malaysia and Myanmar | 2014 | Female | Cross-sectional | Pregnant women | 219 Malaysia, 215 Myanmar | Sera | ELISA | Malaysia, IgG: 39.7%, IgG and IgM: 2.7%. Myanmar, IgG: 30.2%, IgG and IgM: 0.5%. Malaysian pregnant women were more prone to T. gondii infection in the age group 30 years and above. Lack of awareness was also associated with the infection. | [36] |
| Thailand and Myanmar border | 2017 | Both | Cross-sectional | Pregnant women/ Refugee | 200 | Sera | ELISA | IgG: 31.7%, IgM: 1.5%, IgG avidity: high. The infection is more prevalent in people aged 35 years and above. Similarly, being Muslim was associated with a higher risk of infection. | [57] |
| Thailand | 2011 | Female | Cross-sectional | Pregnant women | 640 | Sera | ELISA | IgG: 21.6%, IgM and IgG: 6.7%, IgG avidity: high. Contact with cats and untreated water are the confirmed risk factors. | [56] |
| Thailand | 2014 | Female | Cross-sectional | Pregnant women | 760 | Sera | ELISA | IgG: 22.0%, IgM: 3.0% IgG avidity: high. Pregnant women 26 years and above working as laborers and untreated water were identified as risk factors. | [55] |
| Country | Year | G | Design | Subject | Sample Size | S | Test | Findings | Reference |
|---|---|---|---|---|---|---|---|---|---|
| Malaysia | 2010 | Both | Cross-sectional | Patients with disorders | 129 | Sera | ELISA | IgM: 0.8%, IgG: 38.8%, IgM and IgG: 2.3%. Highest seroprevalence in the age group 20–41 years old. Malay has the highest IgG positivity (32.0%) and the least is among Indians (1.0%). The younger population are at risk of infection. | [5] |
| Malaysia | 2011 | Both | Cases | Renal patients | 247 | Sera | ELISA | IgG: 31.6%. High prevalence of latent toxoplasmosis in renal patients with older people at high risk. | [56] |
| Malaysia | 2016 | Both | Cross-sectional | Patients with disorders | 102 cases | Sera | ELISA | IgG: 44.1%, IgM: 1.0%. The highest was recorded among patients screened for congenital toxoplasmosis (41.7%) and in children less than one-month-old (37.8%). | [37] |
| Country | Year | G | Design | Subject | Sample Size | S | Test | Finding | Reference |
|---|---|---|---|---|---|---|---|---|---|
| Malaysia | 2008 | Male | Cross-sectional | Foreigners/Migrant workers | 501 Migrants, 198 local Malaysians, 90 Police and Immigration | Sera | IFAT | Migrants—IgG: 34.1%, IgM: 5.2%; Locals—IgG: 44.9%, IgM: 8.6%. All nationalities were seropositive with T. gondii antibodies. Seroprevalence among illegal Indonesian workers was the highest, 54.4%, compared to that among Nepalese workers, 46.2%. Infection not imported, those infected got it at the plantation camp. | [42] |
| Malaysia | 2017 | Both | Cross-sectional | Migrant workers | 484 | Sera | ELISA | IgG: 52.9%, IgM: 0.8%, IgG and IgM: 3.8%, IgG avidity: high. The most common factor associated with the prevalence of the infection is age class. Workers older than 45 years and above were found to be more prone to the infection. Second is the migrant countries of origin, which was also identified as a risk factor. | [41] |
| Country | Year | G | Design | Subject | Sample Size | S | Test | Findings | Reference |
|---|---|---|---|---|---|---|---|---|---|
| Malaysia | 2011 | Both | Cross-sectional | Orang Asli/Indigenous | 495 | Sera | ELISA | IgG: 31.0%, IgM: 1.8%, IgG and IgM: 4.2%, IgG avidity: low. Seroprevalence higher among 12 years and above. Close contact with cats and untreated water as risk factors. | [39] |
| Malaysia | 2014 | Both | Cross-sectional | Pangkor Island | 345 individuals | Stool and Sera | Micros and ELISA | Trichuris trichiura: 5.3%. IgG and IgM: 59.7%. Seroprevalence was 59.7% with the infection being higher in children, in females, and also in Malays compared to Indians and Chinese. | [40] |
| Malaysia | 2015 | Both | Cross-sectional | Veterinary personnel and pet owners | 312 people: Veterinarian Technicians Students | Sera | ELISA | IgG: 18.3%, IgM: 1.0%, IgG and IgM: 0.7%, IgG avidity: low, but no clinical symptoms. Veterinarians: 18.4%, technicians: 33.3%, students: 14.9%, and pet owners: 31.4%. Technicians had the highest risk and vulnerability to the infection. Working duration, age group (above 30 years), and gardening were risk factors. Indians were the highest infected 29.0%. | [46] |
| Country | Year | G | Design | Subject | Sample Size | S | Test | Findings | Reference |
|---|---|---|---|---|---|---|---|---|---|
| Malaysia | 2015 | Both | Case control | Schizophrenic | 101 Schizophrenic patients 55 control | Sera | ELISA and qPCR | Schizophrenic—IgG: 51.5%, IgM: 3.9% DNA: 32.1%; Control—IgG: 18.2%, IgM: 0%, DNA: 3.6%. The study confirmed strong association between T. gondii and schizophrenia. | [44] |
| Malaysia | 2013 | Both | Case-control | Hospital-based | 88 Schizophrenic 88 Control | Sera | ELISA | Schizophrenic—IgG: 51.0%, IgM: 1.1%; Control—IgG: 30.7%, IgM: 1.1%. Beef and pork consumption, and risky cats were significantly associated with the infection. There is an association between T. gondii and schizophrenia. | [43] |
| Country | Genotype | Host | Sample Used for Genotyping | Number of T. gondii Isolates | Reference |
|---|---|---|---|---|---|
| Indonesia | Non clonal | Chicken | Bioassay in mice | 1 | [104] |
| Vietnam | Non clonal | Chicken | Bioassay in mice | 1 | [104,105] |
| Myanmar | type I | Bats | Direct from organs | 19 | [87] |
| Malaysia | type I and II | Ducks | Bioassay in mice | 4 | [106] |
| Malaysia | type I | Wild Boars | Bioassay in mice | 11 | [98] |
| Thailand | type I, III, II or III and recombinant | domestic cat | Direct from feces | 13 | [94] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nasiru Wana, M.; Mohd Moklas, M.A.; Watanabe, M.; Nordin, N.; Zasmy Unyah, N.; Alhassan Abdullahi, S.; Ahmad Issa Alapid, A.; Mustapha, T.; Basir, R.; Abd. Majid, R. A Review on the Prevalence of Toxoplasma gondii in Humans and Animals Reported in Malaysia from 2008–2018. Int. J. Environ. Res. Public Health 2020, 17, 4809. https://doi.org/10.3390/ijerph17134809
Nasiru Wana M, Mohd Moklas MA, Watanabe M, Nordin N, Zasmy Unyah N, Alhassan Abdullahi S, Ahmad Issa Alapid A, Mustapha T, Basir R, Abd. Majid R. A Review on the Prevalence of Toxoplasma gondii in Humans and Animals Reported in Malaysia from 2008–2018. International Journal of Environmental Research and Public Health. 2020; 17(13):4809. https://doi.org/10.3390/ijerph17134809
Chicago/Turabian StyleNasiru Wana, Mohammed, Mohamad Aris Mohd Moklas, Malaika Watanabe, Norshariza Nordin, Ngah Zasmy Unyah, Sharif Alhassan Abdullahi, Ashraf Ahmad Issa Alapid, Tijjani Mustapha, Rusliza Basir, and Roslaini Abd. Majid. 2020. "A Review on the Prevalence of Toxoplasma gondii in Humans and Animals Reported in Malaysia from 2008–2018" International Journal of Environmental Research and Public Health 17, no. 13: 4809. https://doi.org/10.3390/ijerph17134809