Difference between Female and Male Patients with Oral Squamous Cell Carcinoma: A Single-Center Retrospective Study in Taiwan


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Clinical Parameters
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Chen, Y.K.; Huang, H.C.; Lin, L.M.; Lin, C.C. Primary oral squamous cell carcinoma: An analysis of 703 cases in southern Taiwan. Oral Oncol. 1999, 35, 173–179. [Google Scholar] [CrossRef]
- Liao, C.T.; Tung-Chieh Chang, J.T.; Wang, H.M.; Chen, I.H.; Lin, C.Y.; Chen, T.M.; Hsieh, L.L.; Cheng, A.J. Telomerase as an Independent Prognostic Factor in Head and Neck Squamous Cell Carcinoma. Head Neck 2004, 26, 504–512. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.T.; Chang, J.T.; Wang, H.M.; Ng, S.H.; Hsueh, C.; Lee, L.Y.; Lin, C.H.; Chen, I.H.; Huang, S.F.; Cheng, A.J.; et al. Analysis of risk factors of predictive local tumor control in oral cavity cancer. Ann. Surg. Oncol. 2008, 15, 915–922. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.T.; Kang, C.J.; Chang, J.T.; Wang, H.M.; Ng, S.H.; Hsueh, C.; Lee, L.Y.; Lin, C.H.; Cheng, A.J.; Chen, I.H.; et al. Survival of second and multiple primary tumors in patients with oral cavity squamous cell carcinoma in the betel quid chewing area. Oral Oncol. 2007, 43, 811–819. [Google Scholar] [CrossRef]
- Chen, Y.J.; Chang, J.T.; Liao, C.T.; Wang, H.M.; Yen, T.C.; Chiu, C.C.; Lu, Y.C.; Li, H.F.; Cheng, A.J. Head and Neck Cancer in the Betel Quid Chewing Area: Recent Advances in Molecular Carcinogenesis. Cancer Sci. 2008, 99, 1507–1514. [Google Scholar] [CrossRef]
- Kao, S.Y.; Lim, E. An overview of detection and screening of oral cancer in Taiwan. Chin. J. Dent. Res. 2015, 18, 7–12. [Google Scholar]
- Al Feghali, K.A.; Ghanem, A.I.; Burmeister, C.; Chang, S.S.; Ghanem, T.; Keller, C.; Siddiqui, F. Impact of smoking on pathological features in oral cavity squamous cell carcinoma. J. Can. Res. Ther. 2019, 15, 582–588. [Google Scholar]
- Blot, W.J.; McLaughlin, J.K.; Winn, D.M.; Austin, D.F.; Greenberg, R.S.; Preston-Martin, S.; Bernstein, L.; Schoenberg, J.B.; Stemhagen, A.; Fraumeni, J.F. Smoking and Drinking in Relation to Oral and Pharyngeal Cancer. Cancer Res. 1988, 48, 3282–3287. [Google Scholar]
- Hashibe, M.; Brennan, P.; Benhamou, S.; Castellsague, X.; Chen, C.; Curado, M.P.; Dal Maso, L.; Daudt, A.W.; Fabianova, E.; Fernandez, L.; et al. Alcohol drinking in never users of tobacco, cigarette smoking in never drinkers, and the risk of head and neck cancer: Pooled analysis in the International Head and Neck Cancer Epidemiology Consortium. J. Natl. Cancer Inst. 2007, 99, 777–789. [Google Scholar] [CrossRef]
- Lee, K.W.; Kuo, W.R.; Tsai, S.M.; Wu, D.C.; Wang, W.M.; Fang, F.M.; Chiang, F.Y.; Ho, K.Y.; Wang, L.F.; Tai, C.F.; et al. Different impact from betel quid, alcohol and cigarette: Risk factors for pharyngeal and laryngeal cancer. Int. J. Cancer 2005, 117, 831–836. [Google Scholar] [CrossRef]
- Ko, Y.C.; Huang, Y.L.; Lee, C.H.; Chen, M.J.; Lin, L.M.; Tsai, C.C. Betel quid chewing, cigarette smoking and alcohol consumption related to oral cancer in Taiwan. J. Oral Pathol. Med. 1995, 24, 450–453. [Google Scholar] [CrossRef] [PubMed]
- Kruse, A.L.; Bredell, M.; Grätz, K.W. Oral Cancer in men and women: Are there differences? Oral Maxillofac. Surg. 2011, 15, 51–55. [Google Scholar] [CrossRef] [PubMed]
- Annertz, K.; Anderson, H.; Palmér, K.; Wennerberg, J. The increase in incidence of cancer of the tongue in the Nordic countries continues into the twenty-first century. Acta Otolaryngol. 2012, 132, 552–557. [Google Scholar] [CrossRef] [PubMed]
- Ng, J.H.; Iyer, N.G.; Tan, M.H.; Edgren, G. Changing epidemiology of oral squamous cell carcinoma of the tongue: A global study. Head Neck 2017, 39, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Vettore, A.L.; Ramnarayanan, K.; Poore, G.; Lim, K.; Ong, C.K.; Huang, K.K.; Leong, H.S.; Chong, F.T.; Lim, T.K.; Lim, W.K.; et al. Mutational landscapes of tongue carcinoma reveal recurrent mutations in genes of therapeutic and prognostic relevance. Genome Med. 2015, 7, 98. [Google Scholar] [CrossRef] [Green Version]
- Rosenquist, K.; Wennerberg, J.; Schildt, E.B.; Bladströ>m, A.; Göran Hansson, B.G.; Andersson, G. Oral status, oral infections and some lifestyle factors as risk factors for oral and oropharyngeal squamous cell carcinoma. A population-based case-control study in southern Sweden. Acta Otolaryngol. 2005, 125, 1327–1336. [Google Scholar] [CrossRef]
- Liang, X.H.; Lewis, J.; Foote, R.; Smith, D.; Kademani, D. Prevalence and significance of human papillomavirus in oral tongue cancer: The Mayo Clinic experience. J. Oral Maxillofac. Surg. 2008, 66, 1875–1880. [Google Scholar] [CrossRef]
- Dahlgren, L.; Dahlstrand, H.M.; Lindquist, D.; Högmo, A.; Björnestål, L.; Lindholm, J.; Lundberg, B.; Dalianis, T.; Munck-Wikland, E. Human papillomavirus is more common in base of tongue than in mobile tongue cancer and is a favorable prognostic factor in base of tongue cancer patients. Int. J. Cancer 2004, 112, 1015–1019. [Google Scholar] [CrossRef]
- Kantola, S.; Parikka, M.; Jokinen, K.; Hyrynkangs, K.; Soini, Y.; Alho, O.P.; Salo, T. Prognostic factors in tongue cancer-relative importance of demographic, clinical and histopathological factors. Br. J. Cancer 2000, 83, 614–619. [Google Scholar] [CrossRef] [Green Version]
- Su, C.C.; Yang, H.F.; Huang, S.J.; Lian, l.B. Distinctive Features of Oral Cancer in Changhua County: High Incidence, Buccal Mucosa Preponderance, and a Close Relation to Betel Quid Chewing Habit. J. Formos. Med. Assoc. 2007, 106, 225–233. [Google Scholar] [CrossRef] [Green Version]
- Koyama, S.; Tabuchi, T.; Okawa, S.; Morishima, T.; Ishimoto, S.; Ishibashi, M.; Miyashiro, I. Oral cavity cancer incidence rates in Osaka, Japan between 2000 and 2014. Oral Oncol. 2020, 105, 104653. [Google Scholar] [CrossRef] [PubMed]
- Giraldi, L.; Leoncini, E.; Pastorino, R.; Wünsch-Filho, V.; de Carvalho, M.; Lopez, R.; Cadoni, G.; Arzani, D.; Petrelli, L.; Matsuo, K.; et al. Alcohol and cigarette consumption predict mortality in patients with head and neck cancer: A pooled analysis within the International Head and Neck Cancer Epidemiology (INHANCE) consortium. Ann. Oncol. 2017, 28, 2843–2851. [Google Scholar] [CrossRef] [PubMed]
- Kawakita, D.; Hosono, S.; Ito, H.; Oze, I.; Watanabe, M.; Hanai, N.; Hasegawa, Y.; Tajima, K.; Murakami, S.; Tanaka, H.; et al. Impact of smoking status on clinical outcome in oral cavity cancer patients. Oral Oncol. 2012, 48, 186–191. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Clinical Characteristics | Gender | Total | p-Value | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Female | Male | |||||||||
| n | Mean | SD | n | Mean | SD | n | Mean | SD | ||
| Age at diagnosis (years) | 122 | 61.7 | 15.1 | 2451 | 56.9 | 10.9 | 2573 | 57.2 | 11.1 | 0.001 |
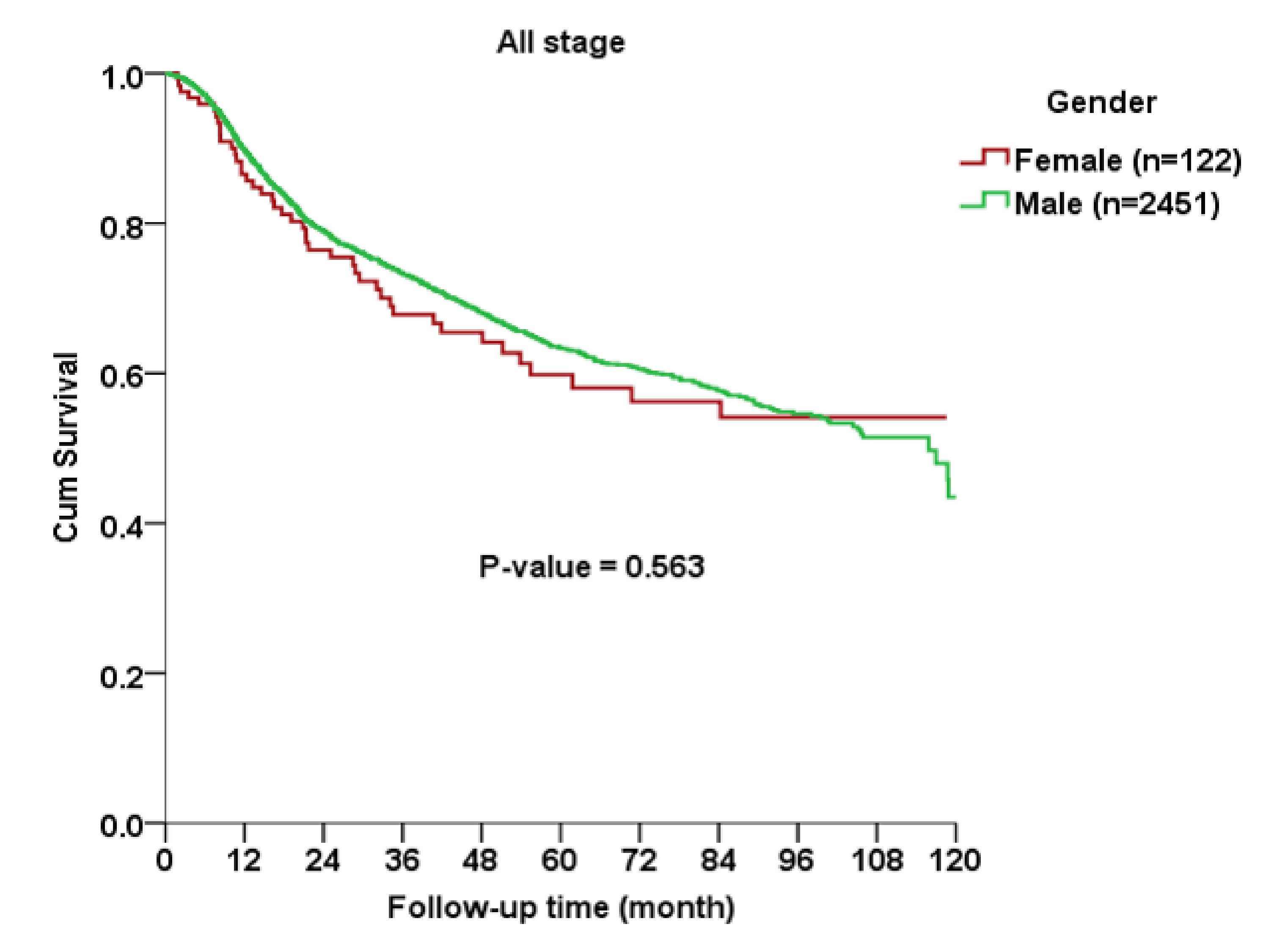
| Survival time * (months) | 122 | 45.4 | 33.8 | 2451 | 44.7 | 31.0 | 2573 | 44.7 | 31.1 | 0.824 |
| Time from diagnosis to recurrence (months) | 30 | 11.6 | 10.9 | 484 | 13.2 | 12.6 | 514 | 13.1 | 12.5 | 0.496 |
| Clinical and Pathological Characteristics | Gender | Total (n = 2573) | p-Value | |||||
|---|---|---|---|---|---|---|---|---|
| Female (n = 122) | Male (n = 2451) | |||||||
| n | % | n | % | n | % | |||
| Age (years) | ≤40 | 12 | 9.8 | 153 | 6.2 | 165 | 6.4 | <0.001 |
| 41–50 | 14 | 11.5 | 547 | 22.3 | 561 | 21.8 | ||
| 51–60 | 33 | 27.0 | 882 | 36.0 | 915 | 35.6 | ||
| 61–70 | 18 | 14.8 | 584 | 23.8 | 602 | 23.4 | ||
| ≥71 | 45 | 36.9 | 285 | 11.6 | 330 | 12.8 | ||
| AJCC anatomic site | Alveolar ridge | 18 | 14.8 | 401 | 16.4 | 419 | 16.3 | <0.001 |
| Anterior tongue | 64 | 52.5 | 669 | 27.3 | 733 | 28.5 | ||
| Buccal mucosa | 23 | 18.9 | 881 | 35.9 | 904 | 35.1 | ||
| Hard palate | 1 | 0.8 | 73 | 3.0 | 74 | 2.9 | ||
| Floor of the mouth | 1 | 0.8 | 76 | 3.1 | 77 | 3.0 | ||
| Retromolar trigone | 4 | 3.3 | 133 | 5.4 | 137 | 5.3 | ||
| Mucosa of the Lips | 11 | 9.0 | 218 | 8.9 | 229 | 8.9 | ||
| Smoking | No | 96 | 78.7 | 454 | 22.5 | 550 | 25.7 | <0.001 |
| Yes | 26 | 21.3 | 1562 | 77.5 | 1588 | 74.3 | ||
| Unknown | 0 | 435 | ||||||
| Betel nut chewing | No | 111 | 91.0 | 808 | 40.1 | 919 | 43.0 | <0.001 |
| Yes | 11 | 9.0 | 1208 | 59.9 | 1219 | 57.0 | ||
| Unknown | 0 | 435 | ||||||
| Alcohol | No | 116 | 95.1 | 844 | 47.5 | 960 | 50.6 | <0.001 |
| Yes | 6 | 4.9 | 931 | 52.5 | 937 | 49.4 | ||
| Unknown | 0 | 676 | ||||||
| AJCC Stage | I | 62 | 50.8 | 942 | 39.3 | 1004 | 39.8 | 0.089 |
| II | 19 | 15.6 | 444 | 18.5 | 463 | 18.4 | ||
| III | 9 | 7.4 | 207 | 8.6 | 216 | 8.6 | ||
| IV | 32 | 26.2 | 805 | 33.6 | 837 | 33.2 | ||
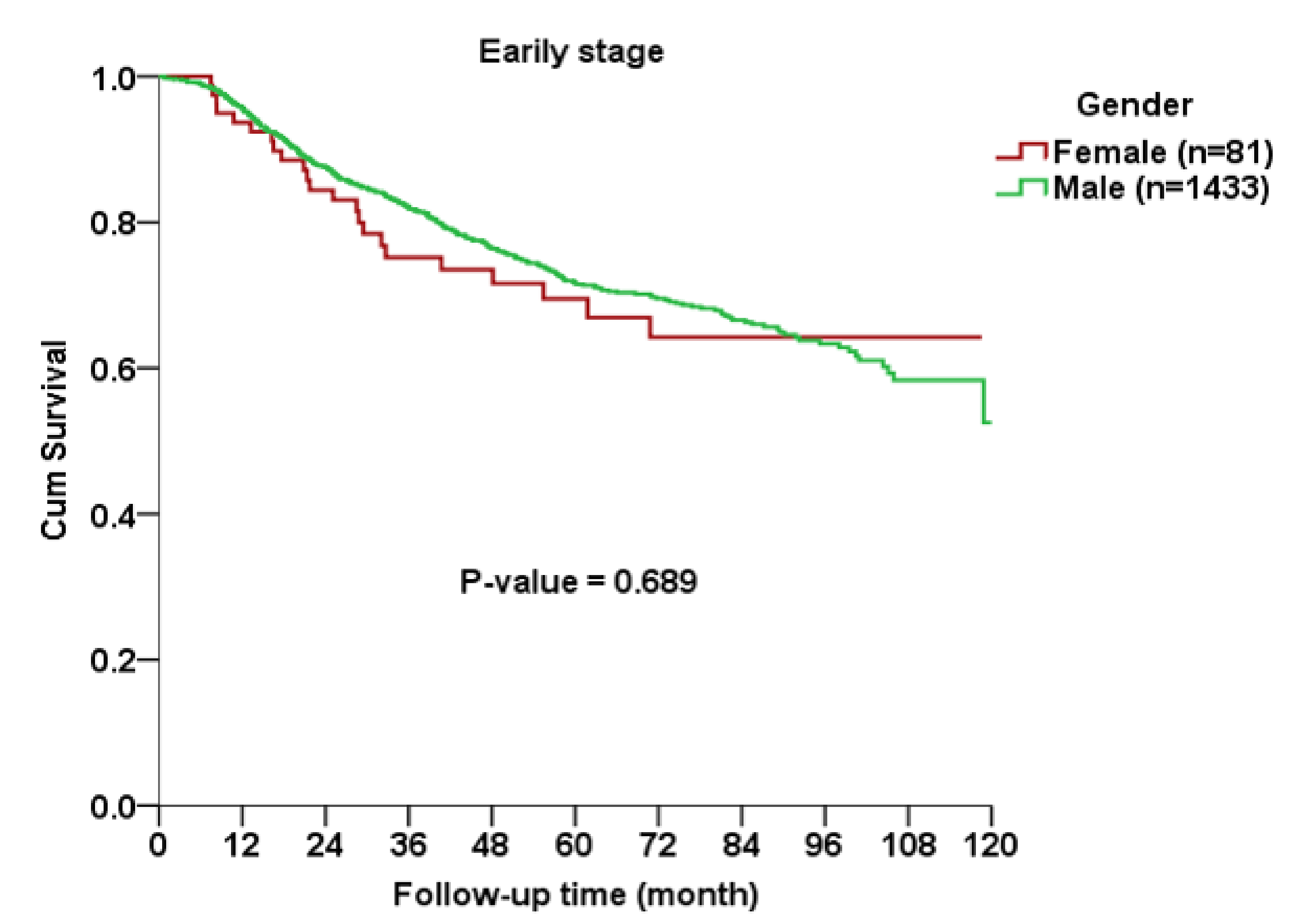
| AJCC Stage | Early (I and II) | 81 | 66.4 | 1433 | 58.5 | 1514 | 58.8 | 0.082 |
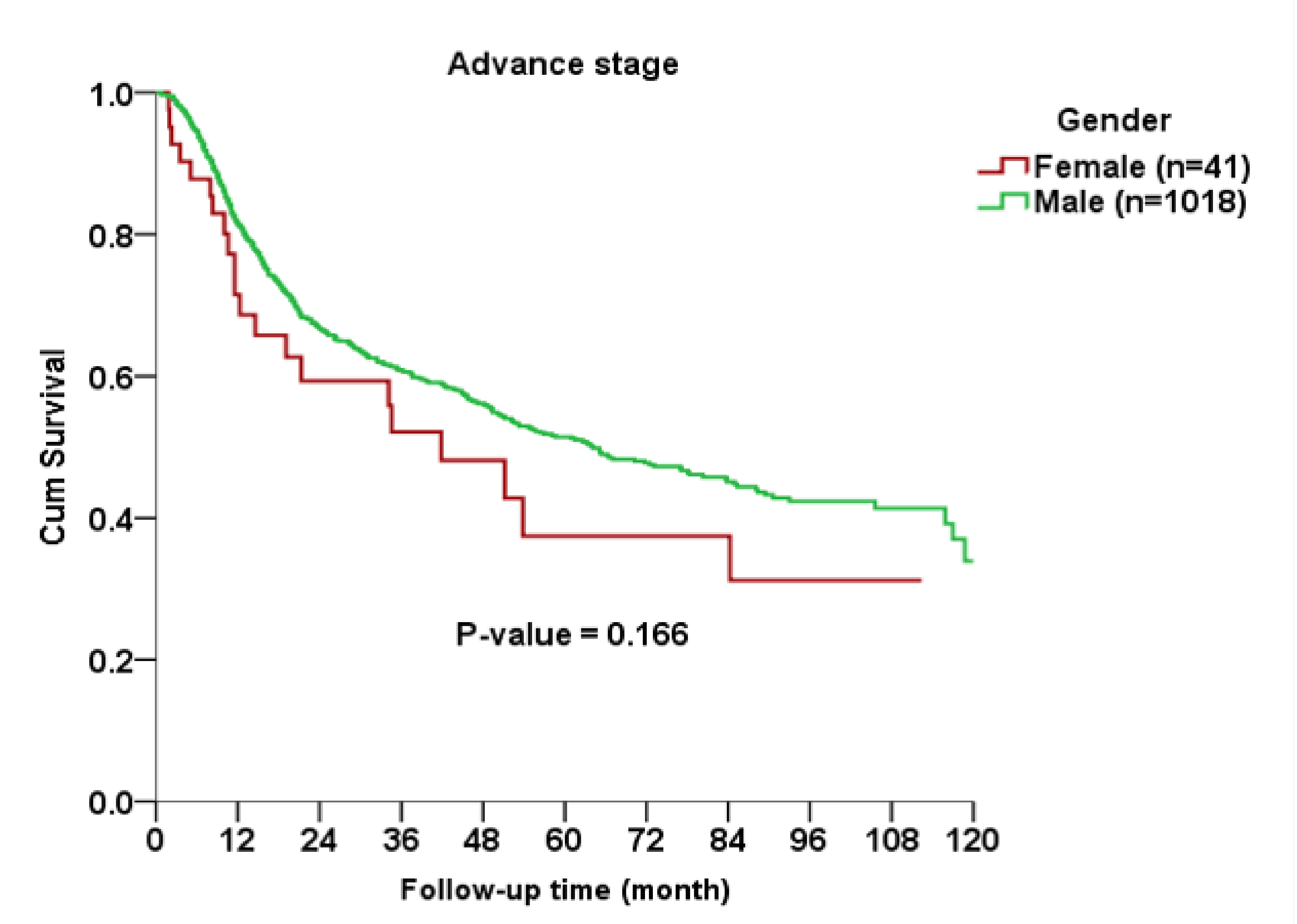
| Advance (III and IV) | 41 | 33.6 | 1018 | 41.5 | 1059 | 41.2 | ||
| T stage | 1 | 66 | 54.1 | 1064 | 43.6 | 1130 | 43.9 | 0.129 |
| 2 | 26 | 21.3 | 578 | 23.6 | 604 | 23.5 | ||
| 3 | 5 | 4.1 | 148 | 6.0 | 153 | 5.9 | ||
| 4 | 25 | 20.5 | 653 | 26.7 | 678 | 26.4 | ||
| N stage | 0 | 62 | 70.5 | 1368 | 73.0 | 1430 | 72.9 | 0.247 |
| 1 | 13 | 14.8 | 170 | 9.1 | 183 | 9.3 | ||
| 2 | 11 | 12.5 | 308 | 16.4 | 319 | 16.3 | ||
| 3 | 2 | 2.3 | 28 | 1.5 | 30 | 1.5 | ||
| Extranodal spread | No | 76 | 84.4 | 1539 | 85.4 | 1615 | 85.4 | 0.801 |
| Yes | 14 | 15.6 | 263 | 14.6 | 277 | 14.6 | ||
| Close margin | No | 115 | 94.3 | 2368 | 96.6 | 2483 | 96.5 | 0.197 |
| Yes | 7 | 5.7 | 83 | 3.4 | 90 | 3.5 | ||
| Recurrence | No | 92 | 75.4 | 1967 | 80.3 | 2059 | 80.0 | 0.192 |
| Yes | 30 | 24.6 | 484 | 19.7 | 514 | 20.0 | ||
| Grade | Well | 12 | 10.1 | 423 | 17.5 | 435 | 17.2 | 0.076 |
| Moderately | 98 | 82.4 | 1866 | 77.2 | 1964 | 77.5 | ||
| Poor | 9 | 7.6 | 127 | 5.3 | 136 | 5.4 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, N.-C.; Hsu, J.-T.; Tsai, K.-Y. Difference between Female and Male Patients with Oral Squamous Cell Carcinoma: A Single-Center Retrospective Study in Taiwan. Int. J. Environ. Res. Public Health 2020, 17, 3978. https://doi.org/10.3390/ijerph17113978
Lin N-C, Hsu J-T, Tsai K-Y. Difference between Female and Male Patients with Oral Squamous Cell Carcinoma: A Single-Center Retrospective Study in Taiwan. International Journal of Environmental Research and Public Health. 2020; 17(11):3978. https://doi.org/10.3390/ijerph17113978
Chicago/Turabian StyleLin, Nan-Chin, Jui-Ting Hsu, and Kuo-Yang Tsai. 2020. "Difference between Female and Male Patients with Oral Squamous Cell Carcinoma: A Single-Center Retrospective Study in Taiwan" International Journal of Environmental Research and Public Health 17, no. 11: 3978. https://doi.org/10.3390/ijerph17113978