Analyzing the Association between Hyperuricemia and Periodontitis: A Cross-Sectional Study Using KoGES HEXA Data


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Data Collection
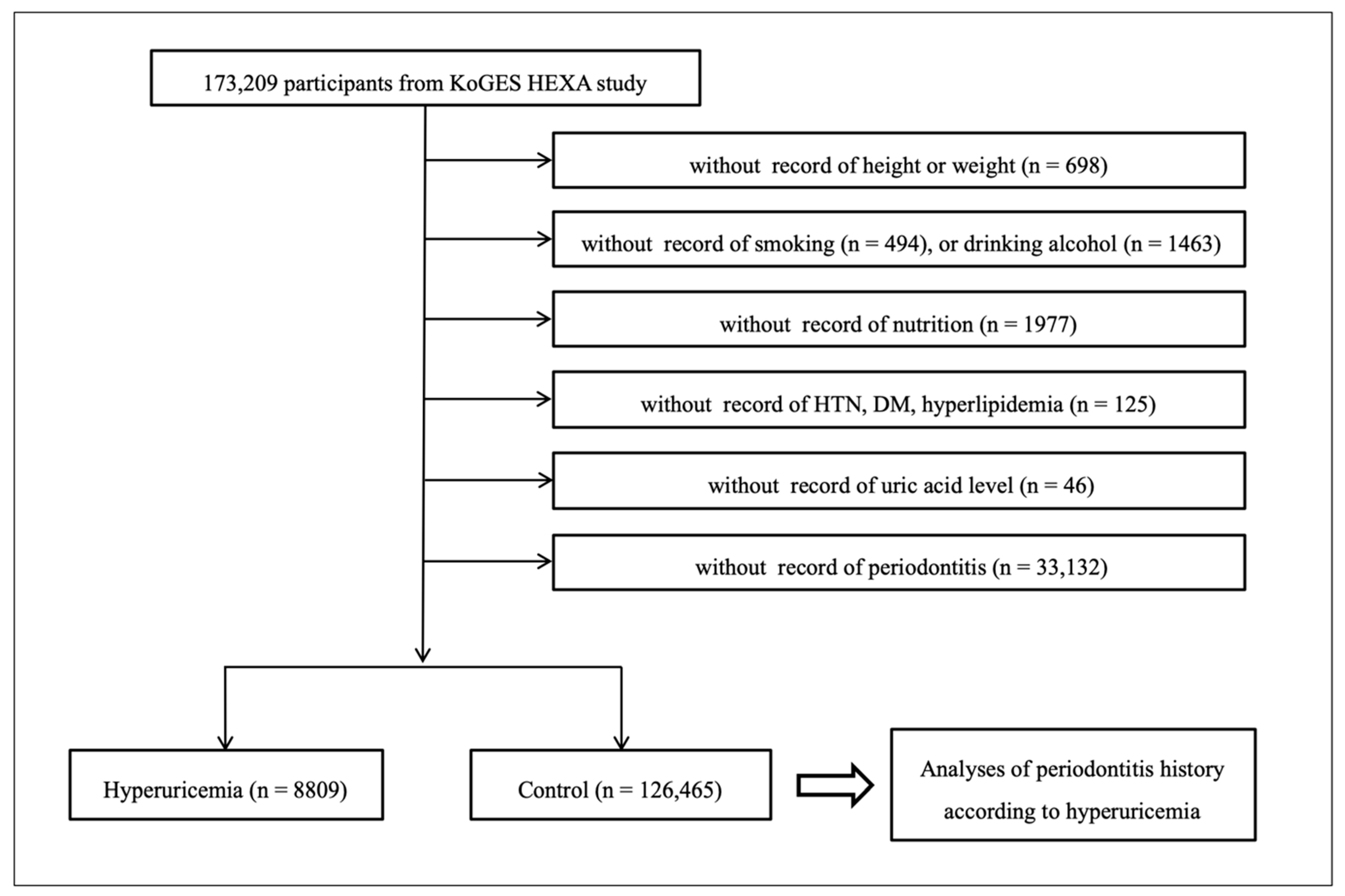
2.2. Participant Selection
2.3. Survey
2.4. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Grassi, D.; Ferri, L.; Desideri, G.; Di Giosia, P.; Cheli, P.; Del Pinto, R.; Properzi, G.; Ferri, C. Chronic hyperuricemia, uric acid deposit and cardiovascular risk. Curr. Pharm. Des. 2013, 19, 2432–2438. [Google Scholar] [CrossRef] [Green Version]
- Kang, M.W.; Chin, H.J.; Joo, K.W.; Na, K.Y.; Kim, S.; Han, S.S. Hyperuricemia is associated with acute kidney injury and all-cause mortality in hospitalized patients. Nephrology 2019, 24, 718–724. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.K.; McCormick, N.; Lu, N.; Rai, S.K.; Yokose, C.; Zhang, Y. Population Impact Attributable to Modifiable Risk Factors for Hyperuricemia. Arthritis Rheumatol. 2020, 72, 157–165. [Google Scholar] [CrossRef]
- Chen, J.H.; Yeh, W.T.; Chuang, S.Y.; Wu, Y.Y.; Pan, W.H. Gender-specific risk factors for incident gout: A prospective cohort study. Clin. Rheumatol. 2012, 31, 239–245. [Google Scholar] [CrossRef] [PubMed]
- George, C.; Minter, D.A. Hyperuricemia; StatPearls: Treasure Island, FL, USA, 2020. [Google Scholar]
- Stewart, D.J.; Langlois, V.; Noone, D. Hyperuricemia and Hypertension: Links and Risks. Integr. Blood Press. Control 2019, 12, 43–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeng, F.; Huang, R.; Lu, Y.; Wu, Z.; Wang, L. Association of anti-hyperuricemia treatment and prevalent cardiovascular disease in hypertensive patients. Arch. Med. Sci. 2020, 16, 545–550. [Google Scholar] [CrossRef]
- Li, C.; Hsieh, M.C.; Chang, S.J. Metabolic syndrome, diabetes, and hyperuricemia. Curr. Opin. Rheumatol. 2013, 25, 210–216. [Google Scholar] [CrossRef]
- Hood, B.; Olander, R. Kidneys, uric acid secretion and hyperuricemia. Lakartidningen 1968, 65, 561–566. [Google Scholar]
- Nakamura, T.; Takagi, K.; Ueda, T. Dynamics of uric acid metabolism in hyperuricemia. Nihon Rinsho 1996, 54, 3230–3236. [Google Scholar]
- Kumar, R.; Khalsa, D.D.; Carmody, J.B. Serum uric acid and hyperuricemia in U.S. adolescents: 40-year trends. Clin. Exp. Rheumatol. 2016, 34, S22–S23. [Google Scholar]
- Borghi, C. The management of hyperuricemia: Back to the pathophysiology of uric acid. Curr. Med. Res. Opin. 2017, 33, 1–4. [Google Scholar] [CrossRef]
- Alqarni, N.A.; Hassan, A.H. Knowledge and practice in the management of asymptomatic hyperuricemia among primary health care physicians in Jeddah, Western Region of Saudi Arabia. Saudi Med. J. 2018, 39, 1218–1225. [Google Scholar] [CrossRef] [PubMed]
- Yang, N.; Yu, Y.; Zhang, A.; Estill, J.; Wang, X.; Zheng, M.; Zhou, Q.; Zhang, J.; Luo, X.; Qian, C.; et al. Reporting, presentation and wording of recommendations in clinical practice guideline for gout: A systematic analysis. BMJ Open 2019, 9, e024315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dioguardi, M.; Crincoli, V.; Laino, L.; Alovisi, M.; Sovereto, D.; Mastrangelo, F.; Russo, L.L.; Muzio, L.L. The Role of Periodontitis and Periodontal Bacteria in the Onset and Progression of Alzheimer’s Disease: A Systematic Review. J. Clin. Med. 2020, 9, 495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kononen, E.; Gursoy, M.; Gursoy, U.K. Periodontitis: A Multifaceted Disease of Tooth-Supporting Tissues. J. Clin. Med. 2019, 8, 1135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Preshaw, P.M.; Taylor, J.J. How has research into cytokine interactions and their role in driving immune responses impacted our understanding of periodontitis? J. Clin. Periodontol. 2011, 38, 60–84. [Google Scholar] [CrossRef]
- Pihlstrom, B.L.; Michalowicz, B.S.; Johnson, N.W. Periodontal diseases. Lancet 2005, 366, 1809–1820. [Google Scholar] [CrossRef] [Green Version]
- Bullon, P.; Newman, H.N.; Battino, M. Obesity, diabetes mellitus, atherosclerosis and chronic periodontitis: A shared pathology via oxidative stress and mitochondrial dysfunction? Periodontol. 2000 2014, 64, 139–153. [Google Scholar] [CrossRef]
- Isola, G.; Matarese, G.; Ramaglia, L.; Pedulla, E.; Rapisarda, E.; Iorio-Siciliano, V. Association between periodontitis and glycosylated haemoglobin before diabetes onset: A cross-sectional study. Clin. Oral Investig. 2019. [Google Scholar] [CrossRef]
- Isola, G.; Alibrandi, A.; Curro, M.; Matarese, M.; Ricca, S.; Matarese, G.; Ientile, R.; Kocher, T. Evaluation of salivary and serum ADMA levels in patients with periodontal and cardiovascular disease as subclinical marker of cardiovascular risk. J. Periodontol. 2020. [Google Scholar] [CrossRef]
- Isola, G.; Alibrandi, A.; Rapisarda, E.; Matarese, G.; Williams, R.C.; Leonardi, R. Association of vitamin D in patients with periodontitis: A cross-sectional study. J. Periodontal. Res. 2020. [Google Scholar] [CrossRef] [PubMed]
- Isola, G. Current Evidence of Natural Agents in Oral and Periodontal Health. Nutrients 2020, 12, 585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tamayo, Y.O.J.A. Systemic Implications of Hyperuricemia. Contrib. Nephrol. 2018, 192, 82–87. [Google Scholar] [CrossRef]
- Chen, Z.Y.; Ye, L.W.; Zhao, L.; Liang, Z.J.; Yu, T.; Gao, J. Hyperuricemia as a potential plausible risk factor for periodontitis. Med. Hypotheses 2020, 137, 109591. [Google Scholar] [CrossRef]
- Stack, A.; Manolis, A.J.; Ritz, E. Detrimental role of hyperuricemia on the cardio-reno-vascular system. Curr. Med. Res. Opin. 2015, 31 (Suppl. 2), 21–26. [Google Scholar] [CrossRef]
- Madianov, I.V.; Balabolkin, M.I.; Markov, D.S.; Markova, T.N. Main causes of hyperuricemia in diabetes mellitus. Ter. Arkh. 2000, 72, 55–58. [Google Scholar]
- Banu, S.; Jabir, N.R.; Mohan, R.; Manjunath, N.C.; Kamal, M.A.; Kumar, K.R.; Zaidi, S.K.; Khan, M.S.; Tabrez, S. Correlation of Toll-like receptor 4, interleukin-18, transaminases, and uric acid in patients with chronic periodontitis and healthy adults. J. Periodontol. 2015, 86, 431–439. [Google Scholar] [CrossRef]
- Prieto, A.K.C.; Gomes-Filho, J.E.; Azuma, M.M.; Sivieri-Araujo, G.; Narciso, L.G.; Souza, J.C.; Ciarlini, P.C.; Cintra, L.T.A. Influence of Apical Periodontitis on Stress Oxidative Parameters in Diabetic Rats. J. Endod. 2017, 43, 1651–1656. [Google Scholar] [CrossRef] [Green Version]
- Zhou, J.; Hu, H.; Huang, R. A pilot study of the metabolomic profiles of saliva from female orthodontic patients with external apical root resorption. Clin. Chim. Acta 2018, 478, 188–193. [Google Scholar] [CrossRef]
- Cao, Y.L.; Qiao, M.; Xu, Z.H.; Zou, G.M.; Ma, L.L.; Li, W.G.; Xu, B.H. The clinical study of IgA nephropathy with severe chronic periodontitis and aggressive periodontitis. Zhonghua Yi Xue Za Zhi 2016, 96, 9–13. [Google Scholar] [CrossRef]
- Kuraji, R.; Fujita, M.; Ito, H.; Hashimoto, S.; Numabe, Y. Effects of experimental periodontitis on the metabolic system in rats with diet-induced obesity (DIO): An analysis of serum biochemical parameters. Odontology 2018, 106, 162–170. [Google Scholar] [CrossRef] [PubMed]
- Babaei, H.; Forouzandeh, F.; Maghsoumi-Norouzabad, L.; Yousefimanesh, H.A.; Ravanbakhsh, M.; Zare Javid, A. Effects of Chicory Leaf Extract on Serum Oxidative Stress Markers, Lipid Profile and Periodontal Status in Patients With Chronic Periodontitis. J. Am. Coll. Nutr. 2018, 37, 479–486. [Google Scholar] [CrossRef]
- Kim, Y.; Han, B.G.; KoGES Group. Cohort Profile: The Korean Genome and Epidemiology Study (KoGES) Consortium. Int. J. Epidemiol. 2017, 46, 1350. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Pandya, B.J.; Choi, H.K. Prevalence of gout and hyperuricemia in the US general population: The National Health and Nutrition Examination Survey 2007–2008. Arthritis Rheum. 2011, 63, 3136–3141. [Google Scholar] [CrossRef] [PubMed]
- Lin, K.C.; Lin, H.Y.; Chou, P. Community based epidemiological study on hyperuricemia and gout in Kin-Hu, Kinmen. J. Rheumatol. 2000, 27, 1045–1050. [Google Scholar] [PubMed]
- Ahn, Y.; Kwon, E.; Shim, J.E.; Park, M.K.; Joo, Y.; Kimm, K.; Park, C.; Kim, D.H. Validation and reproducibility of food frequency questionnaire for Korean genome epidemiologic study. Eur. J. Clin. Nutr. 2007, 61, 1435–1441. [Google Scholar] [CrossRef] [PubMed]
- Daudt, L.D.; Musskopf, M.L.; Mendez, M.; Remonti, L.L.R.; Leitao, C.B.; Gross, J.L.; Weidlich, P.; Oppermann, R.V. Association between metabolic syndrome and periodontitis: A systematic review and meta-analysis. Braz. Oral Res. 2018, 32, e35. [Google Scholar] [CrossRef] [Green Version]
- Arboleda, S.; Vargas, M.; Losada, S.; Pinto, A. Review of obesity and periodontitis: An epidemiological view. Br. Dent. J. 2019, 227, 235–239. [Google Scholar] [CrossRef]
- Chapple, I.L.; Genco, R.; Working Group 2 of Joint EFP/AAP Workshop. Diabetes and periodontal diseases: Consensus report of the Joint EFP/AAP Workshop on Periodontitis and Systemic Diseases. J. Periodontol. 2013, 84, S106–S112. [Google Scholar] [CrossRef]
- Lamster, I.B.; Pagan, M. Periodontal disease and the metabolic syndrome. Int. Dent. J. 2017, 67, 67–77. [Google Scholar] [CrossRef]
- Ali, N.; Perveen, R.; Rahman, S.; Mahmood, S.; Rahman, S.; Islam, S.; Haque, T.; Sumon, A.H.; Kathak, R.R.; Molla, N.H.; et al. Prevalence of hyperuricemia and the relationship between serum uric acid and obesity: A study on Bangladeshi adults. PLoS ONE 2018, 13, e0206850. [Google Scholar] [CrossRef] [Green Version]
- Cortese, F.; Giordano, P.; Scicchitano, P.; Faienza, M.F.; De Pergola, G.; Calculli, G.; Meliota, G.; Ciccone, M.M. Uric acid: From a biological advantage to a potential danger. A focus on cardiovascular effects. Vascul. Pharmacol. 2019, 120, 106565. [Google Scholar] [CrossRef] [PubMed]
- Friedewald, V.E.; Kornman, K.S.; Beck, J.D.; Genco, R.; Goldfine, A.; Libby, P.; Offenbacher, S.; Ridker, P.M.; Van Dyke, T.E.; Roberts, W.C.; et al. The American Journal of Cardiology and Journal of Periodontology Editors’ Consensus: Periodontitis and atherosclerotic cardiovascular disease. Am. J. Cardiol. 2009, 104, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Seymour, G.J.; Palmer, J.E.; Leishman, S.J.; Do, H.L.; Westerman, B.; Carle, A.D.; Faddy, M.J.; West, M.J.; Cullinan, M.P. Influence of a triclosan toothpaste on periodontopathic bacteria and periodontitis progression in cardiovascular patients: A randomized controlled trial. J. Periodontal. Res. 2017, 52, 61–73. [Google Scholar] [CrossRef] [PubMed]
- Holmlund, A.; Holm, G.; Lind, L. Number of teeth as a predictor of cardiovascular mortality in a cohort of 7674 subjects followed for 12 years. J. Periodontol. 2010, 81, 870–876. [Google Scholar] [CrossRef]
- Kebschull, M.; Demmer, R.T.; Papapanou, P.N. “Gum bug, leave my heart alone!”—Epidemiologic and mechanistic evidence linking periodontal infections and atherosclerosis. J. Dent. Res. 2010, 89, 879–902. [Google Scholar] [CrossRef] [Green Version]
- Veronese, N.; Carraro, S.; Bano, G.; Trevisan, C.; Solmi, M.; Luchini, C.; Manzato, E.; Caccialanza, R.; Sergi, G.; Nicetto, D.; et al. Hyperuricemia protects against low bone mineral density, osteoporosis and fractures: A systematic review and meta-analysis. Eur. J. Clin. Investig. 2016, 46, 920–930. [Google Scholar] [CrossRef]
- Khodaii, Z.; Mehrabani, M.; Rafieian, N.; Najafi-Parizi, G.A.; Mirzaei, A.; Akbarzadeh, R. Altered levels of salivary biochemical markers in periodontitis. Am. J. Dent. 2019, 32, 183–186. [Google Scholar]


{kind=link}
| Characteristics | Total Participants | p-Value | |
|---|---|---|---|
| Hyperuricemia | Control | ||
| Age (mean, SD, year) | 54.8 (7.9) | 53.0 (8.3) | <0.001 * |
| Gender (n, %) | <0.001 * | ||
| Men | 5949 (67.5) | 41,298 (32.7) | |
| Women | 2860 (32.5) | 85,167 (67.3) | |
| BMI (mean, SD, kg/m2) | 24.0 (2.9) | 23.9 (2.9) | <0.001 * |
| Income (n, %) | 0.086 | ||
| Missing, no response | 767 (8.7) | 10,847 (8.6) | |
| Low | 2562 (29.1) | 36,456 (28.8) | |
| Middle | 3352 (38.1) | 49,739 (39.3) | |
| High | 2128 (24.2) | 29,423 (23.3) | |
| Smoking status (n, %) | <0.001 * | ||
| Non-smoker | 4174 (47.4) | 93,620 (74.0) | |
| Past smoker | 2735 (31.0) | 17,652 (14.0) | |
| Current smoker | 1900 (21.6) | 15,193 (12.0) | |
| Alcohol consumption (n, %) | <0.001 * | ||
| Non-drinker | 2979 (33.8) | 65,834 (52.1) | |
| Past drinker | 505 (5.7) | 4509 (3.6) | |
| Current drinker | 5325 (60.4) | 56,122 (44.4) | |
| Hypertension | 3663 (41.6) | 27,181 (21.5) | <0.001 * |
| Diabetes mellitus | 986 (11.2) | 10,003 (7.9) | <0.001 * |
| Hyperlipidemia | 1695 (19.2) | 17,996 (14.2) | <0.001 * |
| Nutritional intake | |||
| Total calories (kcal/day) | 1760.2 (580.6) | 1749.4 (569.5) | 0.070 |
| Protein (g/day) | 58.9 (26.6) | 59.8 (26.4) | <0.002 * |
| Fat (g/day) | 27.5 (18.5) | 28.3 (18.2) | <0.001 * |
| Carbohydrate (g/day) | 315.0 (95.2) | 309.8 (92.8) | <0.001 * |
| Periodontitis (n, %) | 657 (7.5) | 9319 (7.4) | 0.756 |
| Characteristics | Odds Ratios for Periodontitis | |||
|---|---|---|---|---|
| Crude | p-Value | Adjusted † | p-Value | |
| Total participants (n = 135,274) | ||||
| Hyperuricemia | 1.01 (0.93–1.10) | 0.756 | 0.89 (0.81–0.96) | 0.005 * |
| Control | 1.00 | 1.00 | ||
| Age ≤ 52 years old, men (n = 21,504) | ||||
| Hyperuricemia | 0.83 (0.70–0.98) | 0.031 * | 0.82 (0.69–0.98) | 0.027 * |
| Control | 1.00 | 1.00 | ||
| Age ≤ 52 years old, women (n = 45,454) | ||||
| Hyperuricemia | 0.91 (0.66–1.24) | 0.546 | 0.77 (0.56–1.05) | 0.100 |
| Control | 1.00 | 1.00 | ||
| Age ≥ 53 years old, men (n = 25,743) | ||||
| Hyperuricemia | 0.99 (0.87–1.13) | 0.900 | 0.96 (0.84–1.09) | 0.506 |
| Control | 1.00 | 1.00 | ||
| Age ≥ 53 years old, women (n = 42,573) | ||||
| Hyperuricemia | 0.92 (0.78–1.09) | 0.320 | 0.87 (0.73–1.03) | 0.101 |
| Control | 1.00 | 1.00 | ||
| Characteristics | Odds Ratios for Periodontitis | |||
|---|---|---|---|---|
| Crude | p-Value | Adjusted † | p-Value | |
| With hypertension (n = 30,844) | ||||
| Hyperuricemia | 1.02 (0.90–1.15) | 0.773 | 0.97 (0.86–1.10) | 0.613 |
| Control | 1.00 | 1.00 | ||
| Without hypertension (n = 104,430) | ||||
| Hyperuricemia | 0.90 (0.80–1.01) | 0.072 | 0.82 (0.73–0.92) | 0.001 * |
| Control | 1.00 | 1.00 | ||
| With diabetes mellitus (n = 10,989) | ||||
| Hyperuricemia | 0.92 (0.74–1.15) | 0.476 | 0.88 (0.70–1.09) | 0.234 |
| Control | 1.00 | 1.00 | ||
| Without diabetes mellitus (n = 124,285) | ||||
| Hyperuricemia | 1.01 (0.92–1.10) | 0.850 | 0.89 (0.81–0.97) | 0.010 * |
| Control | 1.00 | 1.00 | ||
| With hyperlipidemia (n = 19,691) | ||||
| Hyperuricemia | 0.92 (0.79–1.09) | 0.342 | 0.87 (0.74–1.03) | 0.112 |
| Control | 1.00 | 1.00 | ||
| Without hyperlipidemia (n = 115,583) | ||||
| Hyperuricemia | 1.00 (0.91–1.10) | 0.973 | 0.89 (0.80–0.98) | 0.021 * |
| Control | 1.00 | 1.00 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Byun, S.-H.; Yoo, D.-M.; Lee, J.-W.; Choi, H.-G. Analyzing the Association between Hyperuricemia and Periodontitis: A Cross-Sectional Study Using KoGES HEXA Data. Int. J. Environ. Res. Public Health 2020, 17, 4777. https://doi.org/10.3390/ijerph17134777
Byun S-H, Yoo D-M, Lee J-W, Choi H-G. Analyzing the Association between Hyperuricemia and Periodontitis: A Cross-Sectional Study Using KoGES HEXA Data. International Journal of Environmental Research and Public Health. 2020; 17(13):4777. https://doi.org/10.3390/ijerph17134777
Chicago/Turabian StyleByun, Soo-Hwan, Dae-Myoung Yoo, Jung-Woo Lee, and Hyo-Geun Choi. 2020. "Analyzing the Association between Hyperuricemia and Periodontitis: A Cross-Sectional Study Using KoGES HEXA Data" International Journal of Environmental Research and Public Health 17, no. 13: 4777. https://doi.org/10.3390/ijerph17134777