Effects of Exercise Training during Christmas on Body Weight and Cardiometabolic Health in Overweight Individuals

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
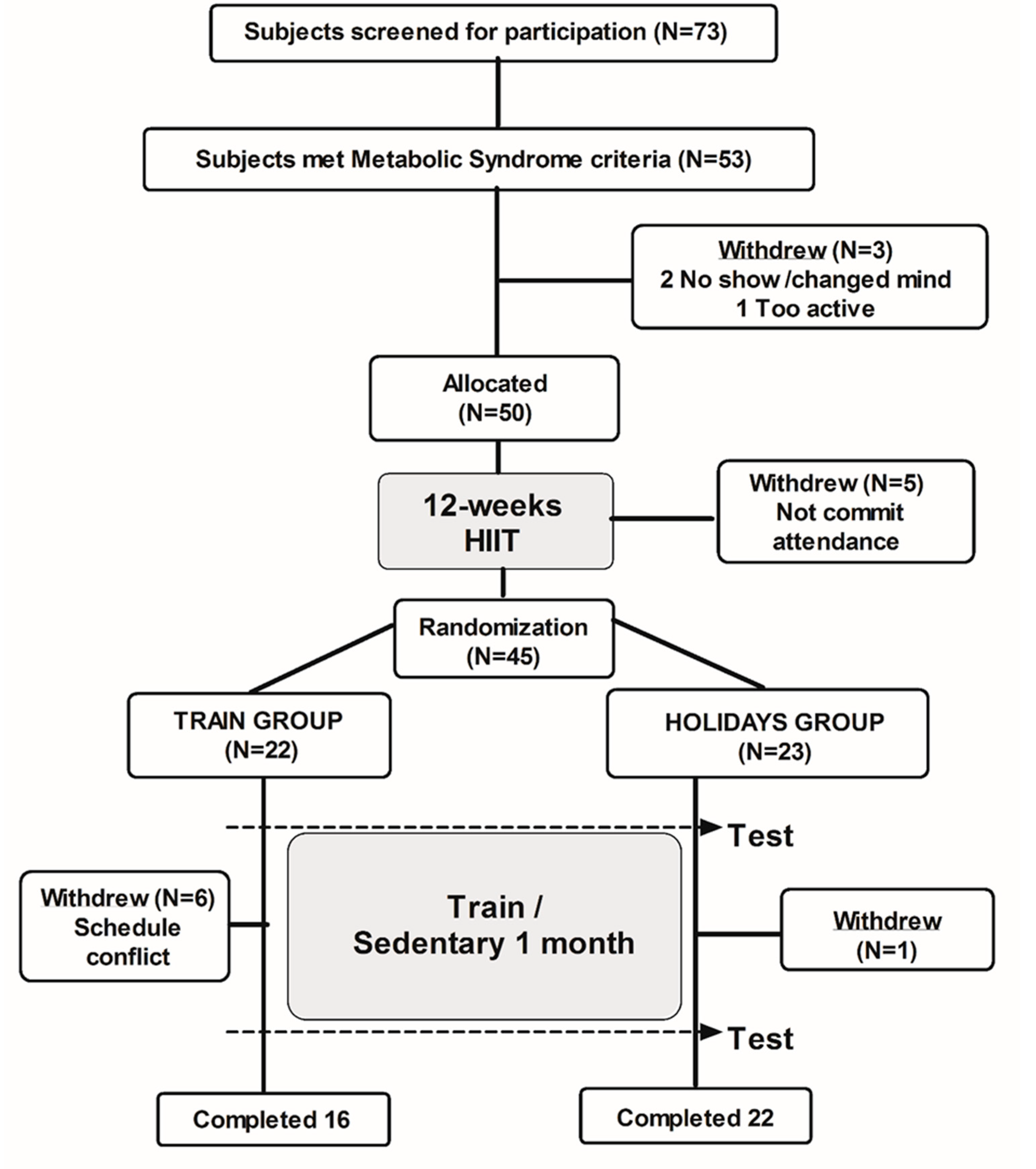
2.1. Participants
2.2. Experimental Design
2.3. Clinical Investigation
2.4. Cardio-Respiratory and Metabolic Fitness Assessment
2.5. Blood Analyses and Insulin Sensitivity
2.6. Statistical Analysis
3. Results
3.1. Caloric Intake, Physical Activity, and Mets Factors
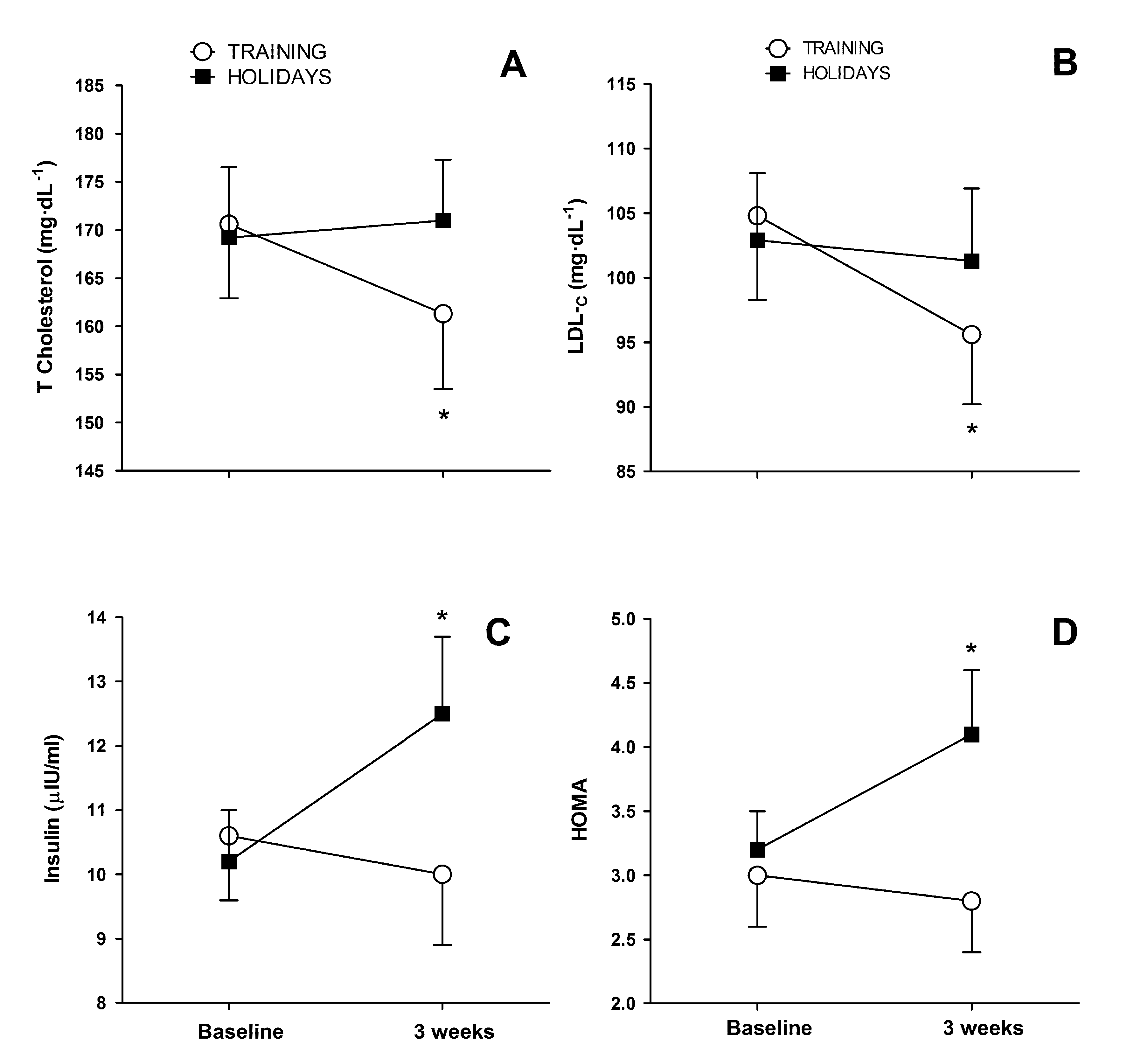
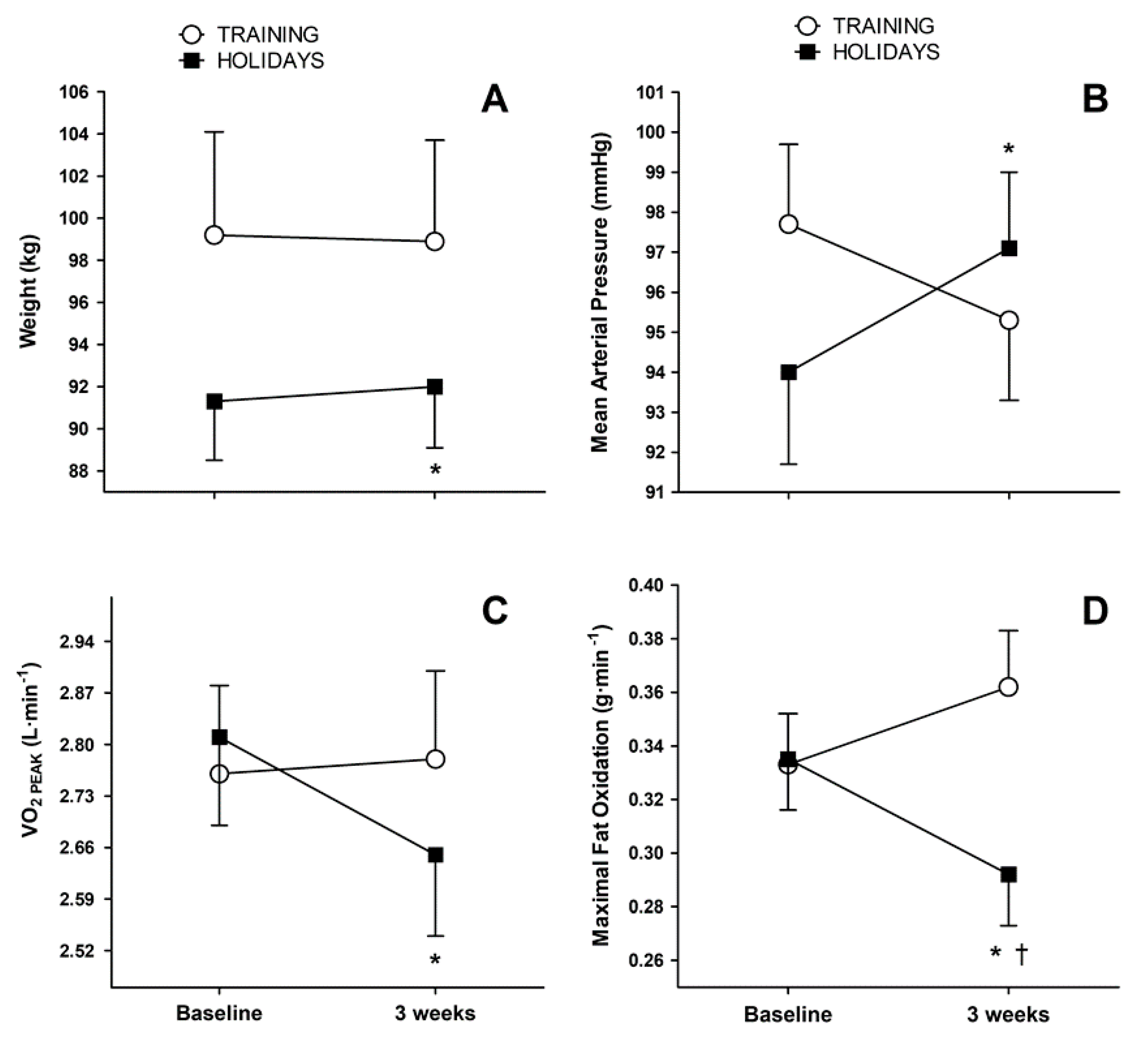
3.2. Body Composition, Carbohydrate, and Lipid Metabolism
3.3. Cardiorespiratory and Metabolic Fitness Parameters
3.4. Correlation Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mottillo, S.; Filion, K.B.; Genest, J.; Joseph, L.; Pilote, L.; Poirier, P.; Rinfret, S.; Schiffrin, E.L.; Eisenberg, M.J. The metabolic syndrome and cardiovascular risk a systematic review and meta-analysis. J. Am. Coll. Cardiol. 2010, 56, 1113–1132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C., Jr. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beltran-Sanchez, H.; Harhay, M.O.; Harhay, M.M.; McElligott, S. Prevalence and trends of metabolic syndrome in the adult U.S. population, 1999–2010. J. Am. Coll. Cardiol. 2013, 62, 697–703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palaniappan, L.; Carnethon, M.R.; Wang, Y.; Hanley, A.J.; Fortmann, S.P.; Haffner, S.M.; Wagenknecht, L. Predictors of the incident metabolic syndrome in adults: The Insulin Resistance Atherosclerosis Study. Diabetes Care 2004, 27, 788–793. [Google Scholar] [CrossRef] [Green Version]
- Van Pelt, D.W.; Newsom, S.A.; Schenk, S.; Horowitz, J.F. Relatively low endogenous fatty acid mobilization and uptake helps preserve insulin sensitivity in obese women. Int. J. Obes. 2015, 39, 149–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaesser, G.A. Exercise for prevention and treatment of cardiovascular disease, type 2 diabetes, and metabolic syndrome. Curr. Diab. Rep. 2007, 7, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Tjonna, A.E.; Lee, S.J.; Rognmo, O.; Stolen, T.O.; Bye, A.; Haram, P.M.; Loennechen, J.P.; Al-Share, Q.Y.; Skogvoll, E.; Slordahl, S.A.; et al. Aerobic interval training versus continuous moderate exercise as a treatment for the metabolic syndrome: A pilot study. Circulation 2008, 118, 346–354. [Google Scholar] [CrossRef] [Green Version]
- Johnson, J.L.; Slentz, C.A.; Houmard, J.A.; Samsa, G.P.; Duscha, B.D.; Aiken, L.B.; McCartney, J.S.; Tanner, C.J.; Kraus, W.E. Exercise training amount and intensity effects on metabolic syndrome (from Studies of a Targeted Risk Reduction Intervention through Defined Exercise). Am. J. Cardiol. 2007, 100, 1759–1766. [Google Scholar] [CrossRef] [Green Version]
- Morales-Palomo, F.; Ramirez-Jimenez, M.; Ortega, J.F.; Mora-Rodriguez, R. Effectiveness of Aerobic Exercise Programs for Health Promotion in Metabolic Syndrome. Med. Sci. Sports Exerc. 2019, 51, 1876–1883. [Google Scholar] [CrossRef]
- Ma, Y.; Olendzki, B.C.; Li, W.; Hafner, A.R.; Chiriboga, D.; Hebert, J.R.; Campbell, M.; Sarnie, M.; Ockene, I.S. Seasonal variation in food intake, physical activity, and body weight in a predominantly overweight population. Eur. J. Clin. Nutr. 2006, 60, 519–528. [Google Scholar] [CrossRef]
- O’Connell, S.E.; Griffiths, P.L.; Clemes, S.A. Seasonal variation in physical activity, sedentary behaviour and sleep in a sample of UK adults. Ann. Hum. Biol. 2014, 41, 1–8. [Google Scholar] [CrossRef]
- Yanovski, J.A.; Yanovski, S.Z.; Sovik, K.N.; Nguyen, T.T.; O’Neil, P.M.; Sebring, N.G. A prospective study of holiday weight gain. N. Engl. J. Med. 2000, 342, 861–867. [Google Scholar] [CrossRef] [Green Version]
- Helander, E.E.; Wansink, B.; Chieh, A. Weight Gain over the Holidays in Three Countries. N. Engl. J. Med. 2016, 375, 1200–1202. [Google Scholar] [CrossRef]
- Stevenson, J.L.; Krishnan, S.; Stoner, M.A.; Goktas, Z.; Cooper, J.A. Effects of exercise during the holiday season on changes in body weight, body composition and blood pressure. Eur. J. Clin. Nutr. 2013, 67, 944–949. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Craig, C.L.; Marshall, A.L.; Sjostrom, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mora-Rodriguez, R.; Ortega, J.F.; Hamouti, N.; Fernandez-Elias, V.E.; Canete Garcia-Prieto, J.; Guadalupe-Grau, A.; Saborido, A.; Martin-Garcia, M.; Guio de Prada, V.; Ara, I.; et al. Time-course effects of aerobic interval training and detraining in patients with metabolic syndrome. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 792–798. [Google Scholar] [CrossRef] [PubMed]
- Frayn, K.N. Calculation of substrate oxidation rates in vivo from gaseous exchange. J. Appl. Physiol. Respir. Environ. Exerc. Physiol. 1983, 55, 628–634. [Google Scholar] [CrossRef] [Green Version]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef]
- Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z. The metabolic syndrome. Lancet 2005, 365, 1415–1428. [Google Scholar] [CrossRef]
- Hull, H.R.; Hester, C.N.; Fields, D.A. The effect of the holiday season on body weight and composition in college students. Nutr. Metab. 2006, 3, 44. [Google Scholar] [CrossRef] [Green Version]
- Cook, C.M.; Subar, A.F.; Troiano, R.P.; Schoeller, D.A. Relation between holiday weight gain and total energy expenditure among 40- to 69-y-old men and women (OPEN study). Am. J. Clin. Nutr. 2012, 95, 726–731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mora-Rodriguez, R.; Ortega, J.F.; Morales-Palomo, F.; Ramirez-Jimenez, M. Weight loss but not gains in cardiorespiratory fitness after exercise-training predicts improved health risk factors in metabolic syndrome. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 1267–1274. [Google Scholar] [CrossRef]
- Pedersen, B.K.; Saltin, B. Exercise as medicine—Evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand. J. Med. Sci. Sports 2015, 25 (Suppl. 3), 1–72. [Google Scholar] [CrossRef] [Green Version]
- Slentz, C.A.; Houmard, J.A.; Johnson, J.L.; Bateman, L.A.; Tanner, C.J.; McCartney, J.S.; Duscha, B.D.; Kraus, W.E. Inactivity, exercise training and detraining, and plasma lipoproteins. STRRIDE: A randomized, controlled study of exercise intensity and amount. J. Appl. Physiol. 2007, 103, 432–442. [Google Scholar] [CrossRef] [Green Version]
- Kraus, W.E.; Slentz, C.A. Exercise training, lipid regulation, and insulin action: A tangled web of cause and effect. Obesity 2009, 17 (Suppl. 3), S21–S26. [Google Scholar] [CrossRef]
- Walhin, J.P.; Richardson, J.D.; Betts, J.A.; Thompson, D. Exercise counteracts the effects of short-term overfeeding and reduced physical activity independent of energy imbalance in healthy young men. J. Physiol. 2013, 591, 6231–6243. [Google Scholar] [CrossRef] [PubMed]
- Ortega, J.F.; Fernandez-Elias, V.E.; Hamouti, N.; Mora-Rodriguez, R. Increased blood cholesterol after a high saturated fat diet is prevented by aerobic exercise training. Appl. Physiol. Nutr. Metab. 2013, 38, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Mikines, K.J.; Sonne, B.; Farrell, P.A.; Tronier, B.; Galbo, H. Effect of physical exercise on sensitivity and responsiveness to insulin in humans. Am. J. Physiol. 1988, 254, E248–E259. [Google Scholar] [CrossRef] [PubMed]
- Dela, F.; Mikines, K.J.; von Linstow, M.; Secher, N.H.; Galbo, H. Effect of training on insulin-mediated glucose uptake in human muscle. Am. J. Physiol. 1992, 263, E1134–E1143. [Google Scholar] [CrossRef]
- Mora-Rodriguez, R.; Ortega, J.F.; Ramirez-Jimenez, M.; Moreno-Cabanas, A.; Morales-Palomo, F. Insulin sensitivity improvement with exercise training is mediated by body weight loss in subjects with metabolic syndrome. Diabetes Metab. 2019. [Google Scholar] [CrossRef]
- Krogh-Madsen, R.; Thyfault, J.P.; Broholm, C.; Mortensen, O.H.; Olsen, R.H.; Mounier, R.; Plomgaard, P.; van Hall, G.; Booth, F.W.; Pedersen, B.K. A 2-wk reduction of ambulatory activity attenuates peripheral insulin sensitivity. J. Appl. Physiol. 2010, 108, 1034–1040. [Google Scholar] [CrossRef] [Green Version]
- Hagobian, T.A.; Braun, B. Interactions between energy surplus and short-term exercise on glucose and insulin responses in healthy people with induced, mild insulin insensitivity. Metabolism 2006, 55, 402–408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, M.; Bhalla, V.; Patnaik, S.; Maludum, O.; Lu, M.; Figueredo, V.M. Heart failure and the holidays. Clin. Res. Cardiol. 2016, 105, 865–872. [Google Scholar] [CrossRef] [PubMed]
- Mancia, G.; Bombelli, M.; Corrao, G.; Facchetti, R.; Madotto, F.; Giannattasio, C.; Trevano, F.Q.; Grassi, G.; Zanchetti, A.; Sega, R. Metabolic syndrome in the Pressioni Arteriose Monitorate E Loro Associazioni (PAMELA) study: Daily life blood pressure, cardiac damage, and prognosis. Hypertension 2007, 49, 40–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, P.T. Increases in weight and body size increase the odds for hypertension during 7 years of follow-up. Obesity 2008, 16, 2541–2548. [Google Scholar] [CrossRef] [Green Version]
- Mora-Rodriguez, R.; Ortega, J.F.; Guio de Prada, V.; Fernandez-Elias, V.E.; Hamouti, N.; Morales-Palomo, F.; Martinez-Vizcaino, V.; Nelson, R.K. Effects of Simultaneous or Sequential Weight Loss Diet and Aerobic Interval Training on Metabolic Syndrome. Int. J. Sports Med. 2016, 37, 274–281. [Google Scholar] [CrossRef] [Green Version]
- Church, T.S.; LaMonte, M.J.; Barlow, C.E.; Blair, S.N. Cardiorespiratory fitness and body mass index as predictors of cardiovascular disease mortality among men with diabetes. Arch. Intern. Med. 2005, 165, 2114–2120. [Google Scholar] [CrossRef]
- Horowitz, J.F. Regulation of lipid mobilization and oxidation during exercise in obesity. Exerc. Sport Sci. Rev. 2001, 29, 42–46. [Google Scholar] [CrossRef]
- Morales-Palomo, F.; Ramirez-Jimenez, M.; Ortega, J.F.; Pallares, J.G.; Mora-Rodriguez, R. Cardiovascular Drift during Training for Fitness in Patients with Metabolic Syndrome. Med. Sci. Sports Exerc. 2017, 49, 518–526. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| TRAIN (n = 16) | HOLID (n = 22) | TRAIN vs. HOLID at Baseline | Time × Group | |||
|---|---|---|---|---|---|---|
| Baseline | 3 Weeks | Baseline | 3 Weeks | p Value | p Value | |
| Systolic blood pressure (mmHg) | 131.3 ± 11.6 | 128.3 ± 11.1 | 127.6 ± 14.3 | 131.3 ± 13.1 * | 0. 387 | 0.010 |
| Diastolic blood pressure (mmHg) | 80.9 ± 6.9 | 78.8 ± 7.4 | 77.2 ± 9.5 | 80.0 ± 7.8 * | 0.179 | 0.013 |
| Mean arterial pressure (mmHg) | 97.7 ± 7.9 | 95.3 ± 8.2 | 94.0 ± 10.6 | 97.1 ± 8.9 * | 0.230 | 0.010 |
| Glucose (mg·dL−1) | 111.1 ± 24.6 | 109.5 ± 19.5 | 125.0 ± 30.9 | 126.7 ± 34.3 | 0.144 | 0.546 |
| HDL-C (mg·dL−1) | 41.4 ± 8.1 | 39.9 ± 9.2 | 44.1 ± 12.4 | 45.7 ± 12.9 | 0.422 | 0.215 |
| Triglycerides (mg·dL−1) | 122.0 ± 37.1 | 128.5 ± 60.4 | 111.0 ± 39.6 | 119.8 ± 39.7 | 0.385 | 0.880 |
| Waist Circumference (cm) | 111.9 ± 11.7 | 112.2 ± 12.1 | 108.1 ± 10.3 | 110.1 ± 9.4 | 0.309 | 0.079 |
| Body weight (kg) | 99.2 ± 19.6 | 98.9 ± 19.3 | 91.3 ± 13.0 | 92.0 ± 13.4 * | 0.177 | 0.011 |
| LDL-C. | Triglycerides | Body Weight | FOMAX | VO2PEAK | |
|---|---|---|---|---|---|
| −0.096 | 0.425 * | 0.036 | −0.262 | −0.183 | HOMA |
| 0.494 * | −0.138 | 0.419 | −0.477 * | −0.290 | SBP |
| 0.032 | 0.494 * | 0.181 | −0.199 | 0.179 | Resting HR |
| −0.468 * | 0.560 * | −0.412 | −0.159 | LDL-C | |
| −0.003 | −0.106 | 0.245 | Triglycerides | ||
| −0.679 * | −0.003 | Body Weight | |||
| 0.214 | FOMAX |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramirez-Jimenez, M.; Morales-Palomo, F.; Ortega, J.F.; Moreno-Cabañas, A.; Guio de Prada, V.; Alvarez-Jimenez, L.; Mora-Rodriguez, R. Effects of Exercise Training during Christmas on Body Weight and Cardiometabolic Health in Overweight Individuals. Int. J. Environ. Res. Public Health 2020, 17, 4732. https://doi.org/10.3390/ijerph17134732
Ramirez-Jimenez M, Morales-Palomo F, Ortega JF, Moreno-Cabañas A, Guio de Prada V, Alvarez-Jimenez L, Mora-Rodriguez R. Effects of Exercise Training during Christmas on Body Weight and Cardiometabolic Health in Overweight Individuals. International Journal of Environmental Research and Public Health. 2020; 17(13):4732. https://doi.org/10.3390/ijerph17134732
Chicago/Turabian StyleRamirez-Jimenez, Miguel, Felix Morales-Palomo, Juan Fernando Ortega, Alfonso Moreno-Cabañas, Valle Guio de Prada, Laura Alvarez-Jimenez, and Ricardo Mora-Rodriguez. 2020. "Effects of Exercise Training during Christmas on Body Weight and Cardiometabolic Health in Overweight Individuals" International Journal of Environmental Research and Public Health 17, no. 13: 4732. https://doi.org/10.3390/ijerph17134732