
Abstract
Background
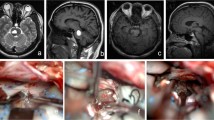
Removal of a pontine cavernous malformation requires sufficient exposure since any restriction on surgical freedom may lead to suboptimal visualization of the lesion, injury to the brainstem, and neurological catastrophe.
Methods
We describe and demonstrate the subtemporal transtentorial approach to a cavernous malformation of the upper pons, with emphasis on adequate surgical exposure while avoiding the need for extensive bone removal of the skull base.
Conclusions
The meticulous technique is paramount to the successful removal of any brainstem cavernous malformation. Along with the surgical exposure, delicate handling of the malformation is demonstrated in the accompanying operative video.





Similar content being viewed by others


Abbreviations
- DVA:
-
Developmental venous anomaly
- MRI:
-
Magnetic resonance imaging
References
Cavalcanti DD, Preul MC, Kalani MYS, Spetzler RF (2016) Microsurgical anatomy of safe entry zones to the brainstem. J Neurosurg 124(5):1359–1376
Dammann P, Wrede K, Jabbarli R, Müller O, Mönninghoff C, Frosting M, Sure U (2017) Of bubbles and layers: which cerebral cavernous malformation are most difficult to dissect from surrounding eloquent brain tissue? Neurosurgery 81(3):498–503
Jacobs R, Kano H, Gross BA, Niranjan A, Monaco EA III, Lunsford LD (2019) Defining long-term clinical outcome and risks of stereotactic radiosurgery for brainstem cavernous malformations. World Neurosurg 124:e58–e64
Kearns KN, Chen CJ, Tvrdik P, Park MS, Kalani MYS (2019) Outcomes of surgery for brainstem cavernous malformations: a systematic review. Stroke 50:2964–2966
Li D, Hao SY, Jia GJ, Wu Z, Zhang LW, Zhang JT (2014) Hemorrhage risks and functional outcomes of untreated brainstem cavernous malformations. J Neurosurg 121:32–41
Porter RW, Detwiler PW, Spetzler RF, Lawton MT, Baskin JJ, Derksen PT, Zabramski JM (1999) Cavernous malformations of the brainstem: experience with 100 patients. Neurosurgery 90(1):50–58
Sanchez Correa TE, Gallardo Ceja D, Mendez Rosito D (2019) Subtemporal approach for the resection of a midbrain cavernous malformation: evaluation of safe surgical corridors. Neurosurg Focus 1(1):v1
Sandalcioglu IE, Widemayer H, Secer S, Asgari S, Stolke D (2002) Surgical removal of brain stem cavernous malformations: surgical indications, technical considerations, and results. J Neurol Neurosurg Psychiatry 72:351–355
Xie MG, Li D, Guo FZ, Zhang LW, Zhang JT, Wu Z, Meng GL, Xiao XR (2018) Brainstem cavernous malformations: surgical indications based on natural history and surgical outcome. World Neurosurg 110:55–63
Yokoyama K, Kawanishi M, Sugie A, Yamada M, Tanaka H, Ito Y, Yamshita M (2019) Microsurgical resection of a ventral pontine cavernoma via supratrigeminal zone by anterior transpetrosal approach: 2-dimensional operative video. Oper Neurosurg 16(3):396
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Consent statement
The patient has consented to the submission of this How I Do It to the Acta Neurochirurgica.
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Summary of key points
1. The subtemporal transtentorial approach accesses the middle incisural space and lateral pons.
2. This operation is suitable for any hemorrhagic cavernous malformation involving the lateral upper pons, as annual re-hemorrhage can be as high as 8% and can lead to significant neurological deficits.
3. An anterior petrosectomy at Kawase’s region may not be necessary unless more anteroinferior exposure is needed.
4. Head position should take advantage of gravity for assistance in the mobilization of the temporal lobe. A lumbar drain can be helpful if the patient’s neck is too stiff for downward lateral flexion.
5. For sufficient exposure, the tentorial incision must be extended to the middle incisural space, but the trochlear nerve and superior cerebellar artery must be carefully preserved near the completion of that incision.
6. A developmental venous anomaly accompanies the brainstem cavernous malformation almost uniformly. Surgical exposure must be adequate to control this while leaving it unharmed to preserve brainstem drainage.
7. Bipolar cautery should be used sparingly and only at a very low setting.
8. Neurophysiological function of the brainstem should be monitored throughout the operation.
9. Nearly all the sensory fibers of the body travel through the upper lateral pons along with cerebellar connections involved in coordination. Expectation should be properly managed, as postoperative numbness and gait problems are quite common.
10. Recovery of sensory and coordination functions, and normalization of the MRI, can occur quickly.
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Vascular Neurosurgery - Arteriovenous malformation
Electronic supplementary material
Rights and permissions
About this article

Cite this article
Jean, W.C., Davis, G.L. How I do it: Subtemporal transtentorial approach for cavernous malformation of the pons. Acta Neurochir 163, 1751–1756 (2021). https://doi.org/10.1007/s00701-020-04457-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-020-04457-9