Article Text

Abstract
Background Remote ischaemic preconditioning (RIPC) is the exposure of body parts to brief periods of circulatory occlusion and reperfusion. Recent studies have also shown that RIPC can improve exercise performance in healthy individuals.
Objective This study aimed to assess the effect of RIPC on walking in people with multiple sclerosis (MS).
Methods This was a double-blind randomised controlled clinical trial. We used three cycles of RIPC delivered by occluding the upper arm with a blood pressure (BP) cuff inflated to a pressure of 30 mm Hg above the systolic BP. In patients in the sham intervention group, the BP cuff was inflated only to 30 mm Hg below diastolic BP. Outcome measures included the Six-Minute Walk Test (6MWT), gait speed, the Borg rate of perceived exertion (RPE) scale, the tolerability of the RIPC using a Numerical Rating Scale for discomfort from 0 to 10, and adverse events. We identified responders meeting the minimal clinically important difference (MCID) established in the literature in each group.
Results Seventy-five participants completed the study (RIPC: 38 and Sham: 37). The distance walked during the 6MWT improved by 1.9% in the sham group and 5.7% in the RIPC group (p=0.012). The number of responders meeting MCID criteria in the RIPC group was significantly greater compared with the sham intervention group. No serious adverse events occurred.
Conclusion Single cycle of RIPC resulted in immediate improvement in walking distances during 6MWT in people with MS.
Trial registration numbers NCT03153553
- multiple sclerosis
- remote ischemic preconditioning
- fatigue
- gait
- exercise tolerance
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Regular physical activity improves physical fitness, fatigue, quality of life and gait and also reduces the rate of progression of disability in individuals with multiple sclerosis (MS).1 However, individuals with MS are less physically active than the general population. Around 78% of people with MS do not participate in any regular physical activity.2 People with MS often experience problems with gait that limit their participation in physical activity. Problems with gait is a concern for 85% of people with MS.3 Loss of ambulation in people with MS is due to multiple factors such as muscle weakness, spasticity, ataxia and loss of proprioception. Ongoing disease progression and deconditioning facilitates a self-fulfilling cycle of progressive inactivity. People with MS who are unable to walk are at risk of developing adverse health conditions associated with sedentary lifestyle.
Remote ischaemic preconditioning (RIPC) is the exposure of the body to brief periods of circulatory occlusion and reperfusion to protect organs against ischaemic injury.4 5 Although the precise mechanisms of ischaemic conditioning are unknown, RIPC is thought to induce changes in gene expression and cellular function, including mitochondrial adaptation to metabolic stress and leucocyte activation.5 RIPC may improve metabolic efficiency by reducing cellular ATP and glycogen depletion and decreasing lactate production.6–8 RIPC may also improve skeletal muscle blood flow by inducing vasodilation through increases in nitric oxide production and the number of endothelial progenitor cells.9 Recent studies have shown that RIPC can also improve levels of exercise capacity and performance in athletes and healthy volunteers.5 10–12 The aim of this study was to evaluate the efficacy of RIPC to enhance gait in people with MS.
Materials and methods
Trial design
This study was a double-blind randomised controlled trial; the patient and the assessor were blinded to the intervention. This trial was registered with ClinicalTrials.gov.
Participants
Potential patients were identified by consultant neurologists and MS specialist nurses of a regional MS clinic at Royal Hallamshire Hospital, Sheffield, UK, from May 2017 to August 2019.
A patient information sheet was given to all potential participants deemed suitable for the trial by the treating team. Participants were given up to 2 weeks to consider their participation in the trial, and those wishing to participate were consented and screened for inclusion and exclusion criteria. Inclusion criteria comprised (1) diagnosis of MS as per 2017 revisions of McDonald’s criteria,13 (2) age 18 or older, (3) sufficient cognitive ability to give informed consent, (4) ability to walk for 6 min and (5) resting systolic BP of less than 170 mm Hg.
Patients with one or more of the following were excluded: (1) cognitive difficulties in giving consent and understanding the questionnaire, (2) inability to walk for 6 min, (3) other neurological conditions that can affect gait like stroke and Parkinson’s disease, (4) systemic illness affecting gait and exercise tolerance and (5) resting systolic BP of 170 mm Hg or more.
Interventions
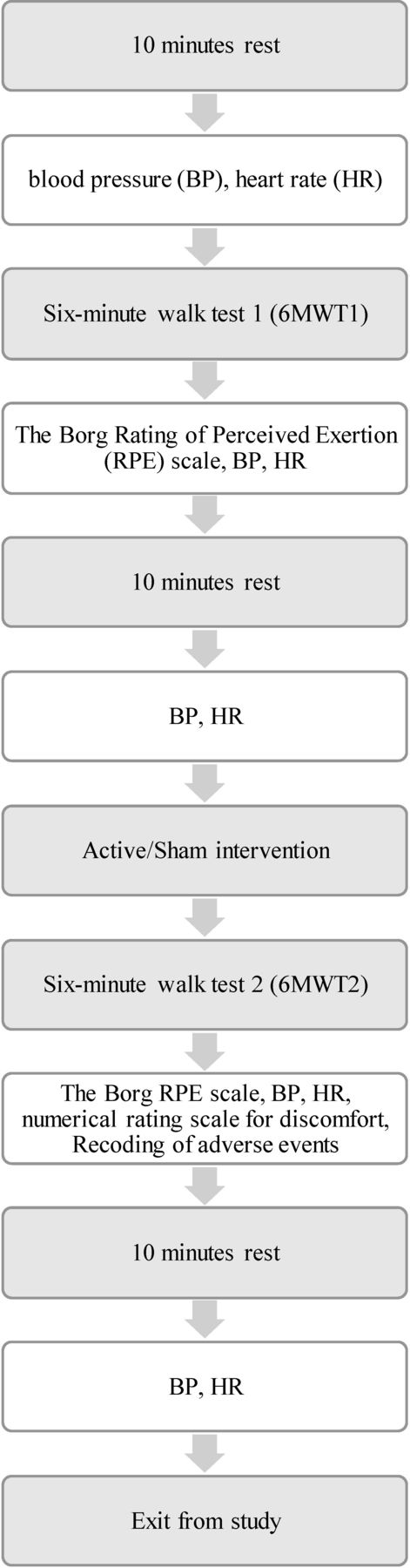
Those eligible to participate were randomised into either the intervention group (RIPC) or the control group using a random number table. The researcher performing the assessments and patients remained blind to group assignment. The study protocol is shown in figure 1. Participants rested in sitting position for 10 min. The resting blood pressure (BP) and heart rate were taken using an automatic BP monitor (Dinamap, GE). Participants were then asked to take part in the Six-Minute Walk Test (6MWT). They were asked to walk on a walkway of 14 m length back and forward for 6 min at a self-determined steady pace. Fluorescent cones were placed on both sides of the walkway to indicate where participants should turn. The total distance walked during this time was measured. Following this, BP and heart rate were measured. The patient was asked to grade the level of exertion using the Borg rate of perceived exertion (RPE) scale.14 BP and heart rate were also measured again after the patient rested for 10 min.
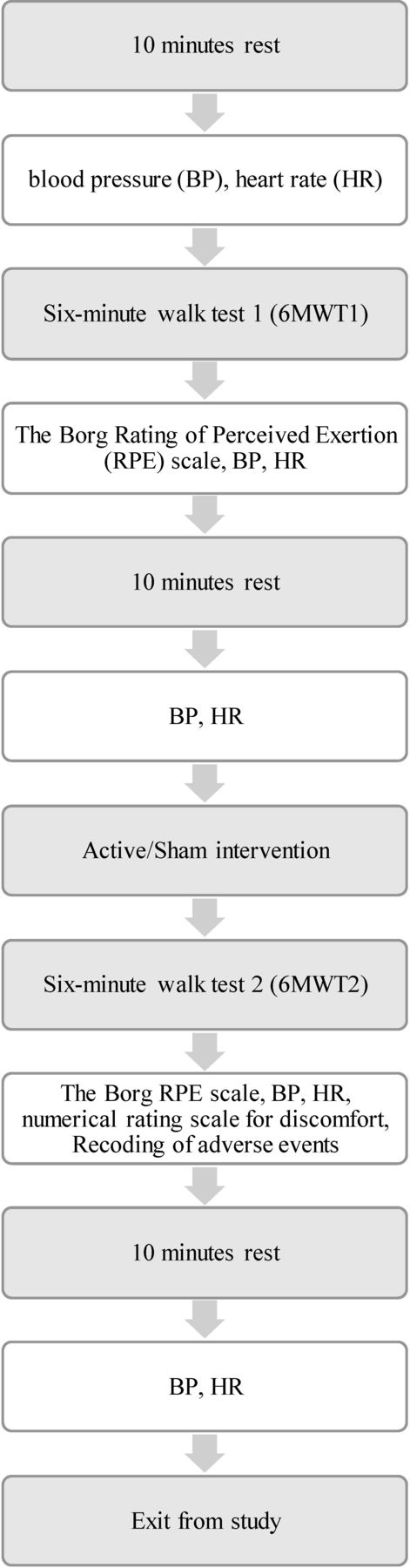
Study protocol.
The cuff of a manual BP apparatus was tied around the upper arm of the RIPC group and was inflated to the pressure 30 mm Hg above the resting systolic BP. The inflation was maintained for 5 min followed by cuff deflation lasting 5 min. The cycle was repeated three times.11
The sham intervention was delivered with the manual BP tied to the upper arm. The cuff was inflated 30 mm Hg below the diastolic BP for 5 min followed by deflation for 5 min. The cycle was repeated three times. Participants were then asked to walk for 6 min on the same 14 m walkway. Immediately after the 6 min walk, the participants were asked to rate their level of exertion using the Borg RPE scale, and BP and heart rate measurements were taken in the sitting position. Patients were asked if they experienced any discomfort using the Numerical Rating Scale (NRS) from 0 to 10. Any adverse events were also recorded. We particularly looked for redness of skin under the cuff, pain, discomfort or any sensory symptoms of the limb to which RIPC was applied. Following a 10-min rest period, BP and heart rate were measured again.
Outcomes
The primary outcome was percentage improvement in 6MWT. The 6MWT is a test of endurance.15 The absolute distance change was calculated using the formula postintervention distance–preintervention distance. The percentage improvement was calculated using the formula (postintervention distance–preintervention distance/preintervention distance)×100. The 6MWT has good reliability and is a strong indicator of exercise tolerance in patients with MS.16 17
Predefined secondary outcomes were gait speed, the Borg RPE scale, the tolerability of the RIPC and the number of people with MS who responded to RIPC. Gait speed was calculated using the formula distance walk from 6MWT (m)/time walk (s). Exertion during 6MWT was assessed before and after intervention using the Borg RPE scale, a valid and reliable tool for measuring the perceived exertion in people with MS.14 The change in exertion was calculated using the formula postintervention Borg scale–preintervention Borg scale. The tolerability of the intervention was examined using an NRS for discomfort due to intervention from 0 to 10 (0 meaning no discomfort and 10 meaning the worst discomfort possible). All adverse events experienced during the trial were recorded. We used the minimal clinically important difference (MCID) established in the literature for defining response. There are three MCIDs reported in the literature for 6MWT for people with MS. They are a relative improvement of 7% in 6MWT distance, absolute distance improvement of 9.1 m from patient perspective and 21.6 m therapist perspective in 6MWT.18 19 The number of participants who had achieved the MCID in each of these three was calculated.
The literature review showed a mean MCID for the 6MWT of 7% change.18 Our preliminary data from 22 patients showed that a sample size of 34 in each group would provide 80% power to detect an improvement of 7% after RIPC with a 0.05 two-sided significance level.
Statistical analysis
Continuous variables were reported using mean±SD for normally distributed data or median with IQRs 25 and 75 for non-normally distributed data (according to Kolmogorov-Smirnov and Shapiro-Wilk tests). Categorical variables were presented as number (percentage). Paired Student t-tests were used to examine any difference between the distances walked during 6MWT before and after the intervention within each group. Wilcoxon signed-rank tests were used to determine if there was any significant difference between the Borg’s RPE scale before and after intervention within each group. To compare quantitative data between two groups, independent t-test was used for normally distributed data, and Mann-Whitney U-test was employed to analyse for non-normally distributed data. Pearson χ2 test was used to compare the numbers of responders between groups. All statistical analyses were performed using SSPS Statistics V.18.0. A p value of <0.05 was considered to be statistically significant.
Patient and public involvement (PPI)
There were no funds or time allocated for PPI, so we were unable to involve patients. Patients were not invited to contribute to the writing or editing of this document for readability or accuracy.
Results
We approached 237 patients, of whom 77 consented to take part in the study and 75 completed the study. Of the 160 participants who chose not to participate, 13 did not meet the inclusion criteria; 102 did not give any reason; 33 reported time constraints; and 12 reported that they were not interested in this trial. The consort diagram of the study is shown on figure 2. Two of the recruited participants were excluded from analysis (one in the RIPC group due to systolic BP of >170 mm Hg and one in the sham group due to incomplete data collection).

{kind=link}
{kind=link}
Consort flow diagram. 6MWT1, Six-Minute Walk Test 1; RIPC, remote ischaemic preconditioning.
Baseline characteristics of both sham and RIPC groups are shown in table 1.
Clinical characteristics of sham and RIPC groups
Within-group comparisons before and after intervention in the sham and RIPC groups are shown in table 2.
Within-group comparisons before and after intervention
The walking distance improved by 1.9% in the sham group and by 5.7% in the RIPC group. Between-group comparisons are shown in table 3.
Comparison between sham and RIPC intervention groups
There was a statistically significant improvement in the percentage change of distance walked during 6MWT (p=0.012). The NRS for discomfort due to intervention was greater in the RIPC group compared with the sham group (p<0.001). The number of responders as defined by MCID in 6MWT is shown in table 4.
Number of patients with MCID in 6MWT after interventions
The number of responders in the RIPC group was significantly greater irrespective of the criteria for MCID used.
We did not encounter any serious adverse event and none of the patients withdrew from this study because of side effect. Adverse events of both sham and RIPC intervention groups are shown in table 5.
Adverse events of both sham intervention and RIPC intervention groups, providing number (per cent)
The common adverse events in RIPC intervention group were tingling (44.7%), redness of skin (42.1%)), pins and needles (26.3%), and skin marking (21.1%).
Discussion
This trial was the first clinical study of RIPC in patients with MS. Previous clinical studies have focused on patients suffering acute coronary events, undergoing cardiac surgery or stroke, while non-clinical studies have mainly involved performance of sports persons.10 20–22 Such studies have demonstrated the safety and tolerability of RIPC. A recent systematic review demonstrated that RIPC improved time-trial performance in 67% of athletes,10 another demonstrated improved maximal knee extensor strength after a single session of RIPC in chronic stroke.22
Cammara-Lemeroy and colleagues recently hypothesised potential mechanistic benefits of RIPC in MS.23 There are two main ways RIPC could induce neuroprotective changes: (1) via ischaemic/hypoxic mechanisms and (2) protection against inflammatory demyelination/neurodegeneration. Unpublished data from a thesis evaluating the effect of RIPC on forearm blood flow and muscle oxygen use in individuals with MS during handgrip exercise did not indicate an effect of RIPC on exercise hyperaemia24; however, the sample size was very small, with only four healthy controls and four patients with MS.
Our intervention group included 18.4% of secondary progressive multiple sclerosis (SPMS) and 10.5% of primary progressive multiple sclerosis (PPMS). The sham group, on the other hand, included lower proportions of both SPMS (2.7%) and PPMS (5.4%), reflecting in a greater level of disease severity in the intervention group (median Extended Disability Status Scale (EDSS) score of 5.0 in the RIPC group and median EDSS of 3.5 in the sham group). The beneficial effects of RIPC on gait were thus demonstrated despite greater disease severity in the intervention group.
Seventy-seven out of 237 approached patients (32.5%) were recruited for the study, a similar recruitment rate to studies randomising exercise therapy for people with MS.25
A recent systematic review and meta-analysis of the effect of functional electrical stimulation for foot drop on gait speed in MS found a statistically significant initial and ongoing orthotic effect with increase in gait speed of 0.05 and 0.08 m/s, respectively on short-walk tests (eg, 10 m and 25 ft) but no initial or ongoing effects on gait speed in long-walk tests (eg, 2 or 6 min walk).26 Our study found similar improvements in gait speed after RIPC (0.05 m/s) even after walking longer distances (6MWT). A recent study on the long-term efficacy of fampridine in gait-impaired patients with MS showed walking endurance using 6MWT improved by 11.9%, much greater than the 5.7% increment we see with single RIPC; however, we do not yet know whether longer term RIPC would result in even greater walking distances. da Mota and Marocolo highlighted that 50% of studies investigating the effect of IPC on exercise tolerance did not include an effective placebo group.27 We used a sham intervention and demonstrated that it is feasible to conduct a double-blind randomised control trial for RIPC. While no participants experienced any serious adverse events, milder side effects were more common, such as transient redness and sensory disturbances of the arm. Both interventions were tolerated; however, patients in the RIPC group graded intervention discomfort as higher (median of 4 on a Likert scale of 0–10) than the participants in the sham group (median of 1 on a Likert scale of 0–10). This was comparable to the average discomfort scores of RIPC (4/10) reported by Lalonde and Curnier in healthy individuals.28 Based on these results, we do not think a crossover design is appropriate for a clinical trial of RIPC.
Walking distances improved in the sham group (7.3 m, p=0.026). This may have been due to familiarisation with the 6MWT walkway. A longer study with multiple 6MWT may help to answer this question. The Borg RPE scale before and after intervention or sham was not significantly different; however, the sample size calculation in this study was based on 6MWT and may not have been powered to detect more subtle changes in this outcome.
Limitations
Our review of literature showed several small single-centre RIPC trials with positive outcomes in different health conditions, only for no beneficial outcome to be identified in subsequent definitive trials.20 We administered only a single cycle of RIPC in a clinical research setting and studied its immediate effect on 6MWT. As we did not study effects of multiple regular RIPC and longer term effects, we do not know whether RIPC produces any sustained benefit in people with MS. This study involved a single quaternary referral centre and recruited only patients who could walk for 6 min, limiting the generalisability of the results. We are in the process of performing a community-based study evaluating the effects of 6 weeks of daily RIPC on activity and gait.
Conclusion
This is the first clinical trial of RIPC on gait in patients with MS. A significant number of patients achieved a beneficial MCID in the primary outcome of walking distance. RIPC is a safe and well-tolerated intervention.
References
Footnotes
Contributors KPSN and CM contributed to the design of the study. KPSN was the principal investigator for the study. KPSN, CC, DH, RR, AI, JD, AA, RBL, BS, SP and DP did patient recruitment. KPSN, CC, DH, and RR did consenting and RIPC intervention. LA, EB, KPSN, CC, DH and RR did collection of outcome measures and study management. CC performed the data analysis and prepared the manuscript. KB helped with the data analysis. All authors contributed to the preparation of the final manuscript.
Funding This research was supported/funded by the National Institute for Health Research (NIHR) Sheffield Biomedical Research Centre/NIHR Sheffield Clinical Research Facility. DH and RR were supported by the University of Sheffield through student grants. CC was supported by the Mahidol University, Bangkok, Thailand. KPSN received funding from GWS Pharma and Pharma Olan for drug trials on spasticity in multiple sclerosis.
Disclaimer The views expressed are those of the author(s) and not necessarily those of the NHS, the National Institute for Health Research or the Department of Health and Social Care.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The protocol for this study was approved by the North of Scotland Research Ethics Committee (IRAS project ID: 224422).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. Anonymised data is available with the corresponding author.