Analysis of Chest-Compression Depth and Full Recoil in Two Infant Chest-Compression Techniques Performed by a Single Rescuer: Systematic Review and Meta-Analysis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Search Strategy
2.3. Eligibility Criteria
2.4. Risk of Bias in Individual Studies
2.5. Data Extraction
2.6. Statistical Analysis
3. Results
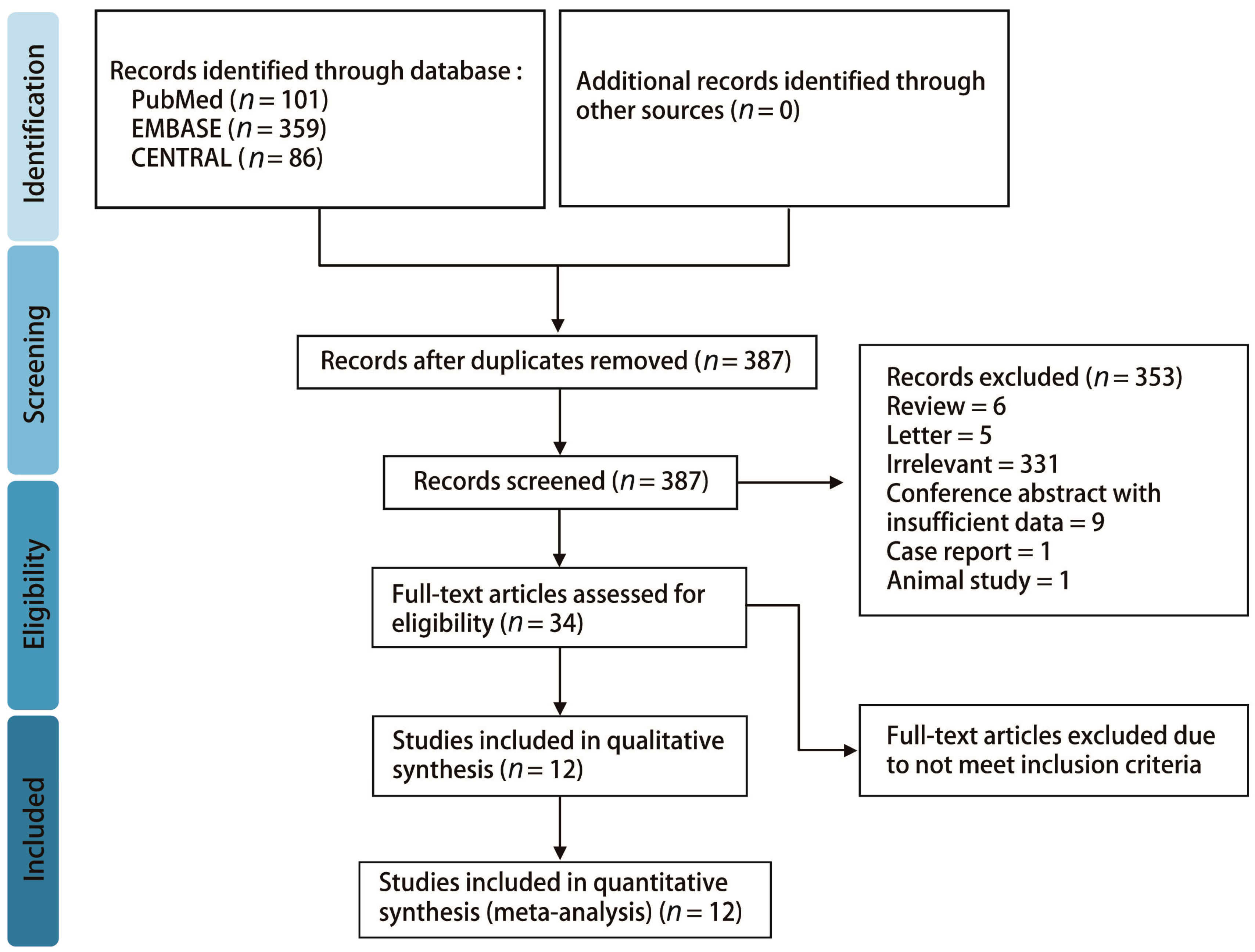
3.1. Study Identification and Selection
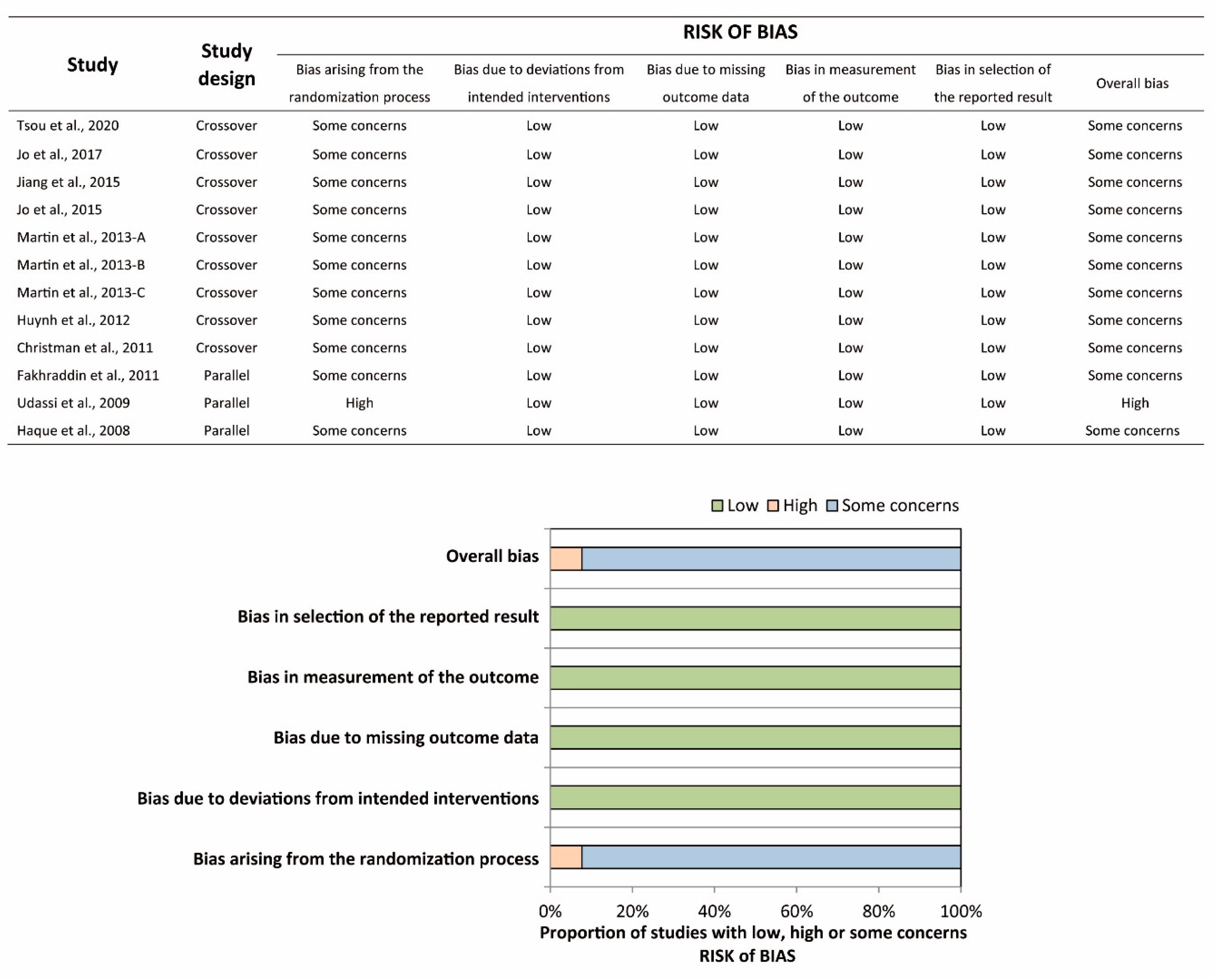
3.2. Study Characteristics and Quality, and Risk of Bias Assessment
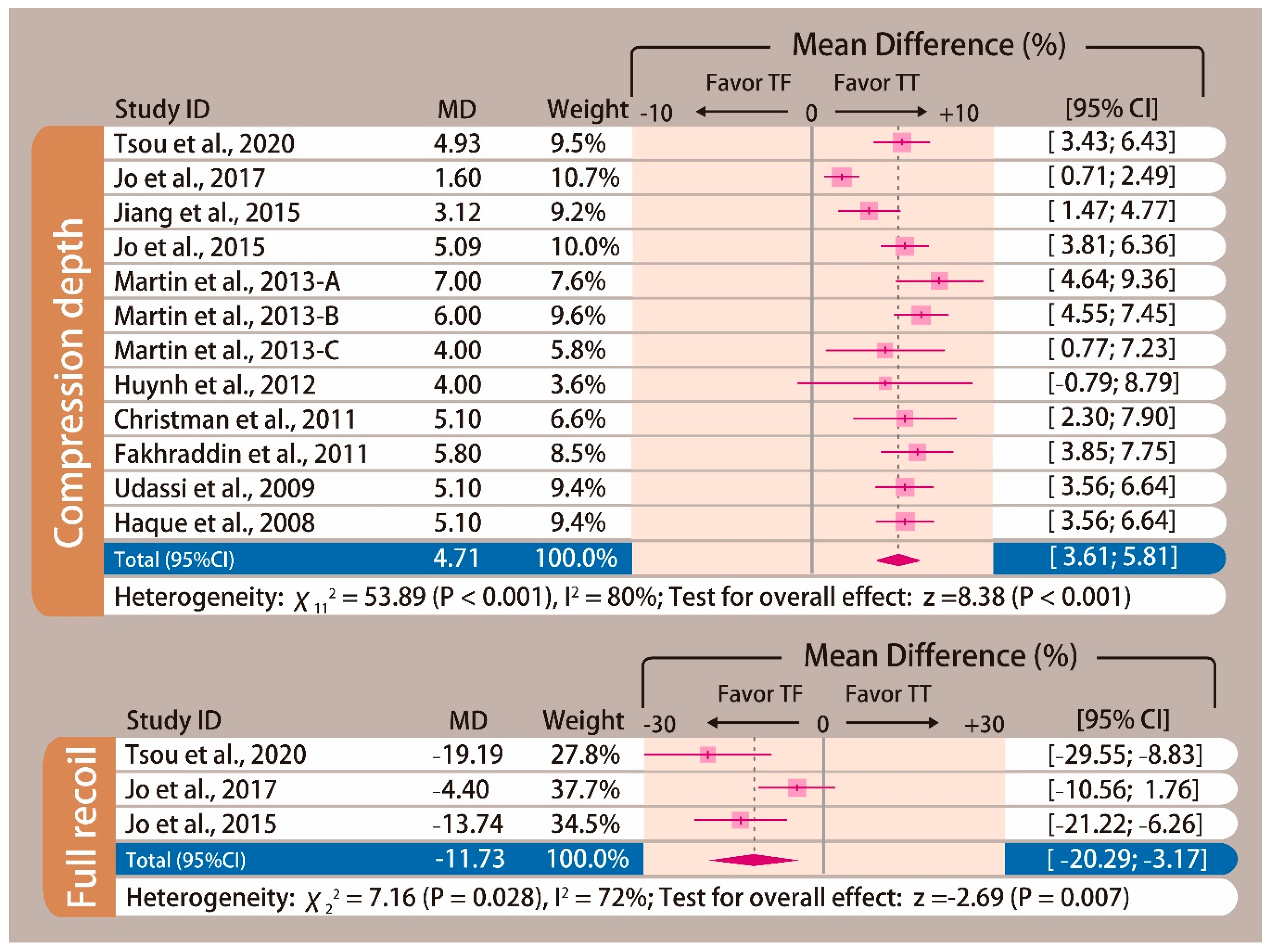
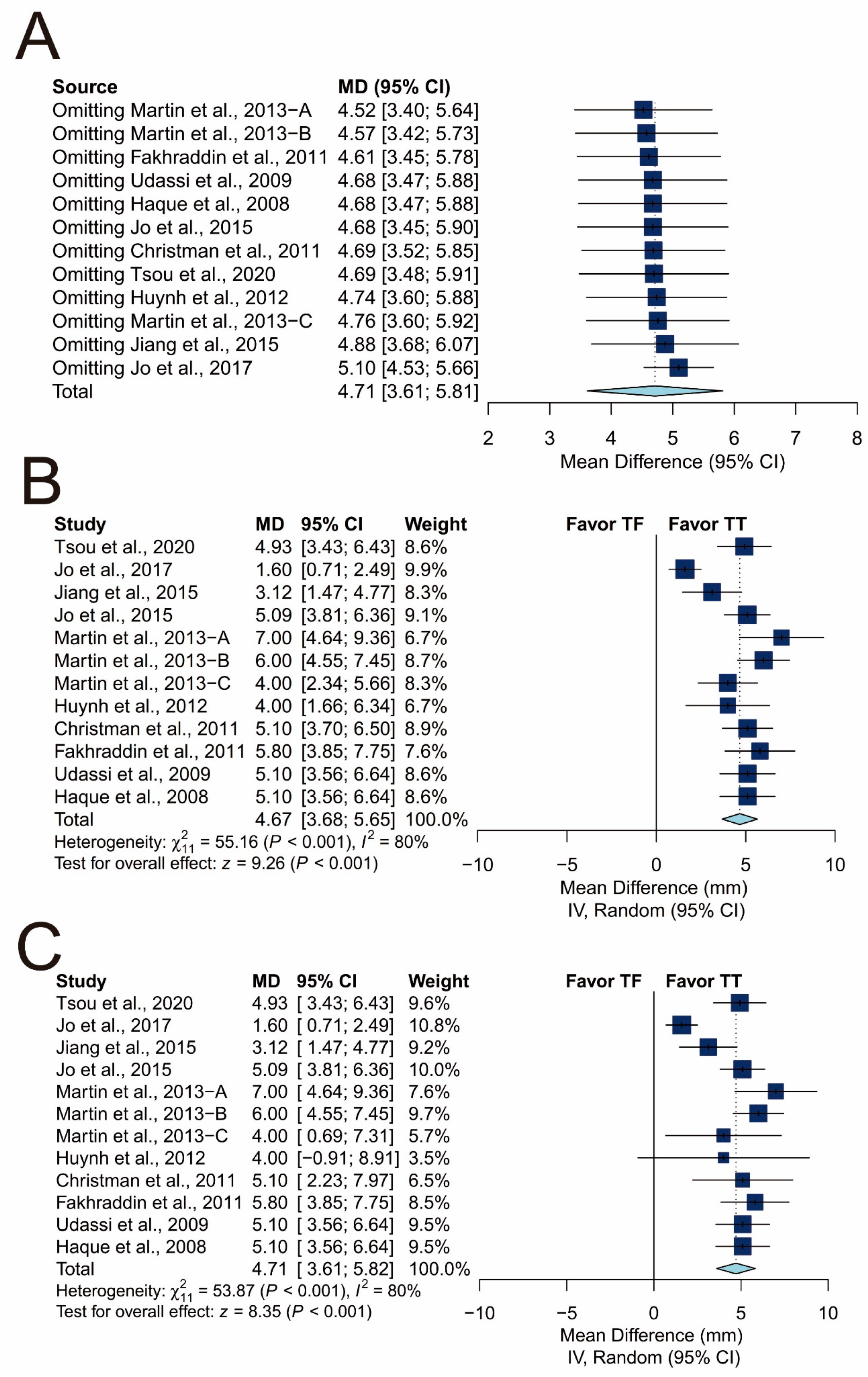
3.3. Overall Summary Measurement
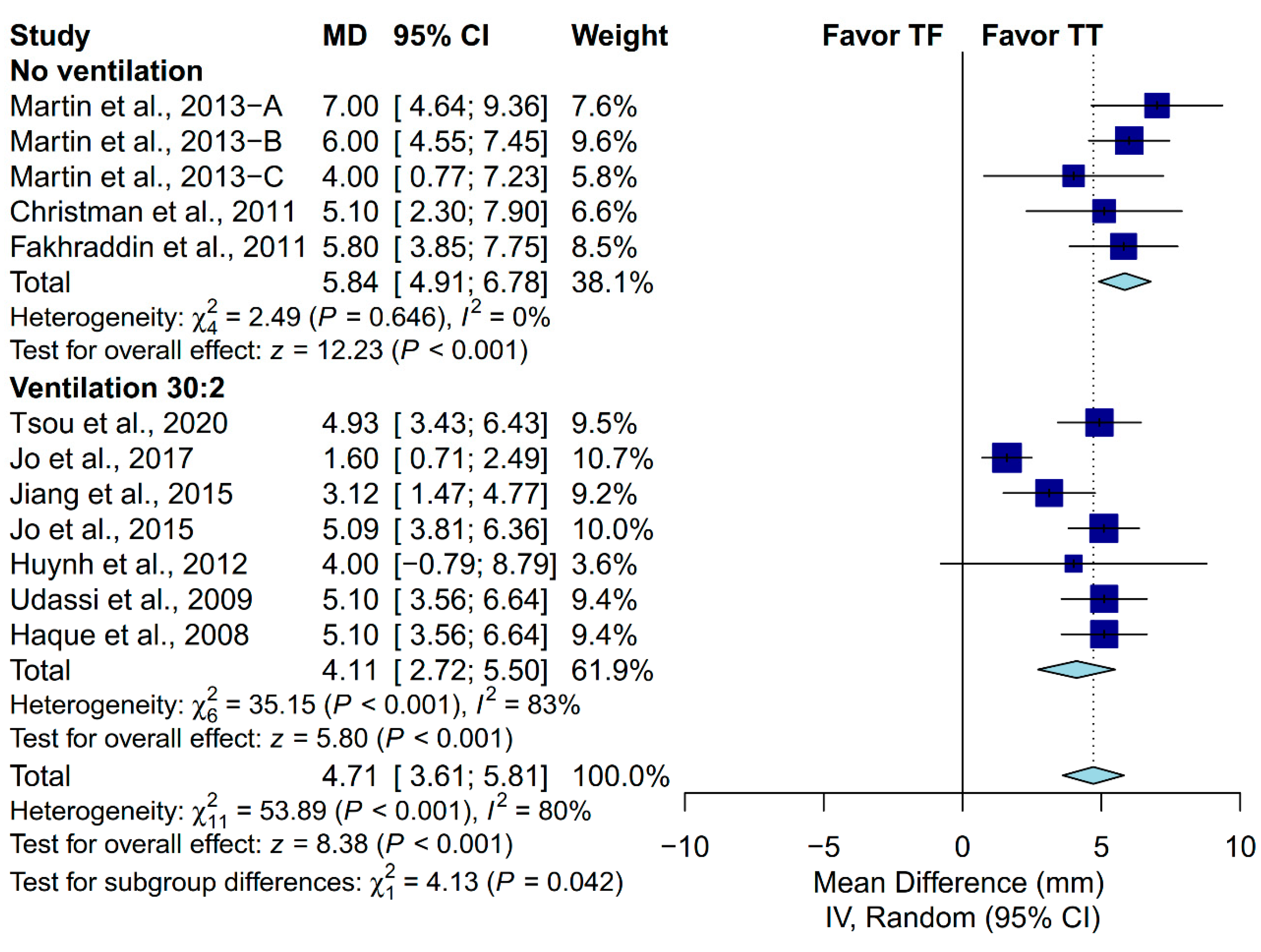
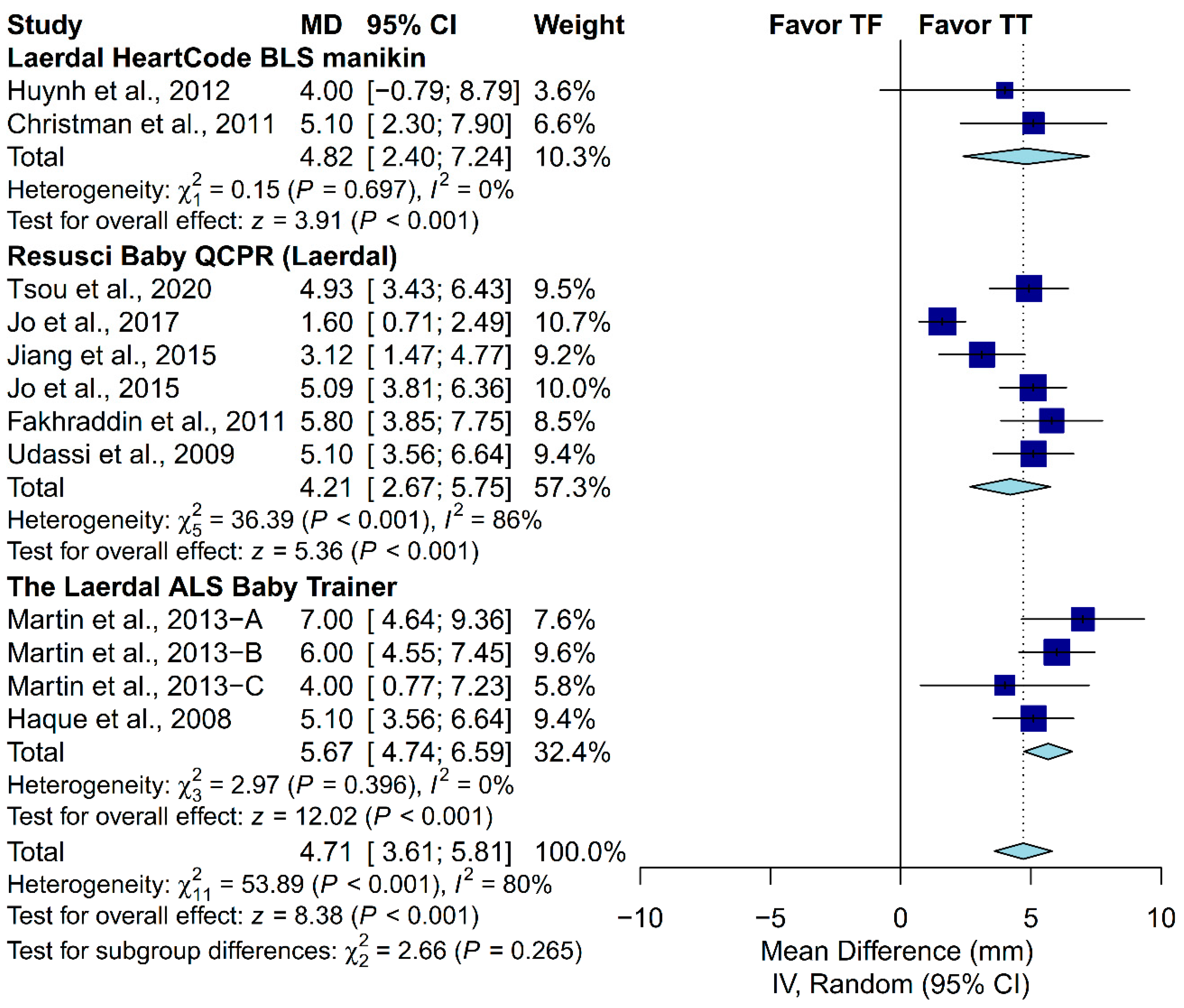
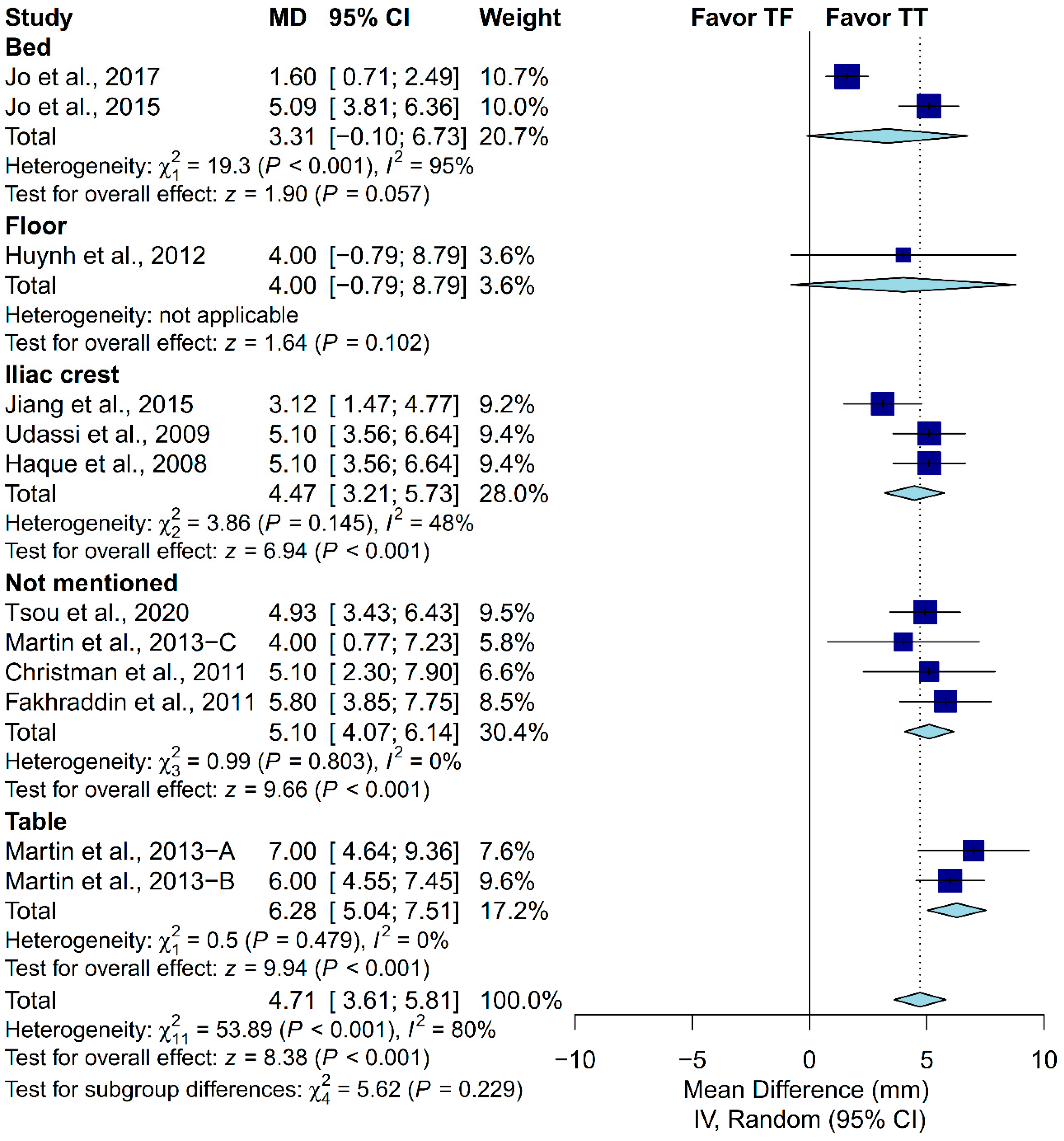
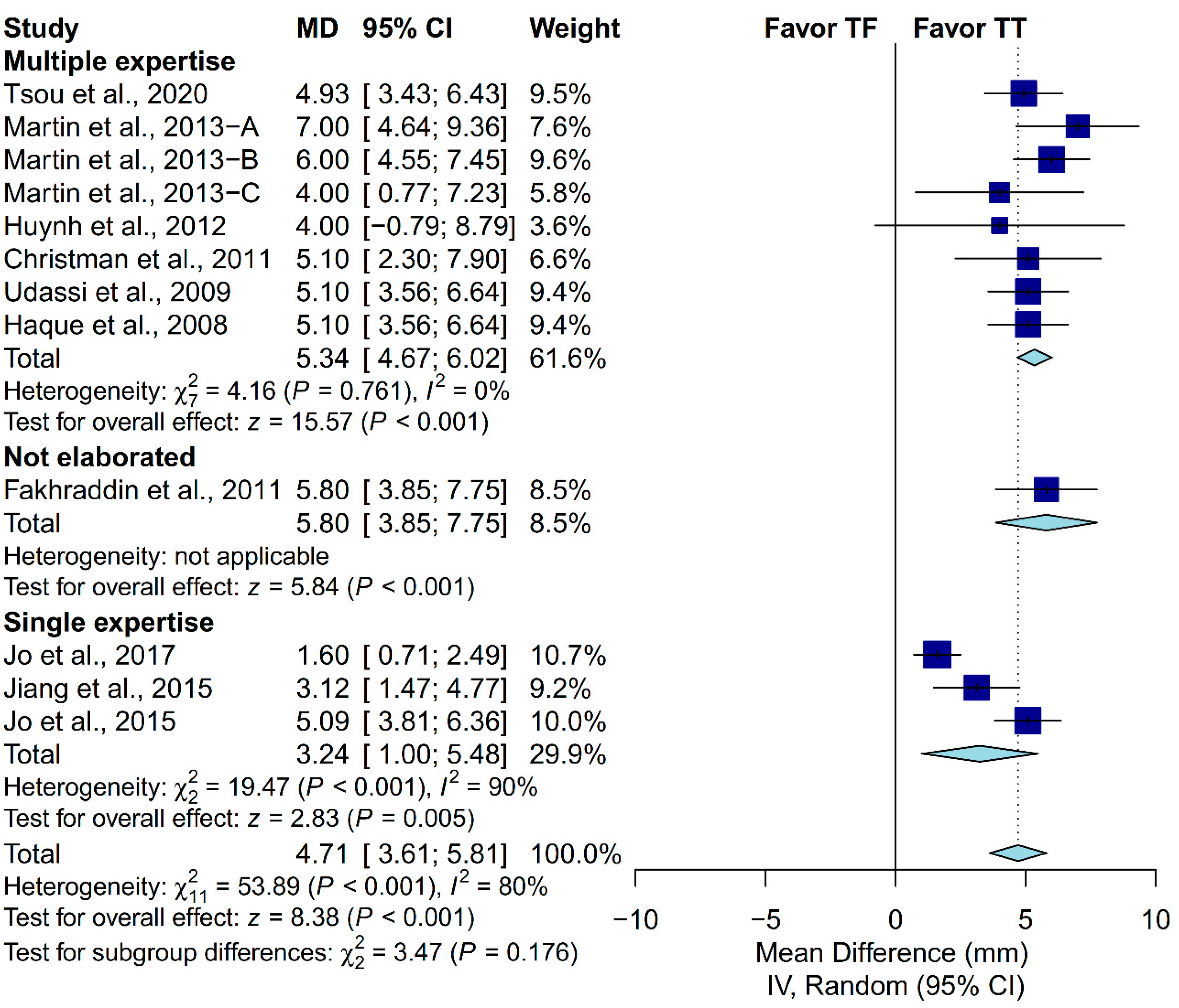
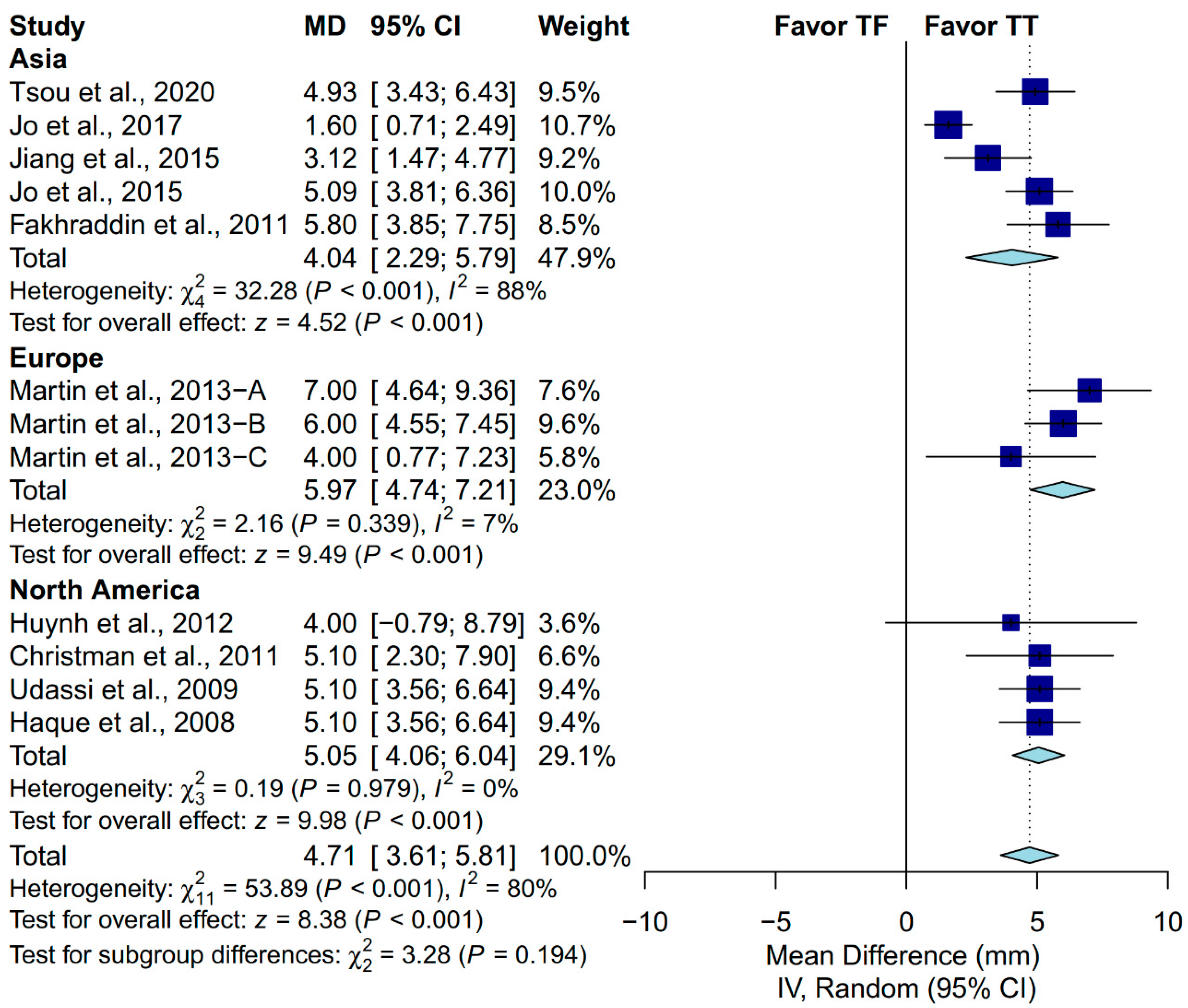
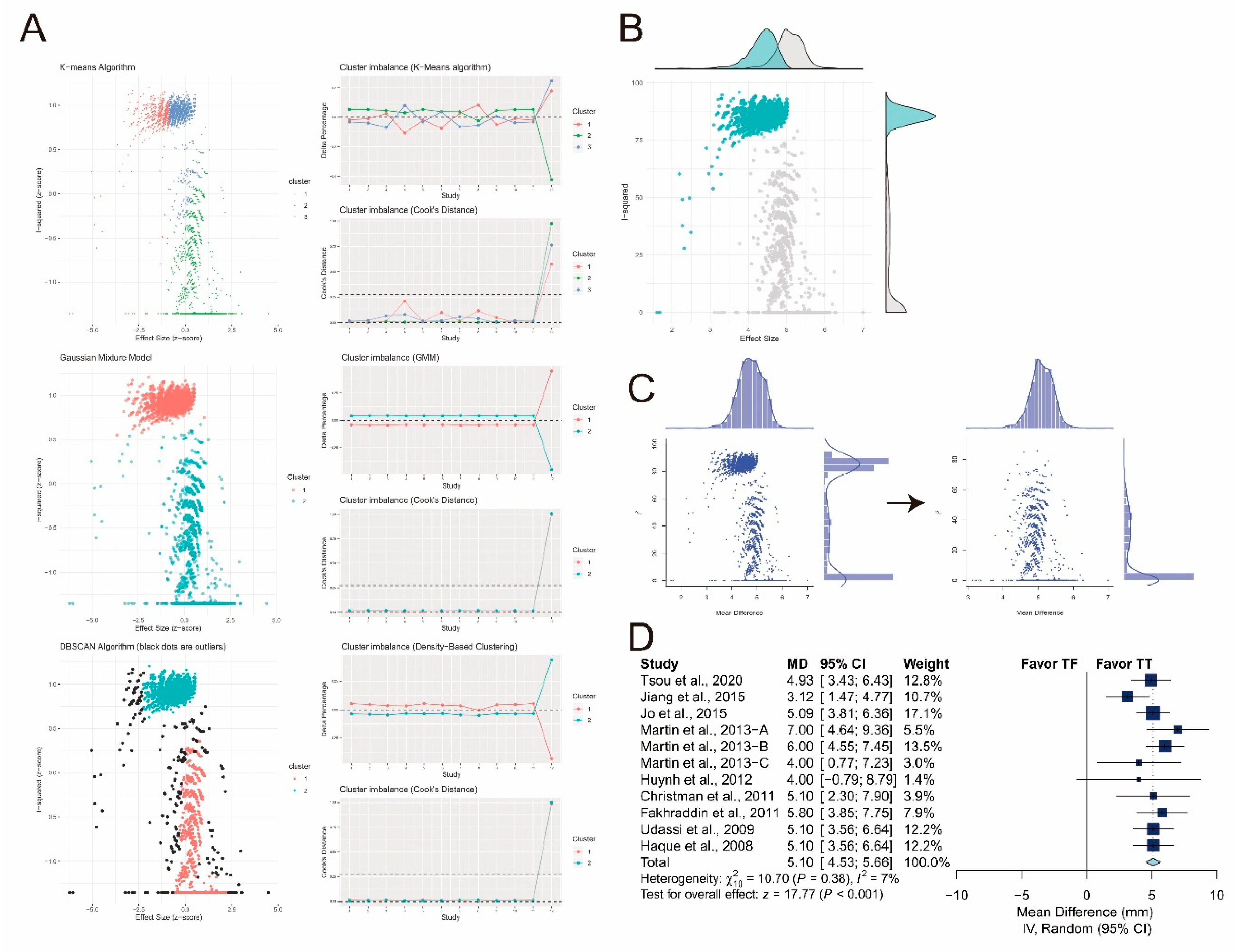
3.4. Subgroup Analysis in Chest-Compression Depth
3.5. Sensitivity Analysis in Chest-Compression Depth
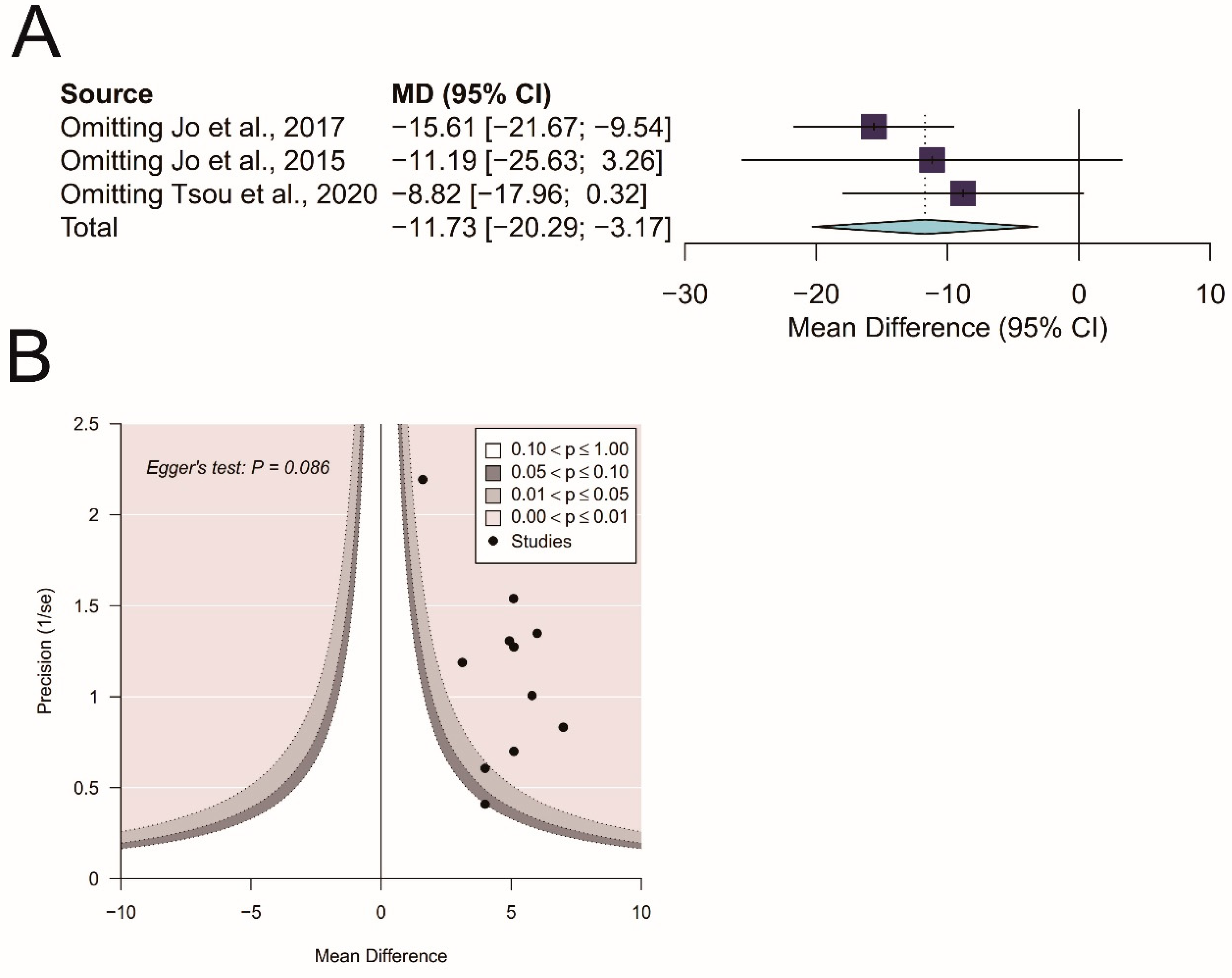
3.6. Influence Analysis in Complete Chest Recoil
3.7. Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Atkins, D.L.; Everson-Stewart, S.; Sears, G.K.; Daya, M.; Osmond, M.H.; Warden, C.R.; Berg, R.A.; Resuscitation Outcomes Consortium, I. Epidemiology and outcomes from out-of-hospital cardiac arrest in children: The Resuscitation Outcomes Consortium Epistry-Cardiac Arrest. Circulation 2009, 119, 1484–1491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, K.D.; Gausche-Hill, M.; McClung, C.D.; Lewis, R.J. A prospective, population-based study of the epidemiology and outcome of out-of-hospital pediatric cardiopulmonary arrest. Pediatrics 2004, 114, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Tress, E.E.; Kochanek, P.M.; Saladino, R.A.; Manole, M.D. Cardiac arrest in children. J. Emerg. Trauma Shock 2010, 3, 267–272. [Google Scholar] [CrossRef] [PubMed]
- Atkins, D.L.; Berger, S.; Duff, J.P.; Gonzales, J.C.; Hunt, E.A.; Joyner, B.L.; Meaney, P.A.; Niles, D.E.; Samson, R.A.; Schexnayder, S.M. Part 11: Pediatric Basic Life Support and Cardiopulmonary Resuscitation Quality: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2015, 132, S519–S525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Caen, A.R.; Maconochie, I.K.; Aickin, R.; Atkins, D.L.; Biarent, D.; Guerguerian, A.M.; Kleinman, M.E.; Kloeck, D.A.; Meaney, P.A.; Nadkarni, V.M.; et al. Part 6: Pediatric Basic Life Support and Pediatric Advanced Life Support: 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation 2015, 132, S177–S203. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Savovic, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Elbourne, D.R.; Altman, D.G.; Higgins, J.P.; Curtin, F.; Worthington, H.V.; Vail, A. Meta-analyses involving cross-over trials: Methodological issues. Int. J. Epidemiol. 2002, 31, 140–149. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Olkin, I.; Dahabreh, I.J.; Trikalinos, T.A. GOSH—A graphical display of study heterogeneity. Res. Synth Methods 2012, 3, 214–223. [Google Scholar] [CrossRef]
- Hartigan, J.A.; Wong, M.A. Algorithm AS 136: A K-Means Clustering Algorithm. J. R Stat. Soc. Ser. C Appl. Stat. 1979, 28, 100–108. [Google Scholar] [CrossRef]
- Schubert, E.; Sander, J.; Ester, M.; Kriegel, H.P.; Xu, X. DBSCAN Revisited, Revisited: Why and How You Should (Still) Use DBSCAN. ACM T Database Syst. 2017, 42, 1–21. [Google Scholar] [CrossRef]
- Leisch, F. FlexMix: A General Framework for Finite Mixture Models and Latent Class Regression in R. J. Stat. Softw. 2004, 11, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; Version 6.0; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]
- Peters, J.L.; Sutton, A.J.; Jones, D.R.; Abrams, K.R.; Rushton, L. Contour-enhanced meta-analysis funnel plots help distinguish publication bias from other causes of asymmetry. J. Clin. Epidemiol. 2008, 61, 991–996. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Borenstein, M.; Hedges, L.; Higgins, J.; Rothstein, H. Comprehensive Meta-Analysis Version 3; Biostat: Englewood, NJ, USA, 2013. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019; Available online: https://www.R-project.org/ (accessed on 16 December 2019).
- Lee, S.Y.; Hong, J.Y.; Oh, J.H.; Son, S.H. The superiority of the two-thumb over the two-finger technique for single-rescuer infant cardiopulmonary resuscitation. Eur. J. Emerg. Med. 2018, 25, 372–376. [Google Scholar] [CrossRef]
- Haque, I.U.; Udassi, J.P.; Udassi, S.; Theriaque, D.W.; Shuster, J.J.; Zaritsky, A.L. Chest compression quality and rescuer fatigue with increased compression to ventilation ratio during single rescuer pediatric CPR. Resuscitation 2008, 79, 82–89. [Google Scholar] [CrossRef]
- Jo, C.H.; Cho, G.C.; Lee, C.H. Two-Thumb Encircling Technique Over the Head of Patients in the Setting of Lone Rescuer Infant CPR Occurred During Ambulance Transfer: A Crossover Simulation Study. Pediatric Emerg. Care 2017, 33, 462–466. [Google Scholar] [CrossRef]
- Jo, C.H.; Jung, H.S.; Cho, G.C.; Oh, Y.J. Over-the-head two-thumb encircling technique as an alternative to the two-finger technique in the in-hospital infant cardiac arrest setting: A randomised crossover simulation study. Emerg. Med. J. 2015, 32, 703–707. [Google Scholar] [CrossRef]
- Jiang, J.; Zou, Y.; Shi, W.; Zhu, Y.; Tao, R.; Jiang, Y.; Lu, Y.; Tong, J. Two-thumb-encircling hands technique is more advisable than 2-finger technique when lone rescuer performs cardiopulmonary resuscitation on infant manikin. Am. J. Emerg. Med. 2015, 33, 531–534. [Google Scholar] [CrossRef] [PubMed]
- Tsou, J.Y.; Kao, C.L.; Chang, C.J.; Tu, Y.F.; Su, F.C.; Chi, C.H. Biomechanics of two-thumb versus two-finger chest compression for cardiopulmonary resuscitation in an infant manikin model. Eur. J. Emerg. Med. 2020, 27, 132–136. [Google Scholar] [CrossRef] [PubMed]
- Martin, P.S.; Kemp, A.M.; Theobald, P.S.; Maguire, S.A.; Jones, M.D. Do chest compressions during simulated infant CPR comply with international recommendations? Arch. Dis. Child. 2013, 98, 576–581. [Google Scholar] [CrossRef] [PubMed]
- Martin, P.S.; Kemp, A.M.; Theobald, P.S.; Maguire, S.A.; Jones, M.D. Does a more “physiological” infant manikin design effect chest compression quality and create a potential for thoracic over-compression during simulated infant CPR? Resuscitation 2013, 84, 666–671. [Google Scholar] [CrossRef] [PubMed]
- Martin, P.; Theobald, P.; Kemp, A.; Maguire, S.; Maconochie, I.; Jones, M. Real-time feedback can improve infant manikin cardiopulmonary resuscitation by up to 79%—A randomised controlled trial. Resuscitation 2013, 84, 1125–1130. [Google Scholar] [CrossRef]
- Huynh, T.K.; Hemway, R.J.; Perlman, J.M. The two-thumb technique using an elevated surface is preferable for teaching infant cardiopulmonary resuscitation. J. Pediatric 2012, 161, 658–661. [Google Scholar] [CrossRef]
- Christman, C.; Hemway, R.J.; Wyckoff, M.H.; Perlman, J.M. The two-thumb is superior to the two-finger method for administering chest compressions in a manikin model of neonatal resuscitation. Arch. Dis. Child. Fetal Neonatal Ed. 2011, 96, F99–F101. [Google Scholar] [CrossRef] [PubMed]
- Fakhraddin, B.Z.; Shimizu, N.; Kurosawa, S.; Sakai, H.; Miyasaka, K.; Mizutani, S. New method of chest compression for infants in a single rescuer situation: Thumb-index finger technique. J. Med. Dent. Sci. 2011, 58, 15–22. [Google Scholar]
- Udassi, J.P.; Udassi, S.; Theriaque, D.W.; Shuster, J.J.; Zaritsky, A.L.; Haque, I.U. Effect of alternative chest compression techniques in infant and child on rescuer performance. Pediatric Crit. Care Med. 2009, 10, 328–333. [Google Scholar] [CrossRef]
- David, R. Closed chest cardiac massage in the newborn infant. Pediatrics 1988, 81, 552–554. [Google Scholar] [CrossRef] [PubMed]
- Whitelaw, C.C.; Slywka, B.; Goldsmith, L.J. Comparison of a two-finger versus two-thumb method for chest compressions by healthcare providers in an infant mechanical model. Resuscitation 2000, 43, 213–216. [Google Scholar] [CrossRef]
- Dorfsman, M.L.; Menegazzi, J.J.; Wadas, R.J.; Auble, T.E. Two-thumb vs. two-finger chest compression in an infant model of prolonged cardiopulmonary resuscitation. Acad Emerg. Med. 2000, 7, 1077–1082. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Houri, P.K.; Frank, L.R.; Menegazzi, J.J.; Taylor, R. A randomized, controlled trial of two-thumb vs two-finger chest compression in a swine infant model of cardiac arrest [see comment]. Prehosp. Emerg. Care 1997, 1, 65–67. [Google Scholar] [CrossRef] [PubMed]
- Smereka, J.; Bielski, K.; Ladny, J.R.; Ruetzler, K.; Szarpak, L. Evaluation of a newly developed infant chest compression technique: A randomized crossover manikin trial. Medicine 2017, 96, e5915. [Google Scholar] [CrossRef] [PubMed]
- Millin, M.G.; Bogumil, D.; Fishe, J.N.; Burke, R.V. Comparing the two-finger versus two-thumb technique for single person infant CPR: A systematic review and meta-analysis. Resuscitation 2020, 148, 161–172. [Google Scholar] [CrossRef]
- Wu, M.Y.; Chien, Y.J.; Chang, C.Y. Comment on “Comparing the two-finger versus two-thumb technique for single person infant CPR: A systematic review and meta-analysis”. Resuscitation 2020, 150, 194–195. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Country | n | Comparison | CPR Duration (min) | Ventilation * | Manikin | Manikin Placement | Participants |
|---|---|---|---|---|---|---|---|---|
| Tsou et al., 2020 [25] | Taiwan | 42 | TT vs. TF | 2 | 30:2 | Resusci Baby QCPR (Laerdal) | Not mentioned | EMT, RN |
| Jo et al., 2017 [22] | Korea | 48 | OTTT vs. TF | 2 | 30:2 | Resusci Baby QCPR (Laerdal) | Bed | Medical students |
| Jiang et al., 2015 [24] | China | 27 | TT vs. TF | 5 | 30:2 | Resusci Baby QCPR (Laerdal) | Iliac crest | Physicians |
| Jo et al., 2015 [23] | Korea | 46 | OTTT vs. TF | 2 | 30:2 | Resusci Baby QCPR (Laerdal) | Bed | RN |
| Martin et al., 2013-A [26] | UK | 22 | TT vs. TF | 2 | No | The Laerdal ALS Baby Trainer | Table | Physicians, RN, resuscitation officers |
| Martin et al., 2013-B [27] | UK | 40 | TT vs. TF | 1.5 | No | Laerdal ALS Baby Trainer | Table | Resuscitation officer, physicians, RN, operating-room practitioner, paramedics |
| Martin et al., 2013-C [28] | UK | 35 | TT vs. TF | 1 | No | Laerdal ALS Baby Trainer | Not mentioned | Resuscitation officers, physicians, RN |
| Huynh et al., 2012 [29] | USA | 18 | TT vs. TF | 2 | 30:2 | Laerdal HeartCode BLS manikin | Floor | RN, NP, physicians |
| Christman et al., 2011 [30] | USA | 25 | TT vs. TF | 1 | No | Laerdal HeartCode BLS manikin | Not mentioned | Physicians, RN |
| Fakhraddin et al., 2011 [31] | Japan | 40 | TT vs. TF | 5 | No | Resusci Baby QCPR (Laerdal) | Not mentioned | PALS providers |
| Udassi et al., 2009 [32] | USA | 32 | TT vs. TF | 5 | 30:2 | Resusci Baby QCPR (Laerdal) | Iliac crest | RN, medical student, physicians, faculty, others |
| Haque et al., 2008 [21] | USA | 32 | TT vs. TF | 5 | 30:2 | Laerdal ALS Baby Trainer | Iliac crest | Faculty, physicians, RN, medical/nursing students, RT, OT |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, C.-Y.; Lin, P.-C.; Chien, Y.-J.; Chen, C.-S.; Wu, M.-Y. Analysis of Chest-Compression Depth and Full Recoil in Two Infant Chest-Compression Techniques Performed by a Single Rescuer: Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 4018. https://doi.org/10.3390/ijerph17114018
Chang C-Y, Lin P-C, Chien Y-J, Chen C-S, Wu M-Y. Analysis of Chest-Compression Depth and Full Recoil in Two Infant Chest-Compression Techniques Performed by a Single Rescuer: Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2020; 17(11):4018. https://doi.org/10.3390/ijerph17114018
Chicago/Turabian StyleChang, Chun-Yu, Po-Chen Lin, Yung-Jiun Chien, Chien-Sheng Chen, and Meng-Yu Wu. 2020. "Analysis of Chest-Compression Depth and Full Recoil in Two Infant Chest-Compression Techniques Performed by a Single Rescuer: Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 17, no. 11: 4018. https://doi.org/10.3390/ijerph17114018