RGB-D-Based Framework to Acquire, Visualize and Measure the Human Body for Dietetic Treatments †

 ,
,  ,
, 
Abstract
:1. Introduction
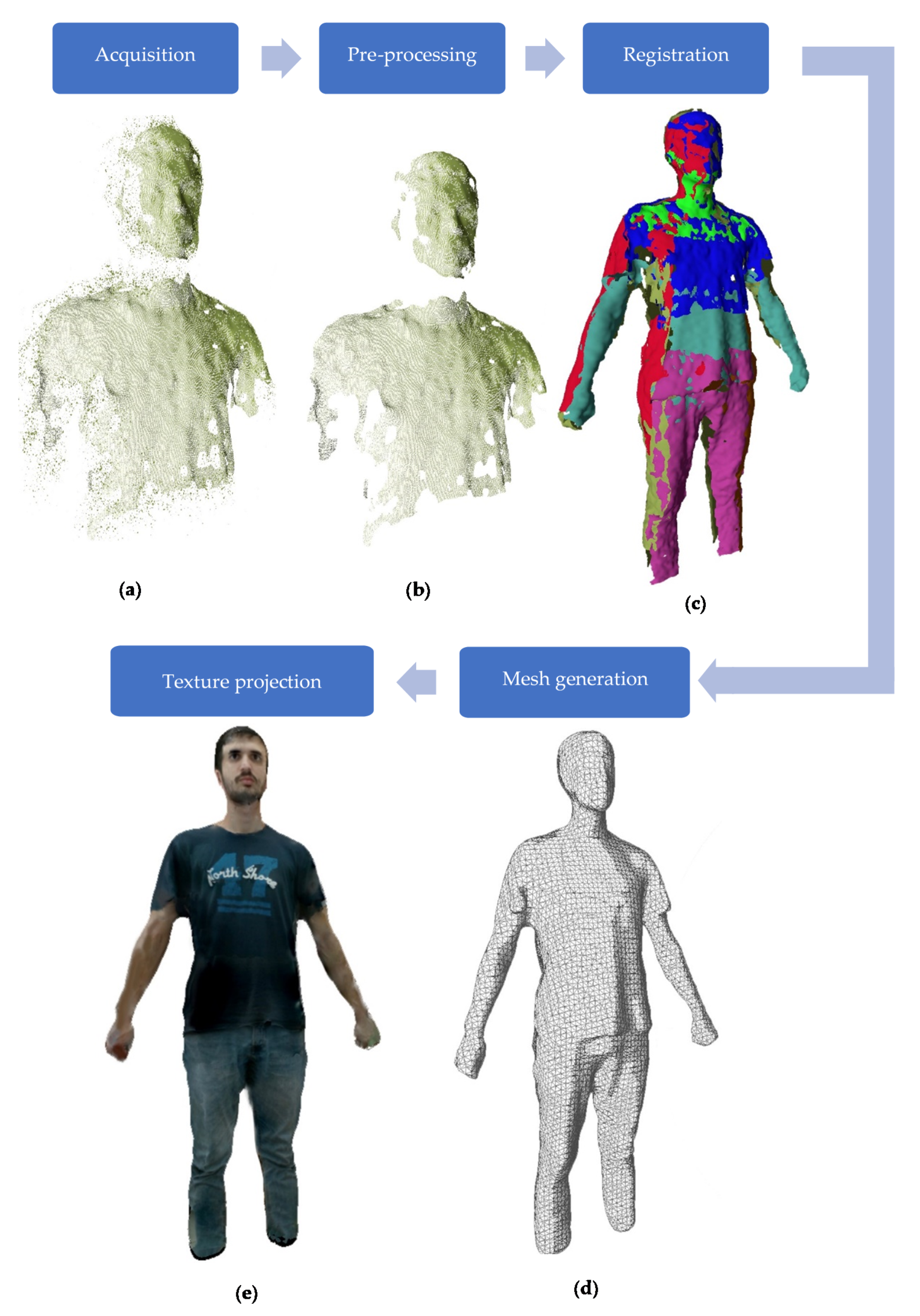
- Obtaining the 3D/4D model: Complete (i.e., from all sides) 3D acquisition of the human body using a low cost RGB-D camera network, obtaining the 3D geometric model and the texture representation of sequences of bodies over time (4D).
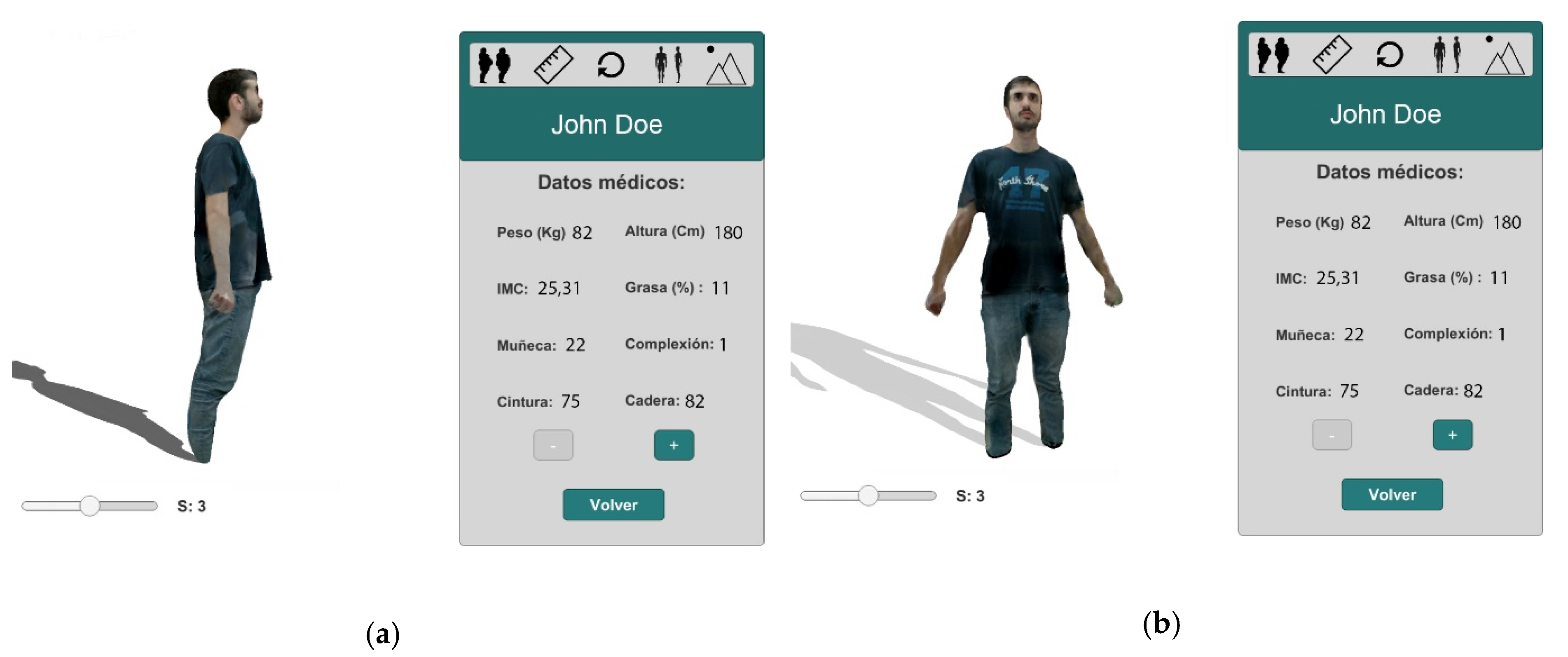
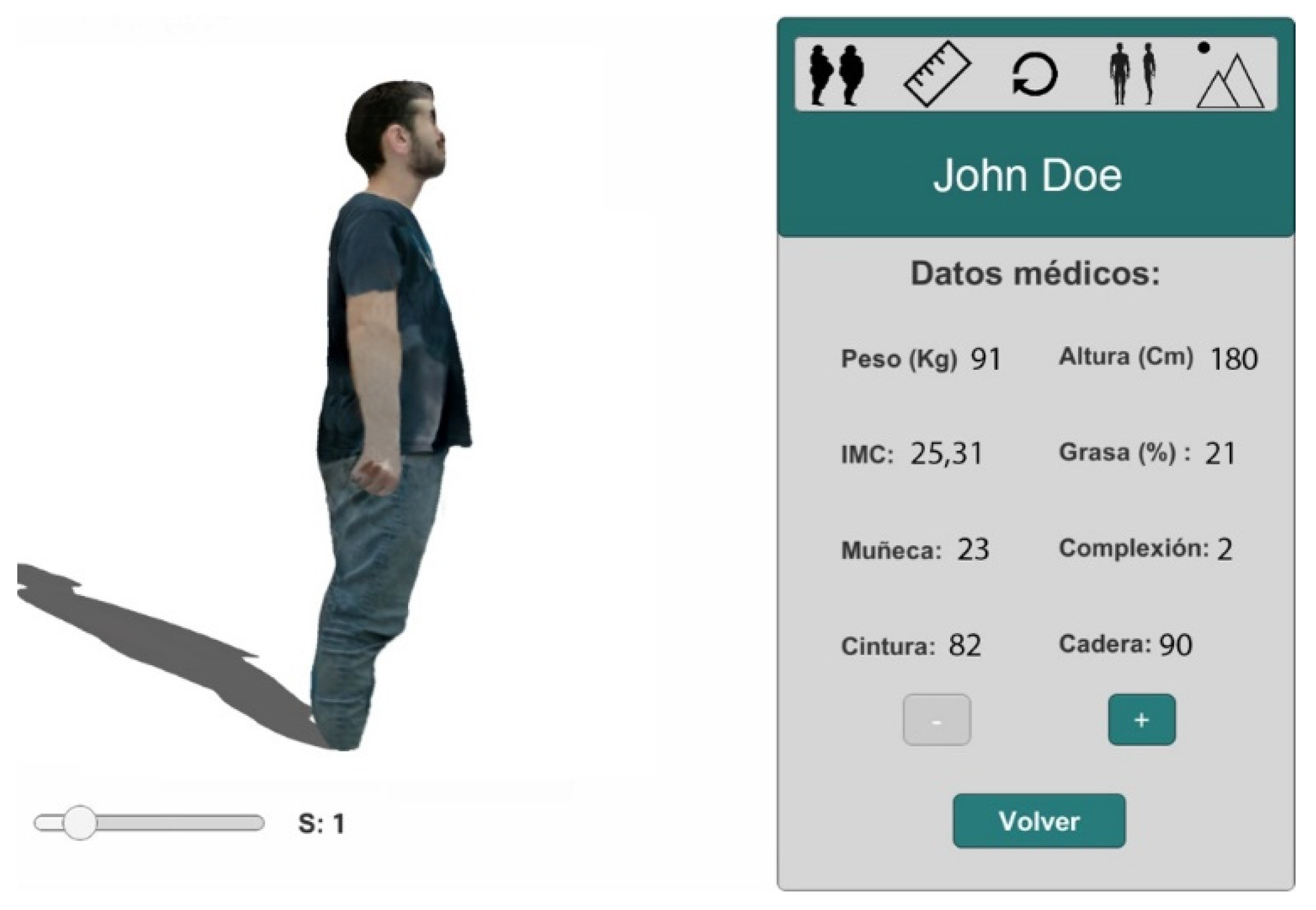
- Visualization of the 3D body: From the 3D models captured over time, realistic visualizations of the body evolution are generated using virtual reality.
- Measuring selected volumes of the human body: Selection of different parts of the human body to obtain 1D, 2D and 3D measurements.
2. Materials and Methods
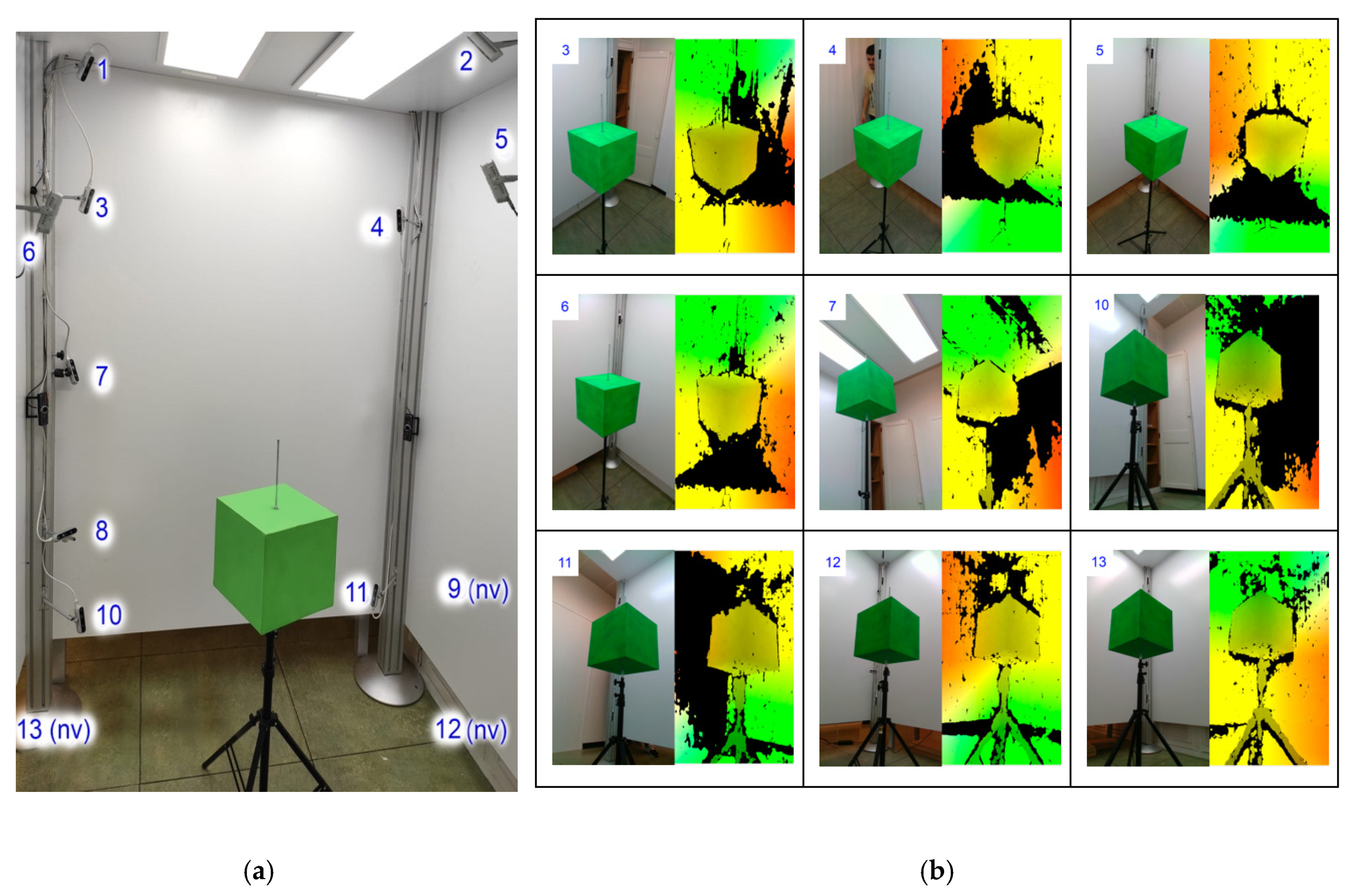
2.1. 3D Reconstruction of the Human Body from Multiple RGB-D Views
2.1.1. Calibration
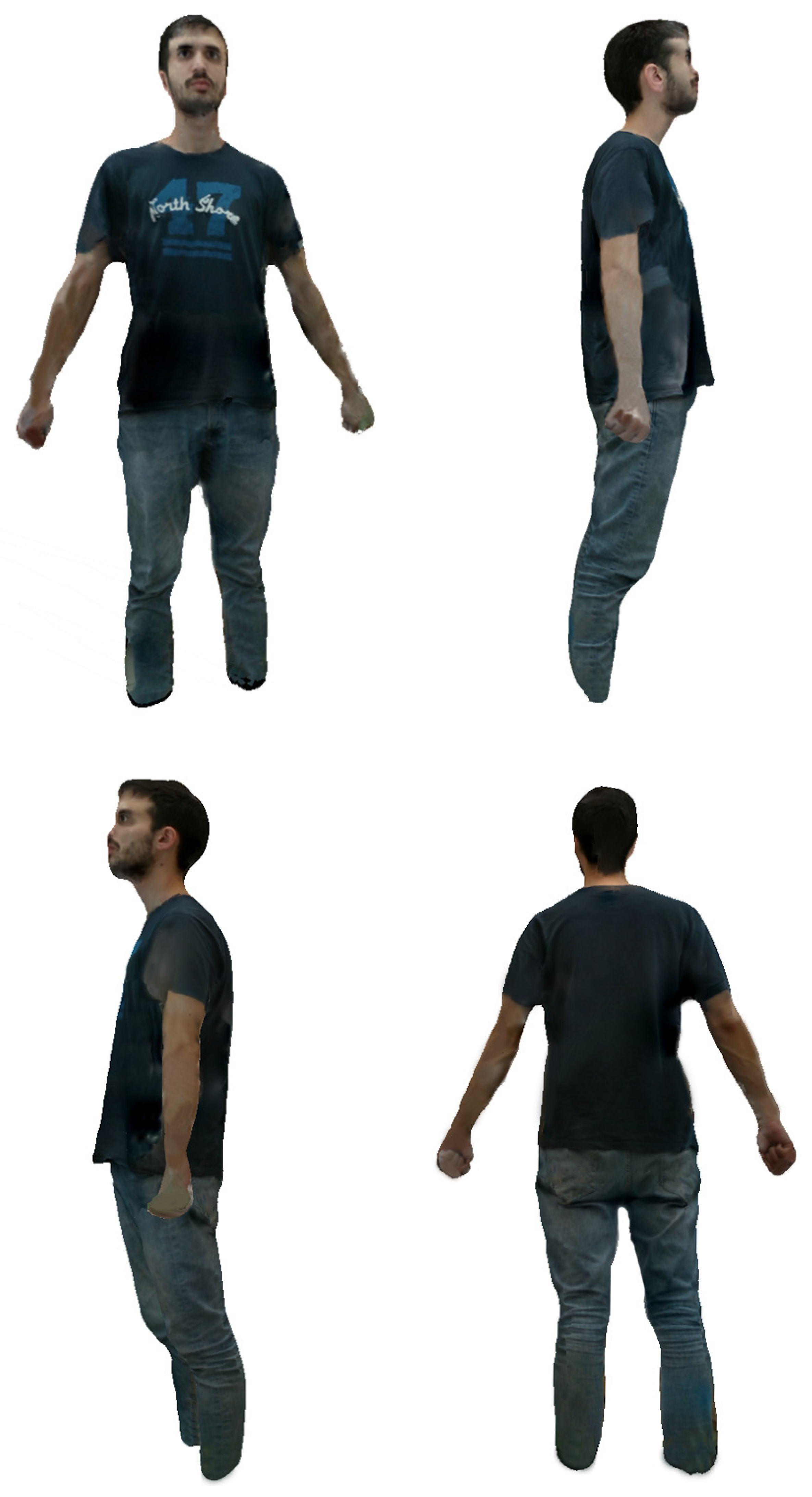
2.1.2. 3D Model Generation
2.2. Visualization of the Human Body Using Virtual Reality for Obesity Treatment Improvement
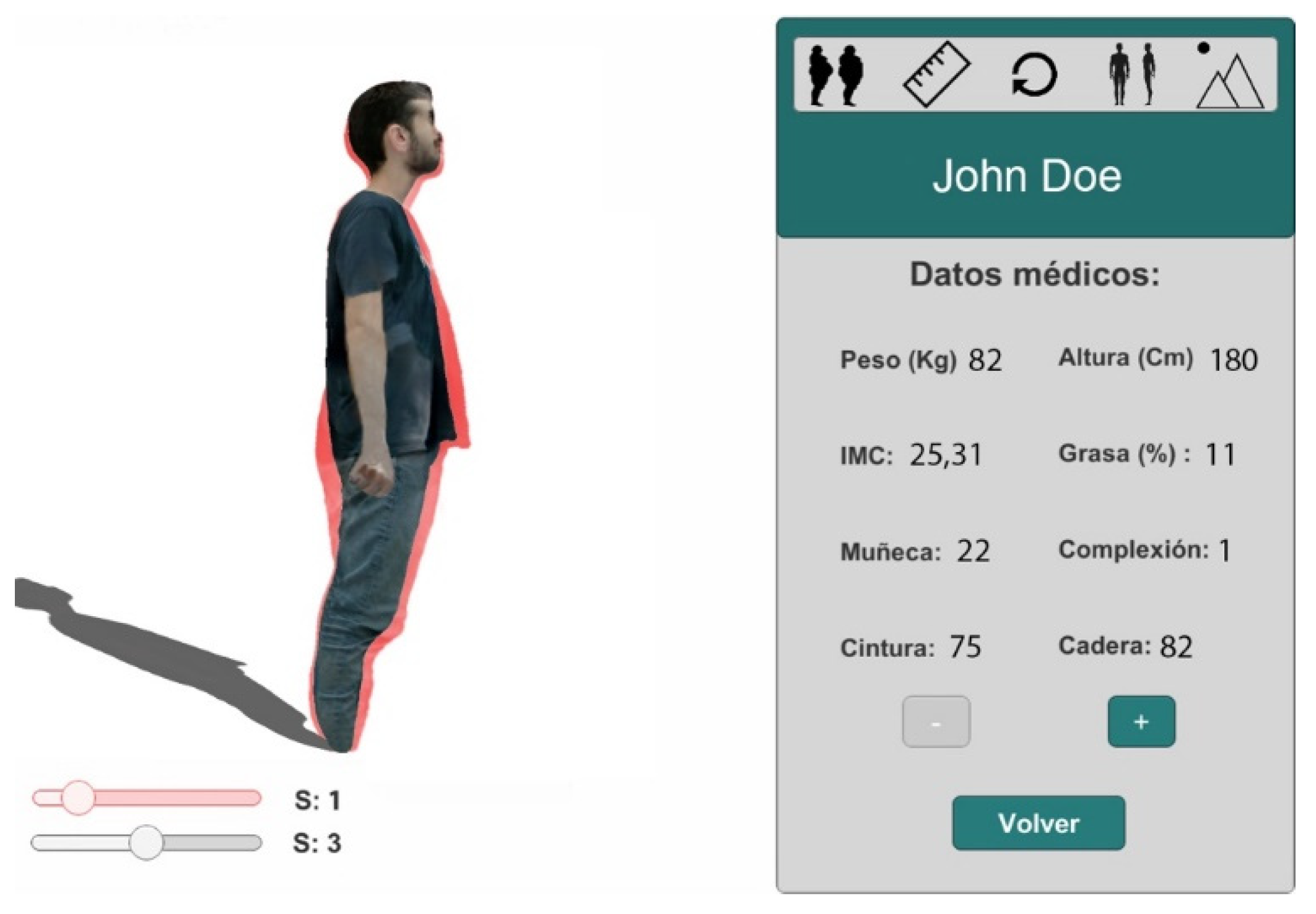
2.2.1. Specialist 4D Image Visualization System for Obesity Treatment
2.2.2. Virtual Reality System
2.3. Body Measuring Methods
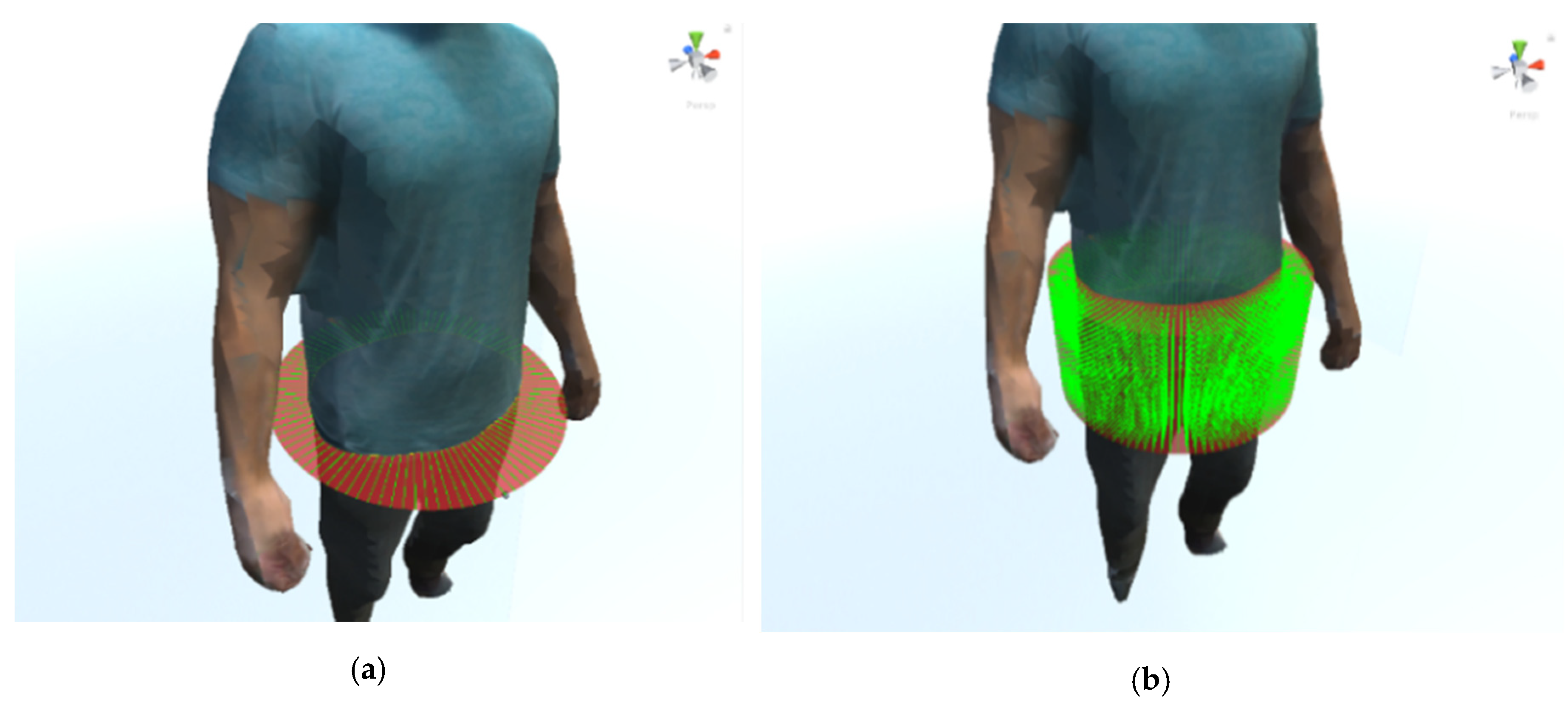
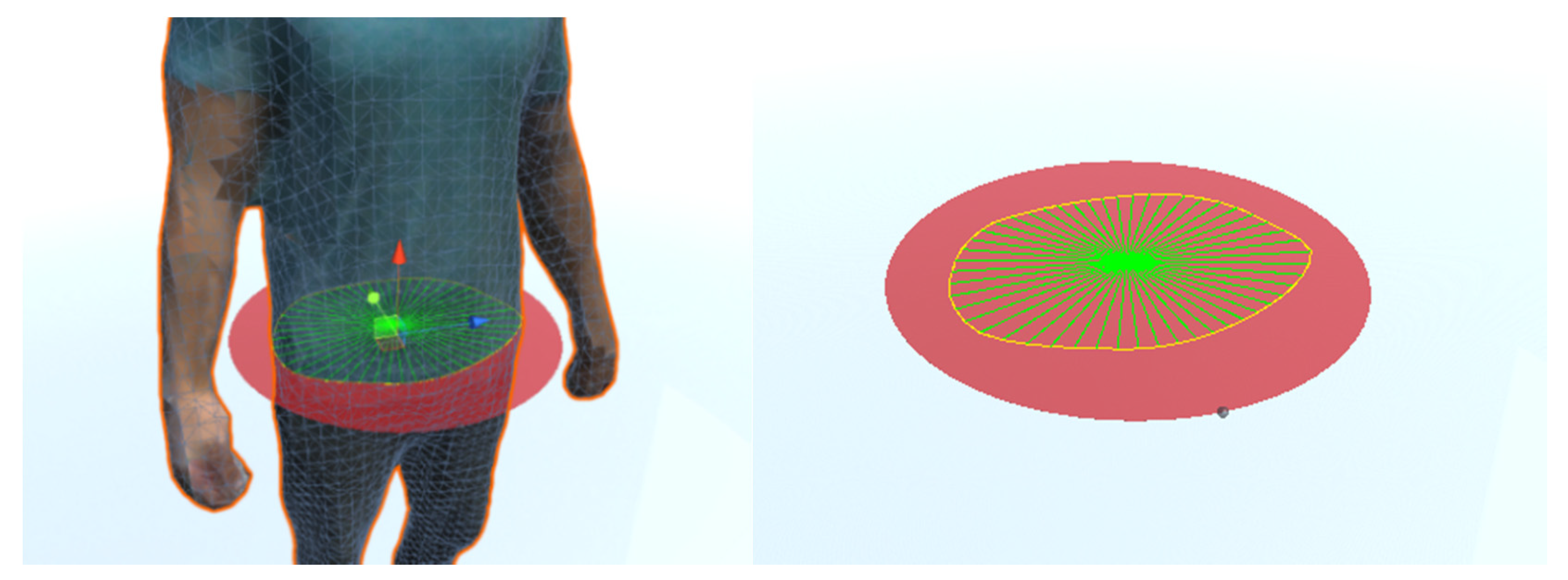
2.3.1. Perimetral Measurement Method
2.3.2. Estimation of Area and Volume
3. Results
3.1. Quantifying the Accuracy of the Method for Measuring Scanned 3D Models
3.1.1. Experimentation with Synthetic 3D Models
3.1.2. Experimentation with Real 3D Objects
3.2. Body Model Visualization
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Boraxbekk, C.J.; Stomby, A.; Ryberg, M.; Lindahl, B.; Larsson, C.; Nyberg, L.; Olsson, T. Diet-induced weight loss alters functional brain responses during an episodic memory task. Obes. Facts 2015, 8, 261–272. [Google Scholar] [CrossRef] [PubMed]
- Drigny, J.; Gremeaux, V.; Dupuy, O.; Gayda, M.; Bherer, L.; Juneau, M.; Nigam, A. Effect of interval training on cognitive functioning and cerebral oxygenation in obese patients: A pilot study. J. Rehabil. Med. 2014, 46, 1050–1054. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lehnert, T.; Sonntag, D.; Konnopka, A.; Riedel-Heller, S.; König, H.-H. Economic costs of overweight and obesity. Best Pract. Res. Clin. Endocrinol. Metab. 2013, 27, 105–115. [Google Scholar] [CrossRef] [PubMed]
- Withrow, D.; Alter, D.A. The economic burden of obesity worldwide: A systematic review of the direct costs of obesity. Obes. Rev. 2011. [Google Scholar] [CrossRef] [PubMed]
- Sicras-Mainar, A.; Gil, J.; Mora, T.; Ayma, J. Prevalencia e impacto económico de la obesidad en adultos durante el periodo 2003–2010. Med. Clin. 2012. [Google Scholar] [CrossRef] [PubMed]
- De Geest, S.; Sabaté, E. Adherence to long-term therapies: Evidence for action. Eur. J. Cardiovasc. Nurs. 2003. [Google Scholar] [CrossRef]
- Boeka, A.; Lokken, K. Neuropsychological performance of a clinical sample of extremely obese individuals. Arch. Clin. Neuropsychol. 2008. [Google Scholar] [CrossRef] [Green Version]
- Roseman, M.G.; Riddell, M.C.; Haynes, J.N. A content analysis of kindergarten-12th grade school-based nutrition interventions: Taking advantage of past learning. J. Nutr. Educ. Behav. 2011. [Google Scholar] [CrossRef]
- Ajie, W.N.; Chapman-Novakofski, K.M. Impact of computer-mediated, obesity-related nutrition education interventions for adolescents: A systematic review. J. Adolesc. Heal. 2014. [Google Scholar] [CrossRef] [Green Version]
- Ferrer-Garcia, M.; Gutiérrez-Maldonado, J.; Riva, G. Virtual reality based treatments in eating disorders and obesity: A review. J. Contemp. Psychother. 2013, 43, 207–221. [Google Scholar] [CrossRef]
- Kuzmar, I.; Rizo, M.; Cortés-Castell, E. Adherence to an overweight and obesity treatment: How to motivate a patient. PeerJ 2014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuster-Guilló, A.; Azorín-López, J.; Zaragoza, J.M.C.; Pérez, L.F.P.; Saval-Calvo, M.; Fisher, R.B. 3D technologies to acquire and visualize the human body for improving dietetic treatment. Proceedings 2019, 31, 53. [Google Scholar] [CrossRef] [Green Version]
- He, Q.; Ji, Y.; Zeng, D.; Zhang, Z. Volumeter: 3D human body parameters measurement with a single kinect. IET Comput. Vis. 2018, 12, 553–561. [Google Scholar] [CrossRef]
- Treleaven, P.; Wells, J. 3D body scanning and healthcare applications. Computer 2007. [Google Scholar] [CrossRef] [Green Version]
- Lin, J.-D.; Chiou, W.-K.; Weng, H.-F.; Tsai, Y.-H.; Liu, T.-H. Comparison of three-dimensional anthropometric body surface scanning to waist-hip ratio and body mass index in correlation with metabolic risk factors. J. Clin. Epidemiol. 2002, 55, 757–766. [Google Scholar] [CrossRef]
- Alldieck, T.; Magnor, M.A.; Xu, W.; Theobalt, C.; Pons-Moll, G. Detailed Human Avatars from Monocular Video. 2018. Available online: https://www.semanticscholar.org/paper/Detailed-Human-Avatars-from-Monocular-Video-Alldieck-Magnor/07377c375ac76a34331c660fe87ebd7f9b3d74c4. (accessed on 10 October 2018).
- Yu, T.; Zheng, Z.; Guo, K.; Zhao, J.; Dai, Q.; Li, H.; Liu, Y. Doublefusion: Real-time capture of human performances with inner body shapes from a single depth sensor. In Proceedings of the 2018 Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 18–23 June 2018. [Google Scholar] [CrossRef] [Green Version]
- Fit 3D Body Scanners. Available online: https://fit3d.com/ (accessed on 14 July 2019).
- Naked—The World’s First Home Body Scanner. Available online: https://nakedlabs.com/ (accessed on 14 July 2019).
- Villena-Martínez, V.; Fuster-Guilló, A.; Azorín-López, J.; Saval-Calvo, M.; Mora-Pascual, J.; Garcia-Rodriguez, J.; Garcia-Garcia, A. A quantitative comparison of calibration methods for RGB-D sensors using different technologies. Sensors 2017, 17, 243. [Google Scholar] [CrossRef] [Green Version]
- Hussein, M.; Nätterdal, C. The benefits of virtual reality in education—A comparision study. Bachelor’s Thesis, University of Gothenburg, Gothenburg, Sweden, 2015. [Google Scholar]
- Saval-Calvo, M.; Azorin-Lopez, J.; Fuster-Guillo, A.; Garcia-Rodriguez, J. Three-dimensional planar model estimation using multi-constraint knowledge based on k-means and RANSAC. Appl. Soft Comput. J. 2015. [Google Scholar] [CrossRef] [Green Version]
- Saval-Calvo, M.; Azorin-Lopez, J.; Fuster-Guillo, A.; Mora-Mora, H. μ-MAR: Multiplane 3D marker based registration for depth-sensing cameras. Expert Syst. 2015, 42, 9353–9365. [Google Scholar] [CrossRef] [Green Version]
- Fischler, M.A.; Bolles, R.C. Random sample consensus: A paradigm for model fitting with applications to image analysis and automated cartography. Commun. ACM 1981, 24, 381–395. [Google Scholar] [CrossRef]
- PCL Team. Point Cloud Library (PCL): pcl::MedianFilter< PointT > Class Template Reference. 2013. Available online: http://docs.ros.org/hydro/api/pcl/html/classpcl_1_1MedianFilter.html (accessed on 27 May 2019).
- PCL Team. Point Cloud Library (PCL): pcl::BilateralFilter< PointT > Class Template Reference. 2019. Available online: https://pointclouds.org/documentation/classpcl_1_1_bilateral_filter.html (accessed on 27 May 2019).
- PCL Team. Point Cloud Library (PCL): pcl::StatisticalOutlierRemoval< PointT > Class Template Reference. 2013. Available online: https://pointclouds.org/documentation/classpcl_1_1_statistical_outlier_removal_3_01pcl_1_1_p_c_l_point_cloud2_01_4.html (accessed on 27 May 2019).
- Rusu, R.B. Documentation—Point Cloud Library (PCL). Available online: http://pointclouds.org/documentation/tutorials/normal_estimation.php (accessed on 19 May 2019).
- Saval-Calvo, M.; Azorín-López, J.; Fuster-Guilló, A. Model-based multi-view registration for RGB-D sensors. Lect. Notes Comput. Sci. 2013. [Google Scholar] [CrossRef]
- Kazhdan, M.; Bolitho, M.; Hoppe, H. Poisson Surface Reconstruction. 2006. Available online: http://hhoppe.com/poissonrecon.pdf. (accessed on 28 May 2019).
- Callieri, M.; Cignoni, P.; Corsini, M.; Scopigno, R. Masked photo blending: Mapping dense photographic data set on high-resolution sampled 3D models. Comput. Graph. 2008, 32, 464–473. [Google Scholar] [CrossRef] [Green Version]
- Media—Tech4Diet: Project TIN2017-89069-R Spanish State Research Agency (AEI). 4D Modelling and Visualization of the Human Body to Improve Adherence to Dietetic-Nutritional Intervention of Obesity. 2019. Available online: http://tech4d.dtic.ua.es/media/ (accessed on 6 November 2019).
- Unity. Unity User Manual (2018.3) – Unity Manual. 2018. Available online: https://docs.unity3d.com/2018.3/Documentation/Manual/ (accessed on 27 May 2019).
- Xu, Z.; Chang, W.; Zhu, Y.; Le, D.; Zhou, H.; Zhang, Q. Building high-fidelity human body models from user-generated data. IEEE Trans. Multimed. 2020, 1. [Google Scholar] [CrossRef]
- Smith, B.M.; Chari, V.; Agrawal, A.; Rehg, J.M.; Sever, R. Towards accurate 3D human body reconstruction from silhouettes. In Proceedings of the 2019 International Conference on 3D Vision (3DV), Québec City, QC, Canada, 16–19 September 2019. [Google Scholar] [CrossRef]
- Dibra, E.; Jain, H.; Oztireli, C.; Ziegler, R.; Gross, M. HS-Nets: Estimating human body shape from silhouettes with convolutional neural networks. In Proceedings of the 2016 Fourth International Conference on 3D Vision (3DV), Stanford, CA, USA, 25–28 October 2016; pp. 108–117. [Google Scholar] [CrossRef]
- Kanazawa, A.; Black, M.J.; Jacobs, D.W.; Malik, J. End-to-End recovery of human shape and pose. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Salt Lake, UT, USA, 18–22 June 2018; pp. 7122–7131. [Google Scholar] [CrossRef] [Green Version]
- Uhm, T.; Park, H.; Park, J.I. Fully vision-based automatic human body measurement system for apparel application. Measurement 2015, 61, 169–179. [Google Scholar] [CrossRef]
- Albances, X.; Binungcal, D.; Nikko Cabula, J.; Cajayon, C.; Cabatuan, M. RGB-D camera based anthropometric measuring system for barong tagalog tailoring. In Proceedings of the 2019 IEEE 11th International Conference on Humanoid, Nanotechnology, Information Technology, Communication and Control, Environment, and Management (HNICEM), Laoag, Philippines, 29 November–1 December 2019. [Google Scholar] [CrossRef]
- Adikari, A.; Ganegoda, N.G.C.; Wanniarachchi, W. Non-Contact Human Body Parameter Measurement Based on Kinect Sensor. IOSR J. Comput. Eng. 2017, 19, 80–85. [Google Scholar] [CrossRef]
- Adikari, S.B.; Ganegoda, N.C.; Meegama, R.G.N.; Wanniarachchi, I.L. Applicability of a Single Depth Sensor in Real-Time 3D Clothes Simulation: Augmented Reality Virtual Dressing Room Using Kinect Sensor. Adv. Hum.Comput. Interact. 2020, 2020, 1314598. [Google Scholar] [CrossRef]
- Xu, H.; Li, J.; Li, J.; Lu, G. Prediction of anthropometric data based on ladder network. In Proceedings of the 2019 Chinese Automation. Congress. (CAC), Hangzhou, China, 22–24 November 2019; pp. 512–517. [Google Scholar] [CrossRef]
- Peeters, T.; Vleugels, J.; Verwulgen, S.; Danckaers, F.; Huysmans, T.; Sijbers, J.; De Bruyne, G. A comparative study between three measurement methods to predict 3D body dimensions using shape modelling. In Proceedings of the AHFE 2019 International Conference on Additive Manufacturing, Modeling Systems and 3D Prototyping, Washington, DC, USA, 24–28 July 2019. [Google Scholar]
- Gan, X.Y.; Ibrahim, H.; Ramli, D.A. A simple vision based anthropometric estimation system using webcam. J. Phys. Conf. Ser. 2020, 1529, 022067. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Object | Perimeter (1D) | Area (2D) | Volume (3D) |
|---|---|---|---|
| Cube 1 | 60.00 | 225.00 | 3375.00 |
| Cube 2 | 200.00 | 2500.00 | 125,000.00 |
| Cylinder 1 | 300.00 | 5000.00 | 196,349.54 |
| Cylinder 2 | 200.00 | 2500.00 | 98,174.77 |
| Cone | 161.80 | 1250.00 | 32,724.92 |
| Pyramid | 97.00 | 450.00 | 9000.00 |
| Object | 102 rays | Rel. ε | 103 Rays | Rel. ε | 104 Rays | Rel. ε | 105 Rays | Rel. ε |
|---|---|---|---|---|---|---|---|---|
| Cube 1 | 58.47 | 0.025500 | 59.95 | 0.000833 | 59.99 | 0.000167 | 59.93 | 0.001167 |
| Cube 2 | 194.86 | 0.025700 | 199.84 | 0.000800 | 199.99 | 0.000050 | 199.87 | 0.000650 |
| Cylinder 1 | 293.71 | 0.020967 | 299.11 | 0.002967 | 299.86 | 0.000467 | 299.44 | 0.001867 |
| Cylinder 2 | 194.72 | 0.026400 | 199.57 | 0.002150 | 199.84 | 0.000800 | 199.62 | 0.001900 |
| Cone | 157.59 | 0.026020 | 160.14 | 0.010260 | 160.49 | 0.008096 | 159.35 | 0.015142 |
| Pyramid | 93.71 | 0.033918 | 95.81 | 0.012268 | 96.00 | 0.010309 | 95.88 | 0.011546 |
| Average ε | 0.026417 | 0.004880 | 0.003315 | 0.005379 |
| Object | 102 Rays | Rel. ε | 103 Rays | Rel. ε | 104 Rays | Rel. ε | 105 Rays | Rel. ε |
|---|---|---|---|---|---|---|---|---|
| Cube 1 | 224.58 | 0.00187 | 225.01 | 0.000044 | 225.03 | 0.00013 | 225.13 | 0.000578 |
| Cube 2 | 2495.36 | 0.00186 | 2500.04 | 0.000016 | 2500.07 | 0.00003 | 2500.61 | 0.000244 |
| Cylinder 1 | 4980.81 | 0.00384 | 4992.94 | 0.001412 | 4993.92 | 0.00122 | 4990.69 | 0.001862 |
| Cylinder 2 | 2491.79 | 0.00328 | 2496.41 | 0.001436 | 2496.54 | 0.00138 | 2494.01 | 0.002396 |
| Cone | 1247.78 | 0.00178 | 1246.22 | 0.003024 | 1247.16 | 0.00227 | 1245.64 | 0.003488 |
| Pyramid | 448.45 | 0.00344 | 449.78 | 0.000489 | 450.15 | 0.00033 | 451.43 | 0.003178 |
| Average ε | 0.00268 | 0.00107 | 0.00089 | 0.00196 |
| Object | 102 Rays | Rel. ε | 103 Rays | Rel. ε | 104 Rays | Rel. ε | 105 Rays | Rel. ε |
|---|---|---|---|---|---|---|---|---|
| Cube 1 | 3368.75 | 0.00185 | 3375.07 | 0.000021 | 3375.15 | 0.00004 | 3376.2 | 0.000356 |
| Cube 2 | 124,768.49 | 0.00185 | 125,002.1 | 0.000017 | 125,006.82 | 0.00005 | 125,033.98 | 0.000272 |
| Cylinder 1 | 194,287.47 | 0.01050 | 194,832.98 | 0.007724 | 194,716.61 | 0.00832 | 195,587.54 | 0.003881 |
| Cylinder 2 | 97,385.65 | 0.00804 | 97,623.71 | 0.005613 | 97,526.31 | 0.00661 | 97,431.41 | 0.007572 |
| Cone | 32,379 | 0.01057 | 32,507.18 | 0.006654 | 32,511.76 | 0.00651 | 32,671.93 | 0.001619 |
| Pyramid | 8970.9 | 0.00323 | 9003.78 | 0.000420 | 9006.89 | 0.00077 | 9009.91 | 0.001101 |
| Average ε | 0.00601 | 0.00341 | 0.00372 | 0.00247 |
| Object | R.1D | E.1D | Rel. ε1 | R.2D | E. 2D | Rel. ε2 | R.3D | E.3D | Rel. ε3 |
|---|---|---|---|---|---|---|---|---|---|
| Cube 1 | 100 | 99.68 | 0.0032 | 625.00 | 632.09 | 0.011 | 15,625 | 15,805.6 | 0.012 |
| Body | Real. 1D | E.1D 13 Cam | E.1D 8 Cam | Abs. ε 13 Cam | Rel. ε 13 Cam | Abs. ε 8 Cam | Rel. ε 8 Cam |
|---|---|---|---|---|---|---|---|
| Calf | 32 | 32.52 | - | 0.52 | 0.016250 | - | - |
| Quadriceps | 44.50 | 44.77 | 41.71 | 0.27 | 0.006067 | 2.79 | 0.062697 |
| Waist | 74 | 75.15 | 72.88 | 1.15 | 0.015541 | 1.12 | 0.015135 |
| Hip | 84.5 | 85.20 | 84.68 | 0.70 | 0.008284 | 0.18 | 0.002130 |
| Elbow | 24.80 | 24.97 | - | 0.17 | 0.006855 | - | - |
| Wrist | 16 | 16 | - | 0.00 | 0.000000 | - | - |
| Biceps | 25.80 | 26.49 | 26.32 | 0.69 | 0.026744 | 0.52 | 0.020155 |
| Forearm | 22 | 21.58 | - | 0.42 | 0.019091 | - | - |
| Forehead | 56.70 | 56.48 | 63.21 | 0.22 | 0.003880 | 6.51 | 0.114815 |
| Neck | 34.10 | 36.48 | 35.29 | 2.38 | 0.069795 | 1.19 | 0.034897 |
| Ankle | 20.80 | 20.96 | 21.33 | 0.16 | 0.007692 | 0.53 | 0.025481 |
| Chest (low rib) | 78.50 | 78.20 | 79.01 | 0.30 | 0.003822 | 0.51 | 0.006497 |
| Shoulders | 107 | 106.59 | 110.9 | 0.41 | 0.003832 | 3.90 | 0.036449 |
| Knee | 36.40 | 31.33 | 42.07 | 5.07 | 0.139286 | 5.67 | 0.155769 |
| Hand (knuckles) | 25.40 | 27.70 | - | 2.30 | 0.090551 | - | - |
| Average ε | 0.984 | 0.027846 | 4.66 | 0.176652 |
| Estimation Method | Chest | Waist | Hip | Average |
|---|---|---|---|---|
| KPhub-I [34] | 12.92 | 23.72 | 8.43 | 15.02 |
| SMPLify [34] | 8.95 | 24.97 | 12.10 | 15.34 |
| HMR [34] | 43.39 | 16.01 | 6.15 | 21.85 |
| [35] | 12.5 | 15.8 | 9.3 | 12.53 |
| [36] | 22.8 | 24 | 20 | 22.27 |
| [37] | 92.8 | 118.3 | 68.7 | 93.27 |
| Ours | 3.0 | 11.5 | 7.0 | 7.16 |
| Estimation Method | Chest | Waist | Hip | Average |
|---|---|---|---|---|
| [38] | 1.676% | 1.52% | 1.29% | 1.49% |
| PRA [39] | 4.87% | 4.30% | 5.63% | 4.93% |
| EIR [39] | 5.02% | 4.74% | 4.57% | 4.78% |
| P2P [39] | 5.06% | 4.30% | 4.16% | 4.51% |
| [40] | 11.60% | 10.97% | N/A | 11.28% |
| [41] | 4.76% | 4.22% | 6.46% | 5.15% |
| [42] | 1.49% | 2.78% | 1.81% | 2.03% |
| Basic [43] | 4.70% | 9.01% | 1.10% | 4.93% |
| Camera [43] | 4.85% | 9.10% | 1.20% | 5.05% |
| Styku [43] | 2.50% | 6.25% | 2.40% | 3.72% |
| [44] | 2.11% | 4.66% | 4.31% | 3.69% |
| Ours | 0.38% | 1.55% | 0.82% | 0.92% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fuster-Guilló, A.; Azorín-López, J.; Saval-Calvo, M.; Castillo-Zaragoza, J.M.; Garcia-D'Urso, N.; Fisher, R.B. RGB-D-Based Framework to Acquire, Visualize and Measure the Human Body for Dietetic Treatments. Sensors 2020, 20, 3690. https://doi.org/10.3390/s20133690
Fuster-Guilló A, Azorín-López J, Saval-Calvo M, Castillo-Zaragoza JM, Garcia-D'Urso N, Fisher RB. RGB-D-Based Framework to Acquire, Visualize and Measure the Human Body for Dietetic Treatments. Sensors. 2020; 20(13):3690. https://doi.org/10.3390/s20133690
Chicago/Turabian StyleFuster-Guilló, Andrés, Jorge Azorín-López, Marcelo Saval-Calvo, Juan Miguel Castillo-Zaragoza, Nahuel Garcia-D'Urso, and Robert B. Fisher. 2020. "RGB-D-Based Framework to Acquire, Visualize and Measure the Human Body for Dietetic Treatments" Sensors 20, no. 13: 3690. https://doi.org/10.3390/s20133690