Infections of Deep Hand and Wrist Compartments

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Anatomical Compartments and Pathogenesis of the Deep Space Infections in the Hand
3. Pathogens
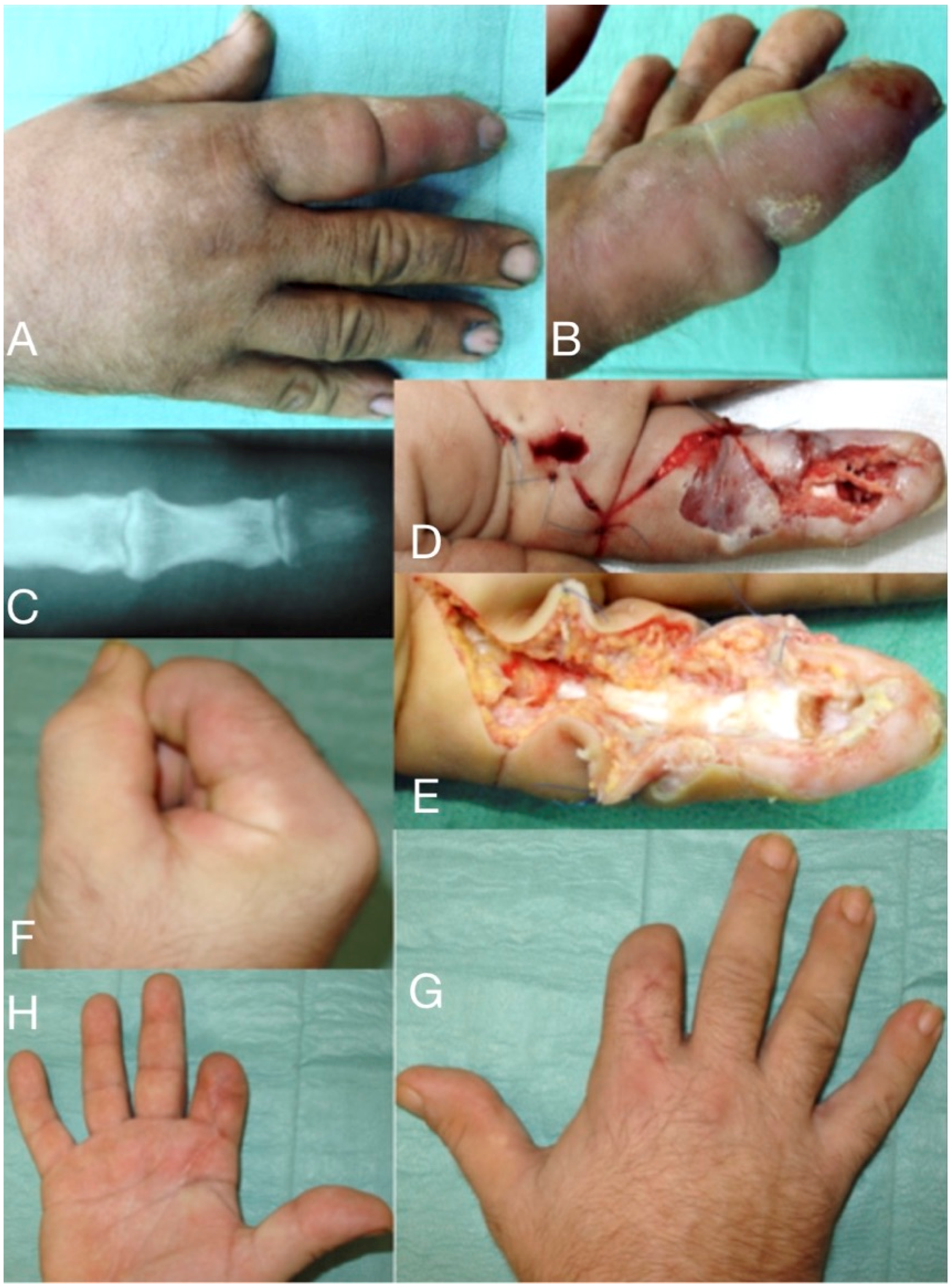
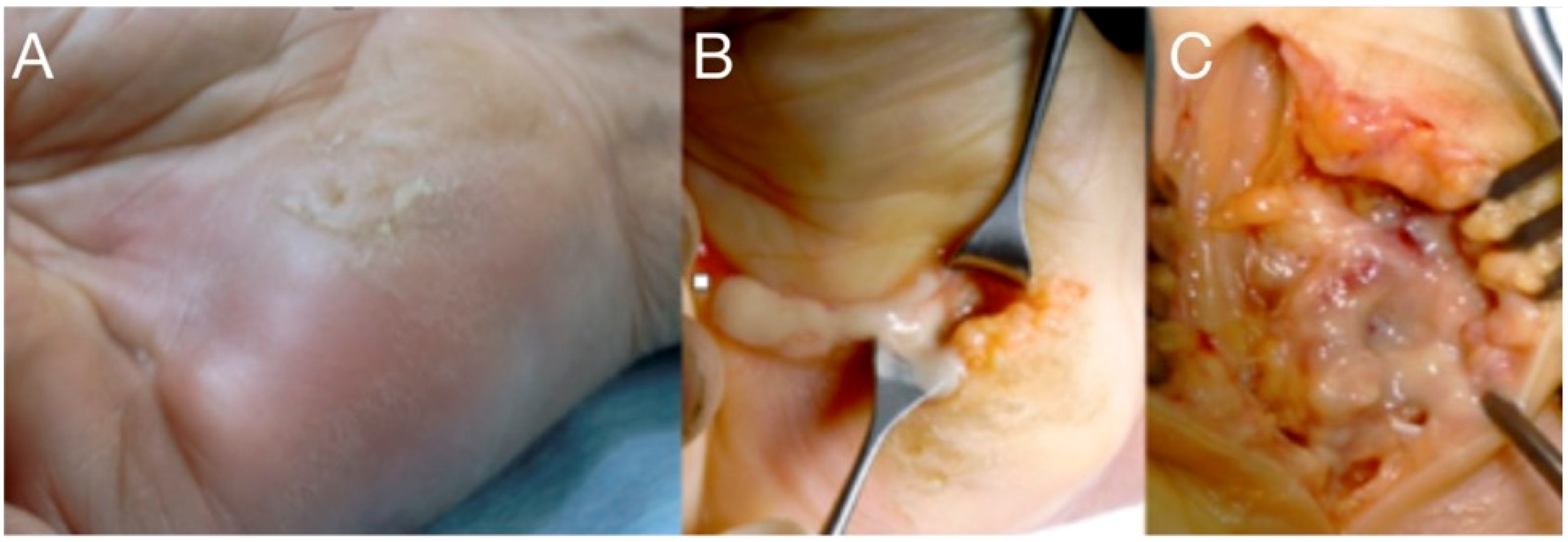
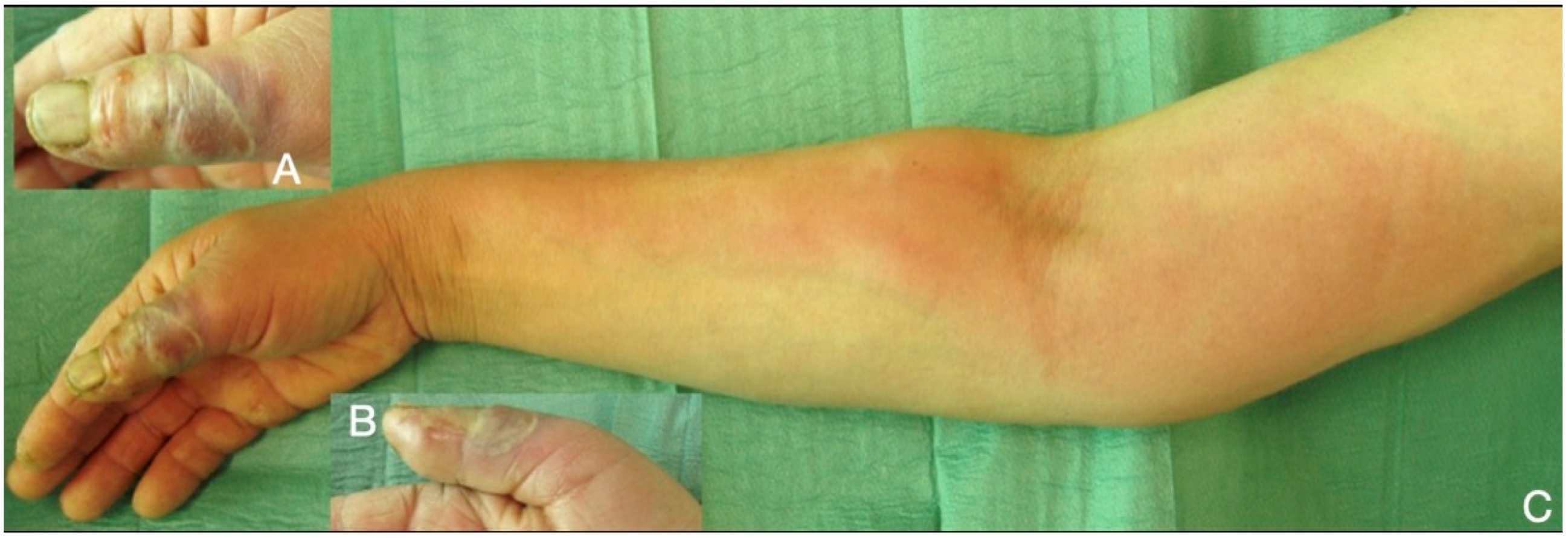
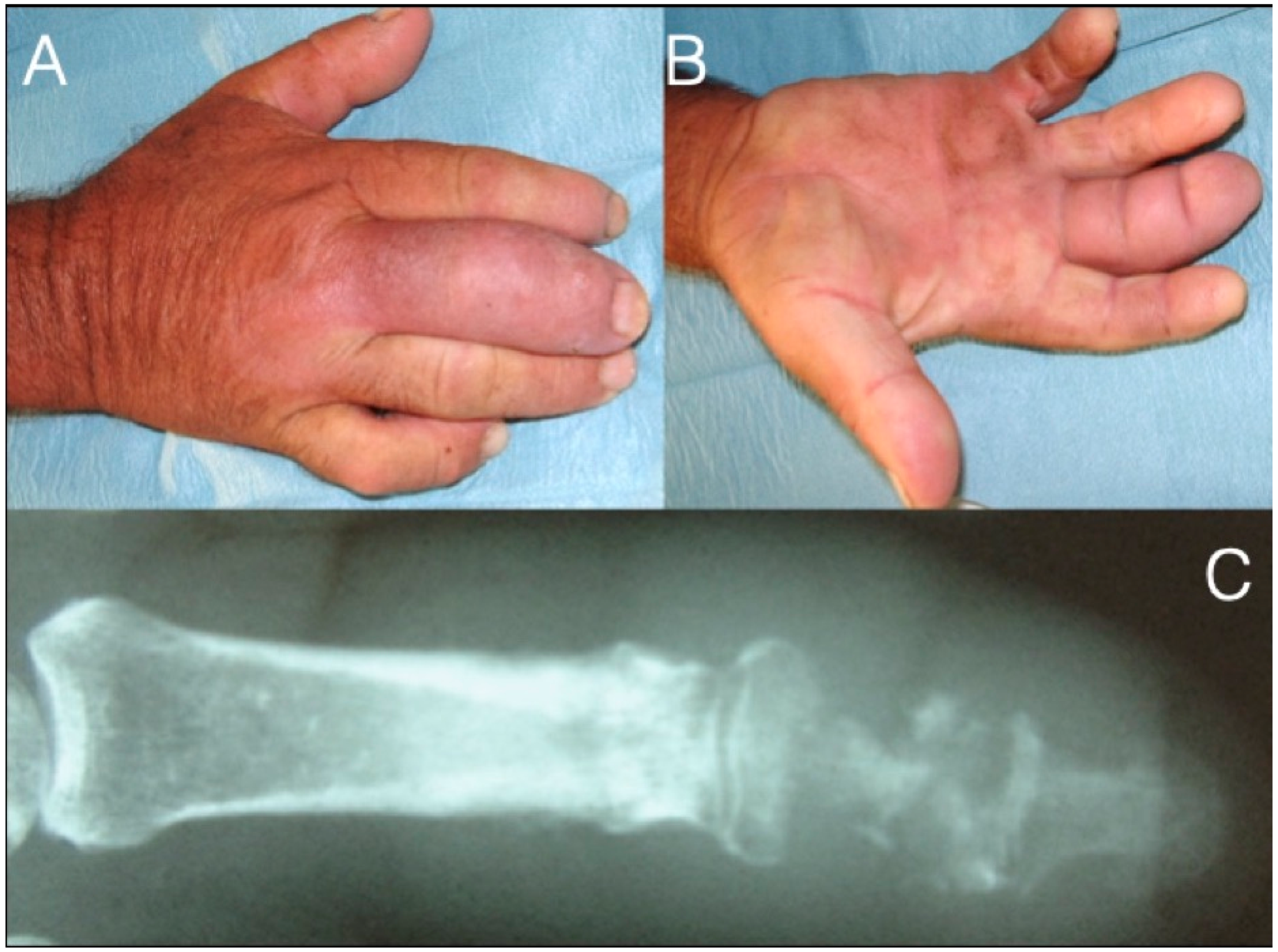
4. Clinical Appearance and Diagnosis
5. Therapeutic Approach
6. Infections at the Deep Anatomical Compartments
Author Contributions
Funding
Conflicts of Interest
References
- Flynn, J.E. Modern considerations of major hand infections. N. Engl. J. Med. 1955, 252, 605–612. [Google Scholar] [CrossRef] [PubMed]
- Belcher, H.J.C.; Clare, T.D. Hand infections. Curr. Orthop. 2003, 17, 28–43. [Google Scholar] [CrossRef]
- McDonald, L.S.; Bavaro, M.F.; Hofmeister, E.P.; Kroonen, L.T. Hand infections. J. Hand Surg. 2011, 36, 1403–1412. [Google Scholar] [CrossRef] [PubMed]
- Afrăsânie, V.A.; Adavidoaiei, A.M.; Zamisnicu, I.H.; Funingănă, I.G.; Marinca, M.V.; Gafton, B.; Clement, D.E.; Păduraru, M.I.; Demşa, I.; Miron, L.; et al. A very rare presentation of lung cancer: Metastases to the distal phalanx of index-case report. Medicine 2019, 98, e17892. [Google Scholar] [CrossRef] [PubMed]
- Szabo, R.M.; Spiegel, J.D. Infected fractures of the hand and wrist. Hand Clin. 1988, 4, 477–489. [Google Scholar]
- Neviaser, R.J. Tenosynovitis. Hand Clin. 1989, 5, 525–531. [Google Scholar]
- Crosswell, S.; Vanat, Q.; Jose, R. The anatomy of deep hand space infections: The deep thenar space. J. Hand Surg. 2014, 39, 2550. [Google Scholar] [CrossRef]
- Patel, D.B.; Emmanuel, N.B.; Stevanovic, M.V.; Matcuk, G.R., Jr.; Gottsegen, C.J.; Forrester, D.M.; White, E.A. Hand infections: Anatomy, types and spread of infection, imaging findings, and treatment options. Radiographics 2014, 34, 1968–1986. [Google Scholar] [CrossRef] [Green Version]
- Afshar, A.; Farhadnia, P.; Khalkhali, H. Metastases to the hand and wrist: An analysis of 221 cases. J. Hand Surg. 2014, 39, 923–932. [Google Scholar] [CrossRef]
- Chaput, B.; Nouaille de Gorce, H.; Courtade-Saïdi, M.; Apredoaei, C.; Rongières, M.; Chavoin, J.P.; Grolleau, J.L.; Garrido, I. The role of a systematic second look at 48–72 h in high pressure injection injuries to the hand: A retrospective study. Chir. Main 2012, 31, 250–255. [Google Scholar] [CrossRef]
- Kistler, J.M.; Thoder, J.J.; Ilyas, A.M. MRSA incidence and antibiotic trends in urban hand infections: A 10-year longitudinal study. Hand 2019, 14, 449–454. [Google Scholar] [CrossRef] [PubMed]
- Dailiana, Z.H.; Rigopoulos, N.; Varitimidis, S.E.; Poultsides, L.; Petinaki, E.; Malizos, K.N. Clinical and epidemiological features of upper-extremity infections caused by Staphylococcus aureus carrying the PVL gene: A four-year study in Greece. Med. Sci. Monit. 2008, 14, CR511–CR514. [Google Scholar] [PubMed]
- Tosti, R.; Trionfo, A.; Gaughan, J.; Ilyas, A.M. Risk factors associated with clindamycin-resistant, methicillin-resistant Staphylococcus aureus in hand abscesses. J. Hand Surg. 2015, 40, 673–676. [Google Scholar] [CrossRef] [PubMed]
- Mann, R.J.; Peacock, J.M. Hand infections in patients with diabetes mellitus. J. Trauma 1977, 17, 376–380. [Google Scholar] [CrossRef]
- Houshian, S.; Seyedipour, S.; Wedderkopp, N. Epidemiology of bacterial hand infections. Int. J. Infect. Dis. 2006, 10, 315–319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldstein, E.J.C. Bite wounds and infection. Clin. Infect. Dis. 1992, 14, 633–638. [Google Scholar] [CrossRef]
- Johnson, M.G.; Stout, J.E. Twenty-eight cases of Mycobacterium marinum infection: Retrospective case series and literature review. Infection 2015, 43, 655–662. [Google Scholar] [CrossRef]
- Chiba, M.; Yanaba, K.; Kohara, A.; Nakayama, M.; Nakagawa, H.; Fukuda, T.; Ishii, N.; Yoshida, K. Septic arthritis caused by Mycobacterium marinum infection. J. Dermatol. 2017, 44, 1179–1180. [Google Scholar] [CrossRef]
- McLain, R.F.; Steyers, C.; Stoddard, M. Infections in open fractures of the hand. J. Hand Surg. 1991, 16, 108–112. [Google Scholar] [CrossRef]
- Rhee, P.; Nunley, M.K.; Demetriades, D.; Velmachos, G.; Doucet, J.J. Tetanus and trauma: Review and recommendations. J. Trauma 2005, 58, 1082–1088. [Google Scholar] [CrossRef]
- Wiese-Posselt, M.; Tertilt, C.; Zepp, F. Vaccination recommendations for Germany. Dtsch. Arztebl. Int. 2011, 108, 771–779. [Google Scholar] [CrossRef]
- Sharma, K.; Mull, A.; Friedman, J.; Pan, D.; Poppler, L.; Fox, I.K.; Levin, L.S.; Moore, A.M. Development and validation of a prognostic, risk-adjusted scoring system for operative upper-extremity infections. J. Hand Surg. 2020, 45, 9–19. [Google Scholar] [CrossRef]
- Prunières, G.; Igeta, Y.; Hidalgo Díaz, J.J.; Gouzou, S.; Facca, S.; Xavier, F.; Liverneaux, P. Ultrasound for the diagnosis of pyogenic flexor tenosynovitis. Hand Surg. Rehabil. 2018, 27, 243–246. [Google Scholar] [CrossRef] [PubMed]
- Eberlin, K.R.; Ring, D. Infection after hand surgery. Hand Clin. 2015, 31, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Jardin, E.; Delord, M.; Aubry, S.; Loisel, F.; Obert, L. Usefulness of ultrasound for the diagnosis of pyogenic flexor tenosynovitis: A prospective single-center study of 57 cases. Hand Surg. Rehabil. 2018, 37, 95–98. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, J.; Mailhot, T.; Chilstrom, M. Point-of-Care Ultrasound Diagnosis of Deep Space Hand Infection. J. Emerg. Med. 2016, 50, 458–461. [Google Scholar] [CrossRef] [PubMed]
- Ridley, L.J.; Han, J.; Ridley, W.E.; Xiang, H. Horseshoe abscess: Hand. J. Med. Imaging Radiat. Oncol. 2018, 62, 143. [Google Scholar] [CrossRef]
- Kanavel, A.B. The symptoms, signs, and diagnosis of tenosynovitis and fascial-space abscesses. In Infections of the Hand, 1st ed.; Lea & Febiger: Philadelphia, PA, USA, 1912; pp. 201–226. [Google Scholar]
- Flevas, D.A.; Syngouna, S.; Fandridis, E.; Tsiodras, S.; Mavrogenis, A.F. Infections of the hand: An overview. EFORT Open Rev. 2019, 4, 183–193. [Google Scholar] [CrossRef]
- Neviaser, R.J. Closed tendon sheath irrigation for pyogenic flexor tenosynovitis. J. Hand Surg. 1978, 3, 462–466. [Google Scholar] [CrossRef]
- Giladi, A.M.; Malay, S.; Chung, K.C. A systematic review of the management of acute pyogenic flexor tenosynovitis. J. Hand Surg. 2015, 40, 720–728. [Google Scholar] [CrossRef] [Green Version]
- Chow, S.P.; Pun, W.K.; So, Y.C.; Luk, K.D.; Chiu, K.Y.; Ng, K.H.; Ng, C.; Crosby, C.A. Prospective study of 245 open distal fractures of the hand. J. Hand Surg. 1991, 16, 137–140. [Google Scholar] [CrossRef]
- Dailiana, Z.H.; Rigopoulos, N.; Varitimidis, S.; Hantes, M.; Bargiotas, K.; Malizos, K.N. Purulent flexor tenosynovitis: Factors influencing the functional outcome. J. Hand Surg. 2008, 33, 280–285. [Google Scholar] [CrossRef]
- Hansen, A.D.; Amadio, P.C.; DeSilva, S.P.; Ilstrup, D.M. Deep postoperative wound infection after carpal tunnel release. J. Hand Surg. 1989, 14, 869–873. [Google Scholar] [CrossRef]
- Gosain, A.K.; Markison, R.E. Catheter Irrigation for Treatment of Pyogenic Closed Space Infections of the Hand. Br. J. Plast. Surg. 1991, 44, 270–273. [Google Scholar] [CrossRef]
- Chapman, T.; Ilyas, A.M. Pyogenic Flexor Tenosynovitis: Evaluation and Treatment Strategies. J. Hand Surg. 2019, 44, 981–985. [Google Scholar] [CrossRef]
- Schnall, S.B.; Vu-Rose, T.; Holtom, P.D.; Doyle, B.; Stevanovic, M. Tissue pressures in pyogenic flexor tenosynovitis of the finger: Compartment syndrome and its management. J. Bone Jt. Surg. Br. 1996, 78, 792–795. [Google Scholar] [CrossRef] [Green Version]
- Rigopoulos, N.; Dailiana, Z.H.; Varitimidis, S.; Malizos, K.N. Closed-space hand infections: Diagnostic and treatment considerations. Orthop. Rev. 2012, 4, e19. [Google Scholar] [CrossRef] [Green Version]
- Sharma, K.S.; Rao, K.; Hobson, M.I. Space of Parona infections: Experience in management and outcomes in a regional hand centre. J. Plast. Reconstr. Aesthet. Surg. 2013, 66, 968–972. [Google Scholar] [CrossRef]
- Speirs, J.; Showery, J.; Abdou, M.; Pirela-Cruz, M.A.; Abdelgawad, A.A. Dog bites to the upper extremity in children. J. Paediatr. Child Health 2015, 51, 1172–1174. [Google Scholar] [CrossRef]
- Bula-Rudas, F.J.; Olcott, J.L. Human and Animal Bites. Pediatr. Rev. 2018, 39, 490–500. [Google Scholar] [CrossRef]
- Daniels, D.M.; Ritzi, R.B.S.; O’Neil, J.; Scherer, L.R. Analysis of nonfatal dog bites in children. J. Trauma 2009, 66, 17–22. [Google Scholar] [CrossRef]
- Kheiran, A.; Palial, V.; Rollett, R.; Wildin, C.J.; Chatterji, U.; Singh, H.P. Cat bite: An injury not to underestimate. J. Plast. Surg. Hand Surg. 2019, 53, 341–346. [Google Scholar] [CrossRef]
- Schalamon, J.; Ainoedhofer, H.; Singer, G.; Petnehazy, T.; Mayr, J.; Kiss, K.; Höllwarth, M.E. Analysis of dog bites in children who are younger than 17 years. Pediatrics 2006, 117, e374–e379. [Google Scholar] [CrossRef] [Green Version]
- Morgan, M.; Palmer, J. Dog bites. BMJ 2007, 334, 413–417. [Google Scholar] [CrossRef]
- Gonzalez, M.H.; Papierski, P.; Hall, R.F., Jr. Osteomyelitis of the hand after a human bite. J. Hand Surg. 1993, 18, 520–522. [Google Scholar] [CrossRef]
- Cheah, A.E.; Chong, A.K. Bites to the hand: Are they more than we can chew? Singap. Med. J. 2011, 52, 715–718. [Google Scholar]
- Raval, P.; Khan, W.; Haddad, B.; Mahapatra, A.N. Bite injuries to the hand: Review of the literature. Open Orthop. J. 2014, 8, 204–208. [Google Scholar] [CrossRef]
- Ellis, R.; Ellis, C. Dog and cat bites. Am. Fam. Physician 2014, 90, 239–243. [Google Scholar]
- Howell, R.D.; Sapienza, A. The Management of Domestic Animal Bites to the Hand. Bull. Hosp. Jt. Dis. 2015, 73, 156–160. [Google Scholar]
- Medeiros, I.; Sacaonato, H. Antibiotic Prophylaxis for mammalian bites. Cochrane Database Syst. Rev. 2001. [Google Scholar] [CrossRef]
- Phair, I.C.; Quinton, D.N. Clenched fist human bite injuries. J. Hand Surg. 1989, 14, 86–87. [Google Scholar] [CrossRef]
- Shoji, K.; Cavanaugh, Z.; Rodner, C. Acute fight bite. J. Hand Surg. 2013, 18, 1612–1614. [Google Scholar] [CrossRef]
- Faciszewski, T.; Coleman, D.A. Human bite wounds. Hand Clin. 1989, 5, 561–569. [Google Scholar] [PubMed]
- Smith, H.R.; Hartman, H.; Loveridge, J.; Gunnarsson, R. Predicting serious complications and high cost of treatment of tooth-knuckle injuries: A systematic literature review. Eur. J. Trauma Emerg. Surg. 2016, 42, 701–710. [Google Scholar] [CrossRef]
- Goldstein, E.J.; Miller, T.A.; Citron, D.M.; Finegold, S.M. Infections following clenched-fist injury: A new perspective. J. Hand Surg. 1978, 3, 455–457. [Google Scholar] [CrossRef]
- Patzakis, M.J.; Wilkins, J.; Bassett, R.L. Surgical findings in clenched-fist injuries. Clin. Orthop. Relat. Res. 1987, 237–240. [Google Scholar] [CrossRef]
- De Smet, L.; Stoffelen, D. Clenched fist injury: A pitfall for patients and surgeons. Deep space abscess. Acta Orthop. Belg. 1997, 63, 113–117. [Google Scholar]
- Berlet, G.; Richards, R.S.; Roth, J.H. Clenched-fist injury complicated by methicillin-resistant Staphylococcus aureus. Can. J. Surg. 1997, 40, 313–314. [Google Scholar]
- Sternberg, M.L.; Jacobs, T. Clenched fist injury. J. Emerg. Med. 2010, 39, 97. [Google Scholar] [CrossRef]
- Shewring, D.J.; Trickett, R.W.; Subramanian, K.N.; Hnyda, R. The management of clenched fist ‘fight bite’ injuries of the hand. J. Hand Surg. 2015, 40, 819–824. [Google Scholar] [CrossRef]
- Murray, P.M. Septic arthritis of the hand and wrist. Hand Clin. 1998, 14, 579–587. [Google Scholar]
- Sinha, M.; Jain, S.; Woods, D.A. Septic arthritis of the small joints of the hand. J. Hand Surg. 2006, 31, 665–672. [Google Scholar] [CrossRef] [PubMed]
- Mathews, C.J.; Kingsley, G.; Field, M.; Jones, A.; Weston, V.C.; Phillips, M.; Walker, D.; Coakley, G. Management of septic arthritis: A systematic review. Ann. Rheum. Dis. 2007, 66, 440–445. [Google Scholar] [CrossRef]
- Kowalski, T.J.; Thompson, L.A.; Gundrum, J.D. Antimicrobial management of septic arthritis of the hand and wrist. Infection 2014, 42, 379–384. [Google Scholar] [CrossRef] [PubMed]
- Yap, R.T.; Tay, S.C. Wrist septic arthritis: An 11year review. Hand Surg. 2015, 20, 391–395. [Google Scholar] [CrossRef]
- Jennings, J.D.; Zielinski, E.; Tosti, R.; Ilyas, A.M. Septic arthritis of the wrist: Incidence, risk factors, and predictors of infection. Orthopedics 2017, 40, e526–e531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reilly, K.E.; Linz, J.C.; Stern, P.J.; Giza, E.; Wyrick, J.D. Osteomyelitis of the tubular bones of the hand. J. Hand Surg. 1997, 22, 644–649. [Google Scholar] [CrossRef]
- Barbieri, R.A.; Freeland, A.E. Osteomyelitis of the hand. Hand Clin. 1998, 14, 589–603. [Google Scholar]
- Honda, H.; Mcdonald, J.R. Current recommendations in the management of osteomyelitis of the hand and wrist. J. Hand Surg. 2009, 34, 1135–1136. [Google Scholar] [CrossRef] [Green Version]
- Pinder, R.; Barlow, G. Osteomyelitis of the hand. J. Hand Surg. 2016, 41, 431–440. [Google Scholar] [CrossRef]
- Rivas Felice, J.; González Herranz, P.; Mejía Casado, A.; Pérez Navarro, R.; Hernández Díaz, R. Chronic recurrent osteomyelitis: A diagnostic and therapeutic challenge. Rev. Española Cir. Ortop. Traumatol. 2017, 61, 35–42. [Google Scholar] [CrossRef]
- Xing, K.; Huang, G.; Hua, S.; Xu, G.; Li, M. Systematic review of randomised controlled trials on antibiotic treatment for osteomyelitis in diabetes. Diabet. Med. 2019, 36, 546–556. [Google Scholar] [CrossRef] [PubMed]
- Dadras, M.; Böhm, C.; Wallner, C.; Wagner, J.M.; Behr, B.; Lehnhardt, M.; Daigeler, A. Long-term results of bacterial septic arthritis of the wrist. J. Plast. Reconstr. Aesthet. Surg. 2018, 71, 1138–1145. [Google Scholar] [CrossRef] [PubMed]
- Karl, J.S.; Summer, D.M.; Pezeshk, R.A.; Cheng, J. Oral antibiotics are effective for the treatment of hand osteomyelitis in children. Hand 2020, 15, 220–223. [Google Scholar]
- Schecter, W.; Meyer, A.; Schecter, G.; Giuliano, A.; Newmeyer, W.; Kilgore, E. Necrotizing fasciitis of the upper extremity. J. Hand Surg. 1982, 7, 15–20. [Google Scholar] [CrossRef]
- Pessa, M.E.; Howard, R.J. Necrotizing fasciitis. Surg. Gynecol. Obstet. 1985, 161, 357–361. [Google Scholar]
- Wilkerson, R.; Paull, W.; Coville, F.V. Necrotizing fasciitis. Review of the literature and case report. Clin. Orthop. Relat. Res. 1987, 216, 187–192. [Google Scholar]
- Gonzalez, M.H. Necrotizing fasciitis and gangrene of the upper extremity. Hand Clin. 1998, 14, 635–645. [Google Scholar]
- Huang, K.C.; Hsieh, P.H.; Huang, K.C.; Tsai, Y.H. Vibrio necrotizing soft-tissue infection of the upper extremity: Factors predictive of amputation and death. J. Infect. 2008, 57, 290–297. [Google Scholar] [CrossRef]
- Ryssel, H.; Germann, G.; Kloeters, O.; Radu, C.A.; Reichenberger, M.; Gazyakan, E. Necrotizing fasciitis of the extremities: 34 cases at a single centre over the past 5 years. Arch. Orthop. Trauma Surg. 2010, 130, 1515–1522. [Google Scholar] [CrossRef]
- Chauhan, H.; Patil, S.; Hajare, A.; Krishnaprasad, K.; Bhargava, A. Necrotizing Fasciitis of Hand By Methicillin Resistant Staphylococcus aureus (MRSA)—A Sinister. J. Clin. Diagn. Res. 2015, 9. [Google Scholar] [CrossRef]
- Nawijn, F.; Smeeing, D.P.J.; Houwert, R.M.; Leenen, L.P.H.; Hietbrink, F. Time is of the essence when treating necrotizing soft tissue infections: A systematic review and meta-analysis. World J. Emerg. Surg. 2020, 15, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]








© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malizos, K.N.; Papadopoulou, Z.K.; Ziogkou, A.N.; Rigopoulos, N.; Athanaselis, E.D.; Varitimidis, S.E.; Dailiana, Z.C. Infections of Deep Hand and Wrist Compartments. Microorganisms 2020, 8, 838. https://doi.org/10.3390/microorganisms8060838
Malizos KN, Papadopoulou ZK, Ziogkou AN, Rigopoulos N, Athanaselis ED, Varitimidis SE, Dailiana ZC. Infections of Deep Hand and Wrist Compartments. Microorganisms. 2020; 8(6):838. https://doi.org/10.3390/microorganisms8060838
Chicago/Turabian StyleMalizos, Konstantinos N., Zoe K. Papadopoulou, Anna N. Ziogkou, Nikolaos Rigopoulos, Efstratios D. Athanaselis, Socrates E. Varitimidis, and Zoe C. Dailiana. 2020. "Infections of Deep Hand and Wrist Compartments" Microorganisms 8, no. 6: 838. https://doi.org/10.3390/microorganisms8060838