Mothers and Fathers Parenting Stress and Their Perception of Children’s Psychosocial Functioning in Paediatric Diabetes: A Pilot Study

 , ,
, ,
Abstract
:1. Introduction
- the child’s HbA1c would significantly correlate with both mothers’ and fathers’ parenting stress and their perception of the child’s psychosocial symptoms [6];
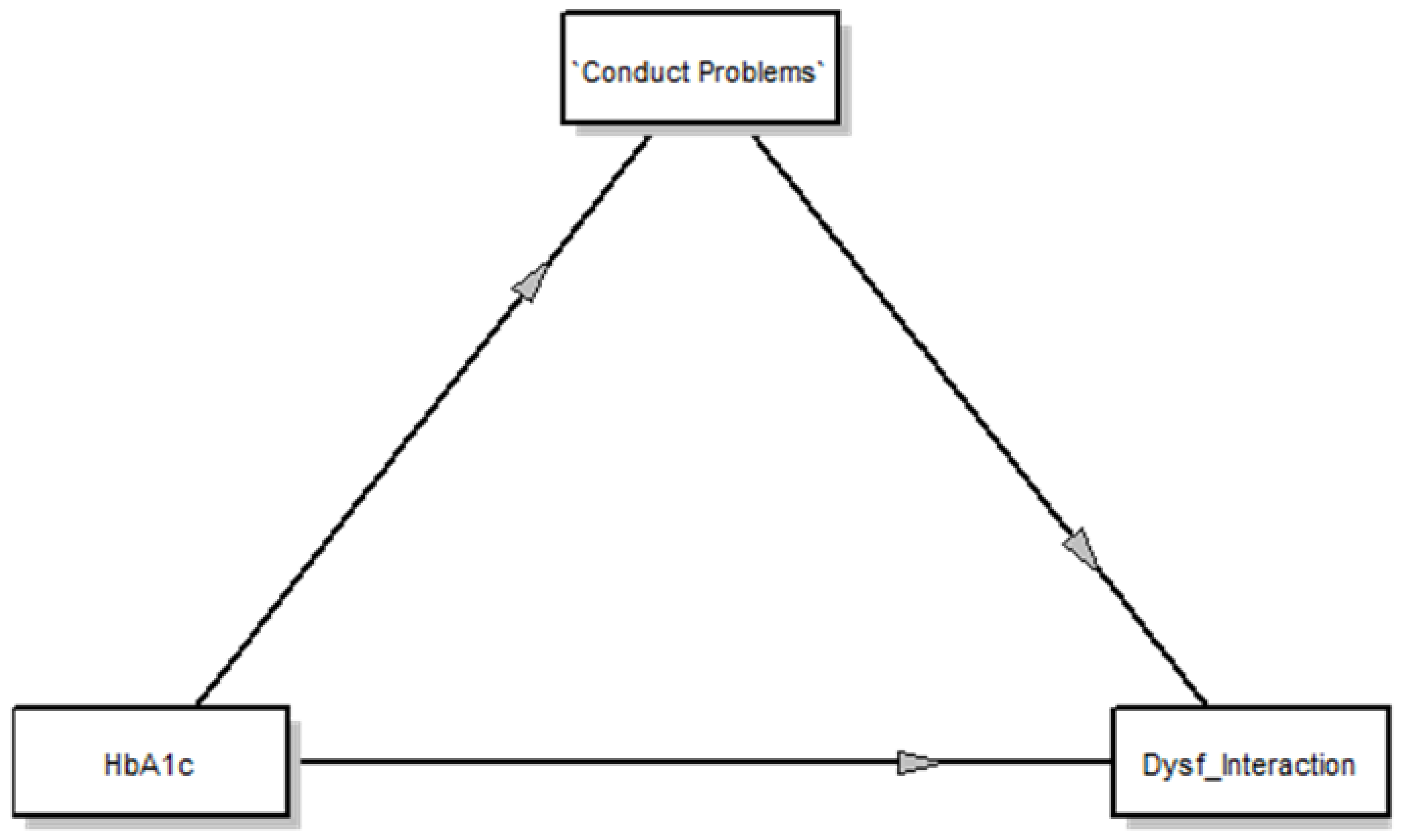
- a relationship between HbA1c and mothers’ and fathers’ parenting stress, mediated by perception of their child’s emotional and behavioral problems. It was assumed that poor glycemic control would be associated with a higher level of parenting stress, mediated by their association with the increased perception of the child’s emotional and behavioral problems in both parents [8,9,10,11,13].
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Measures
2.3.1. The Strengths and Difficulties Questionnaire–Parents
2.3.2. Parenting Stress Index-Fourth Edition-Short Form
2.4. Statistical Analysis
3. Results
3.1. T-Test For Paired-Samples in Parental Couples
3.2. Partial Correlations in Parental Couples
3.3. Mediation Models
3.3.1. Fathers
3.3.2. Mothers
4. Discussion
Limitations and Future Implications
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- International Diabetes Federation. Available online: https://www.idf.org/e-library/epidemiology-research/diabetes-atlas/19-atlas-6th-edition.html (accessed on 1 March 2020).
- Bianchi, C.; Rossi, E.; Miccoli, R. Epidemiologia del diabete. In Il Diabete in Italia, 1st ed.; Bonora, E., Sesti, G., Eds.; Bononia University Press: Bologna, Italy, 2016; pp. 13–20. [Google Scholar]
- Boogered, E.A.; Noordam, C.; Verhaak, C.M. The Sugarsquare study: Protocol of a multicenter randomized controlled trial concerning a web-based patient portal for parents of a child with type 1 diabetes. BMC Pediatr. 2014, 14, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iversen, A.S.; Graue, M.; Haugstvedt, A.; Råheim, M. Being mothers and fathers of a child with type 1 diabetes aged 1 to 7 years: A phenomenological study of parents’ experiences. Int. J. Qual. Stud. Health Well Being 2018, 13, 1487758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maas-van Schaaijk, N.M.; Odink, R.J.; Ultee, K.; van Baar, A.L. Can one question be a useful indicator of psychosocial problems in adolescents with diabetes mellitus? Acta Paediatr. 2011, 100, 708–711. [Google Scholar] [CrossRef] [PubMed]
- Whittemore, R.; Jaser, S.S.; Chao, A.; Jang, M.; Grey, M. Psychological Experience of Parents of Children with Type 1 Diabetes: A Systematic Mixed-Studies Review. Diabetes Educ. 2012, 38, 562–579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reynolds, K.A.; Helgeson, V.S. Children with Diabetes Compared to Peers: Depressed? Distressed? A Meta-Analytic Review. Ann. Behav. Med. 2011, 42, 29–41. [Google Scholar] [CrossRef] [Green Version]
- Limbers, C.A.; Teasdale, A. Parenting Stress in Fathers of Children with Type 1 Diabetes. Fam. Community Health 2018, 41, 117–122. [Google Scholar] [CrossRef]
- Viaene, A.S.; Van Daele, T.; Bleys, D.; Faust, K.; Massa, G.G. Fear of Hypoglycemia, Parenting Stress, and Metabolic Control for Children with Type 1 Diabetes and Their Parents. J. Clin. Psychol. Med. Settings 2017, 24, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Sweenie, R.; Mackey, E.R.; Streisand, R. Parent-Child Relationships in Type 1 Diabetes: Associations among Child Behavior, Parenting Behavior, and Pediatric Parenting Stress. Fam. Syst. Health 2013, 32, 31–42. [Google Scholar] [CrossRef] [Green Version]
- Streisand, R.; Swift, E.; Wickmark, T.; Holmes, C.S. Pediatric Parenting Stress among Parents of Children with Type 1 Diabetes: The Role of Self-Efficacy, Responsibility, and Fear. J. Pediatr. Psychol. 2005, 30, 513–521. [Google Scholar] [CrossRef]
- Aldubayee, M.; Mohamud, S.; Almadani, K.A.; Alabbad, A.A.; Alotabi, A.G.; Alkodair, A.A.; Babiker, A. Parental levels of stress managing a child diagnosed with type 1 diabetes in Riyadh: A cross-sectional study. BMC Psychiatry 2020, 20, 2–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaser, S.S.; Whittemore, R.; Ambrosino, J.M.; Lindemann, E.; Grey, M. Mediators of depressive symptoms in children with type 1 diabetes and their Mothers. J. Pediatr. Psychol. 2008, 33, 509–519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eckshtain, D.; Ellis, D.A.; Kolmodin, K.; Naar-King, S. The effects of parental Depression and parenting practices on depressive symptoms and metabolic control in urban youth with insulin-dependent. J. Pediatr. Psychol. 2010, 35, 426–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maas-van Schaaijk, N.M.; Roeleveld, A.; van BaarAnneloes, A. The Interrelationships among Paternal and Maternal Parenting Stress, Metabolic Control, and Depressive Symptoms in Adolescents with Type 1 Diabetes Mellitus. J. Pediatr. Psychol. 2013, 38, 30–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cousino, M.; Hazan, R. Parenting stress among caregivers of children with chronic illness: A systematic review. J. Pediatr. Psychol. 2013, 1, 3–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hilliard, M.E.; Monaghan, M.; Cogen, F.R.; Streisand, R. Parent stress and child behavior among young children with type 1 diabetes. Child Care Health Dev. 2011, 37, 224–232. [Google Scholar] [CrossRef]
- Van Gampelaere, C.; Luyckx, K.; Straaten, S.; Laridaen, J.; Goethals, E.R.; Casteels, K.; Goubert, L. Families with pediatric type 1 diabetes: A comparison with the general population on child well-being, parental distress and parenting behavior. Pediatr. Diabetes 2019, 21, 395–408. [Google Scholar] [CrossRef]
- Phares, V.; Lopez, E.; Fields, S.; Kamboukos, D.; Duhig, A.M. Are Fathers Involved in Pediatric Psychology Research and Treatment? J. Pediatr. Psychol. 2005, 30, 631–643. [Google Scholar] [CrossRef]
- Dashiff, C.; Vance, D.; Abdullatif, H.; Wallander, J. Parenting, autonomy and self-care of adolescents with Type 1 diabetes. Child Care Health Dev. 2009, 35, 79–88. [Google Scholar] [CrossRef] [Green Version]
- De Los Reyes, A.; Augenstein, T.M.; Wang, M.; Thomas, S.A.; Drabick, D.A.G.; Burgers, D.E.; Rabinowitz, J. The validity of the multi-informant approach to assessing child and adolescent mental health. Psychol. Bull. 2015, 141, 858–900. [Google Scholar] [CrossRef]
- Streisand, R.; Mackey, E.R.; Elliot, B.M.; Mednick, L.; Slaughter, I.M.; Turek, J.; Austin, A. Parental anxiety and depression associated with caring for a child newly diagnosed with type 1 diabetes: Opportunities for education and counseling. Patient Educ. Couns. 2008, 73, 333–338. [Google Scholar] [CrossRef]
- Rumburg, T.M.; Lord, J.H.; Savin, K.L.; Jaser, S.S. Maternal diabetes distress is linked to maternal depressive symptoms and adolescents’ glycemic control. Pediatr. Diabetes 2017, 18, 67–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Gampelaere, C.; Vervoort, T.; Luyckx, K.; De Paepe, A.; Van Aken, S.; Goubert, L. Maternal distress in the context of their child’s type 1 diabetes: Exploring the role of adaptive maternal emotion regulation on child outcomes. Psychol. Health Med. 2018, 23, 337–346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hannonen, R.; Aunola, K.; Eklund, K.; Ahonen, T. Maternal Parenting Style and Glycemic Control in Children with Type 1 Diabetes. Int. J. Environ. Res. Public Health 2019, 16, 214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiebe, D.J.; Gelfand, D.; Butler, J.M.; Korbel, C.; Fortnberry, K.T.; McCabe, J.E.; Berg, C.A. Longitudinal Associations of Maternal Depressive Symptoms, Maternal Involvement, and Diabetes Management Across Adolescence. J. Pediatr. Psychol. 2011, 36, 837–846. [Google Scholar] [CrossRef] [Green Version]
- Lewis, A.B.; Storch, E.A.; Silverstein, J.H.; Baumeister, A.L.; Strawser, M.S.; Geffken, G.R. Validation of the Pediatric Inventory for Parents in Mothers of Children with Type 1 Diabetes: An Examination of ParentingStress, Anxiety, and Childhood Psychopathology. Fam. Syst. Health 2005, 23, 56–65. [Google Scholar] [CrossRef]
- Hood, K.K.; Peterson, C.M.; Rohan, J.M.; Drotar, D. Association between adherence and glycemic control in pediatric type 1 diabetes: A meta-analysis. Pediatrics 2009, 124, e1171–e1179. [Google Scholar] [CrossRef]
- Mullins, P.; Sharplin, P.; Yki-Jarvinen, H.; Riddle, M.C.; Haring, H.U. Negative binomial meta-regression analysis of combined glycosylated hemoglobin and hypoglycemia outcomes across eleven Phase III and IV studies of insulin glargine compared with neutral protamine Hagedorn insulin in type 1 and type 2 diabetes mellitus. Clin. Ther. 2007, 29, 1607–1619. [Google Scholar] [CrossRef]
- Khandan, M.; Abazari, F.; Tirgari, B.; Cheraghi, M.A. Lived Experiences of Mothers with Diabetic Children from the Transfer of Caring Role. IJCBNM 2018, 6, 76–88. [Google Scholar]
- Mitchell, S.J. Stress among fathers of young children with type 1 diabetes. Fam. Syst. Health 2009, 27, 314–324. [Google Scholar] [CrossRef] [Green Version]
- Hansen, A.; Weissebrod, C.; Schwarts, D.D.; Taylor, W.P. Paternal Involvement in Pediatric Type 1 Diabetes: Fathers’ and Mothers’ Psychological Functioning and Disease Management. Fam. Syst. Health 2012, 30, 47–59. [Google Scholar] [CrossRef]
- Al-Khurinej, A. Emotional and Behavioral Problems among Diabetic Children. Dig. Middle East Stud. 2007, 16, 1–11. [Google Scholar] [CrossRef]
- Zenlea, I.S.; Mednick, L.; Rein, J.; Quinn, M.; Wolfsdorf, J.; Rhodes, E.T. Routine behavioral and mental health screening in young children with type 1 diabetes mellitus. Pediatr. Diabetes 2014, 15, 384–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kristensen, L.J.; Birkebaek, N.H.; Mose, A.H.; Hohwü, L.; Thastum, M. Symptoms of emotional, behavioral, and social difficulties in the danish population of children and adolescents with type 1 diabetes—Results of a national survey. PLoS ONE 2014, 9, e97543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eilander, M.M.A.; Snoek, F.J.; Rotteveel, J.; Aanstoot, H.J.; Bakker-van Waarde, W.M.; Houdijk, E.C.A.M.; de Wit, M. Parental Diabetes Behaviors and Distress Are Related to Glycemic Control in Youth with Type 1 Diabetes: Longitudinal Data from the DINO Study. Diabetes Res. Clin. Pract. 2017, 2017, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Goodman, R. The strengths and difficulties questionnaire: A research note. J. Child Psychol. Psychiatry 1997, 38, 581–586. [Google Scholar] [CrossRef]
- Tobia, V.; Marzocchi, G.M. The strengths and difficulties questionnaire-parents for Italian school-aged children: Psychometric properties and norms. Child Psychiatry Hum. Dev. 2018, 49, 1–8. [Google Scholar] [CrossRef]
- Abidin, R.R. Parenting Stress Index, 4th ed.; Lutz, F.L., Ed.; PAR: Lutz, FL, USA, 2012. [Google Scholar]
- Guarino, A.; Laghi, F.; Serantoni, G.; Di Blasio, P.; Camisasca, E. Parenting Stress Index, 4th ed.; (PSI-4); Richard, R.A., Giunti O.S., Eds.; IRIS PubliCatt: Firenze, Italy, 2016; pp. 1–134. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Academic Press: New York, NY, USA, 1988. [Google Scholar]
- Preacher, K.J.; Hayes, A.F. Asymptotic and Resampling Strategies for Assessing and Comparing Indirect Effects in Multiple Mediator Models. Behav. Res. Methods 2008, 40, 879–891. [Google Scholar] [CrossRef]
- Hayes, A.F. Beyond Baron and Kenny: Statistical Mediation Analysis in the New Millennium. Commun. Monogr. 2009, 76, 408–420. [Google Scholar] [CrossRef]
- Levy, A.J.; Landerman, L.R.; Davis, L.L. Advances in Mediation Analysis Can Facilitate Nursing Research. Nurs. Res. 2011, 60, 333–339. [Google Scholar] [CrossRef] [Green Version]
- IBM Corp. IBM SPSS Statistics for Windows; Version 24.0; IBM Corp.: Armonk, NY, USA, 2016. [Google Scholar]
- Marigliano, M.; Tadiotto, A.; Morandi, A.; Sabbion, A.; Contreas, G.; Avossa, F.; Fedeli, U.; Maffeis, C. Epidemiology of type 1 diabetes mellitus in the pediatric population in Veneto Region, Italy. Diabetes Res. Clin. Pract. 2015, 9, e20–e21. [Google Scholar] [CrossRef]
- Ferrito, L.; Predieri, B.; Pjetraj, D.; Alessandrelli, M.C.; Pagnini, M.; Iannilli, A.; Marino, M.; Tobolini, S.; Pintaudi, B.; Lucisano, G.; et al. Weekend-Based Parent-Group Intervention to Reduce Sress in Parents of Children and Adolescents with Type 1 Diabetes: A Pilot Study. J. Diabetes Res. 2019, 1, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Bekker, C.I.; Deacon, E.; Segal, D. Meaning in life experienced by parents of children living with diabetes. Health Psychol. Open 2019, 6, 1–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reinard, J.C. Communication Research Statistics; SAGE: London, UK, 2006; pp. 1–582. [Google Scholar] [CrossRef]


{kind=link}
| Paired T-Test | Mother Mean (SD) | Father Mean (SD) | Mean Difference (SD) | Z | Sig. (2 Tailed) |
|---|---|---|---|---|---|
| PSI_Total Stress Scale | 71.08 (13.58) | 64.75 (14.57) | 6.33 (14.84) | −1.38 | 0.17 |
| PSI_Parental Distress | 26.83 (6.28) | 22.42 (4.87) | 4.42 (7.95) | −1.74 | 0.08 |
| PSI_Parent–Child Dysfunctional Interaction | 19.17 (4.45) | 18.00 (3.93) | 1.17 (5.47) | −.64 | 0.53 |
| PSI_Difficult Child | 25.08 (7.27) | 24.50 (7.71) | 0.58 (4.52) | −1.13 | 0.89 |
| SDQ_Internalizing Symptoms | 3.42 (3.43) | 2.83 (2.79) | 0.58 (0.90) | −1.93 | 0.04 |
| SDQ_Externalizing Symptoms | 5.67 (3.17) | 5.33 (2.71) | 0.33 (2.02) | −1.20 | 0.23 |
| SDQ_Total Score | 9.08 (6.36) | 8.17 (5.31) | 0.92 (2.19) | 0.13 | |
| SDQ_Emotional Symptoms | 2.17 (2.13) | 1.92 (1.78) | 0.25 (0.87) | −1.00 | 0.34 |
| SDQ_Conduct Problems | 2.08 (1.78) | 2.00 (1.78) | 0.08 (0.80) | −0.38 | 0.71 |
| Mothers | HbA1c (mg/dL) | SDQ-P_Total Score | SDQ-P_ Internalizing | SDQ-P_ Externalizing | SDQ-P_Emotional Symptoms | SDQ-P_Conduct Problems | PSI_Total Stress | PSI_Parental Distress | PSI_Parent–Child Dysfunctional Interaction |
|---|---|---|---|---|---|---|---|---|---|
| SDQ-P_Total Score | 0.85 *** | 1.00 | |||||||
| SDQ-P_Internalizing | 0.82 *** | 0.98 *** | 1.00 | ||||||
| SDQ-P_Externalizing | 0.85 *** | 0.98 *** | 0.92 *** | 1.00 | |||||
| SDQ-P_Emotional Symptoms | 0.84 *** | 0.78 ** | 0.80 | 0.73 | 1.00 | ||||
| SDQ-P_Conduct Problems | 0.93 *** | 0.89 *** | 0.83 *** | 0.92 *** | 0.84 *** | 1.00 | |||
| PSI_Total Stress | 0.47 | 0.48 | 0.56 | 0.38 | 0.53 | 0.49 | 1.00 | ||
| PSI_Parental Distress | −0.21 | −0.14 | −0.04 | −0.24 | 0.00 | −0.10 | 0.65 ** | 1.00 | |
| PSI_Parent–Child Dysfunctional Interaction | 0.68 ** | 0.74 ** | 0.83 *** | 0.61 | 0.68 * | 0.62 | 0.82 *** | 0.24 | 1.00 |
| PSI_Difficult Child | 0.69 ** | 0.60 | 0.60 | 0.57 | 0.61 | 0.75 ** | 0.85 *** | 0.22 | 0.72 * |
| Fathers | HbA1c (mg/dL) | SDQ-P_Total Score | SDQ-P_ Internalizing | SDQ-P_ Externalizing | SDQ-P_Emotional Symptoms | SDQ-P_Conduct Problems | PSI_Total Stress | PSI_Parental Distress | PSI_Parent–Child Dysfunctional Interaction |
|---|---|---|---|---|---|---|---|---|---|
| SDQ-P_Total Score | 0.78 ** | 1.00 | |||||||
| SDQ-P_Internalizing | 0.70 ** | 0.98 *** | 1.00 | ||||||
| SDQ-P_Externalizing | 0.84 *** | 0.98 *** | 0.93 *** | 1.00 | |||||
| SDQ-P_Emotional Symptoms | 0.73 ** | 0.87 *** | 0.84 *** | 0.78 ** | 1.00 | ||||
| SDQ-P_Conduct Problems | 0.90 *** | 0.81 *** | 0.75 ** | 0.84 *** | 0.73 ** | 1.00 | |||
| PSI_Total Stress | 0.88 *** | 0.65 ** | 0.61 | 0.67 ** | 0.60 | 0.79 ** | 1.00 | ||
| PSI_Parental Distress | 0.72 ** | 0.55 | 0.48 | 0.60 | 0.37 | 0.73 ** | 0.85 *** | 1.00 | |
| PSI_Parent–Child Dysfunctional Interaction | 0.58 | 0.21 | 0.13 | 0.29 | 0.21 * | 0.27 | 0.66 ** | 0.35 | 1.00 |
| PSI_Difficult Child | 0.86 *** | 0.73 ** | 0.72 ** | 0.71 ** | 0.74 ** | 0.85 *** | 0.95 *** | 0.75 ** | 0.47 * |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Riso, D.; Bassi, G.; Mancinelli, E.; Zaffani, S.; Salcuni, S.; Maffeis, C. Mothers and Fathers Parenting Stress and Their Perception of Children’s Psychosocial Functioning in Paediatric Diabetes: A Pilot Study. Int. J. Environ. Res. Public Health 2020, 17, 4734. https://doi.org/10.3390/ijerph17134734
Di Riso D, Bassi G, Mancinelli E, Zaffani S, Salcuni S, Maffeis C. Mothers and Fathers Parenting Stress and Their Perception of Children’s Psychosocial Functioning in Paediatric Diabetes: A Pilot Study. International Journal of Environmental Research and Public Health. 2020; 17(13):4734. https://doi.org/10.3390/ijerph17134734
Chicago/Turabian StyleDi Riso, Daniela, Giulia Bassi, Elisa Mancinelli, Silvana Zaffani, Silvia Salcuni, and Claudio Maffeis. 2020. "Mothers and Fathers Parenting Stress and Their Perception of Children’s Psychosocial Functioning in Paediatric Diabetes: A Pilot Study" International Journal of Environmental Research and Public Health 17, no. 13: 4734. https://doi.org/10.3390/ijerph17134734