Required Evidence for Clinical Applications of Liquid Biopsy Using Especially CTCs in Lung Cancer


Department of Pulmonary Diseases, University Medical Center Groningen, University of Groningen, 9713 GZ Groningen, The Netherlands
*
Author to whom correspondence should be addressed.
Appl. Sci. 2020, 10(11), 3704; https://doi.org/10.3390/app10113704
Submission received: 17 April 2020
/
Revised: 19 May 2020
/
Accepted: 20 May 2020
/
Published: 27 May 2020
(This article belongs to the Special Issue Circulating Biomarkers)
Abstract
:As therapies have become more and more dependent on tumor as well as patient characteristics, obtaining tumor material has become of great importance. Liquid biopsies hold much potential as shown by a large amount of evidence across several studies. Clinical applications for circulating tumor cells (CTCs) are unfortunately still lacking. In part this is due to a lack of studies comparing liquid biopsies to conventional diagnostics and response measurements as well as studies showing that liquid biopsies can be used to switch therapies leading to improved outcomes. However, liquid biopsies using ctDNA for specific markers such as EGFR, ALK, ROS1 or RET have clinical applications because specific drugs are available.
1. Lung Cancer
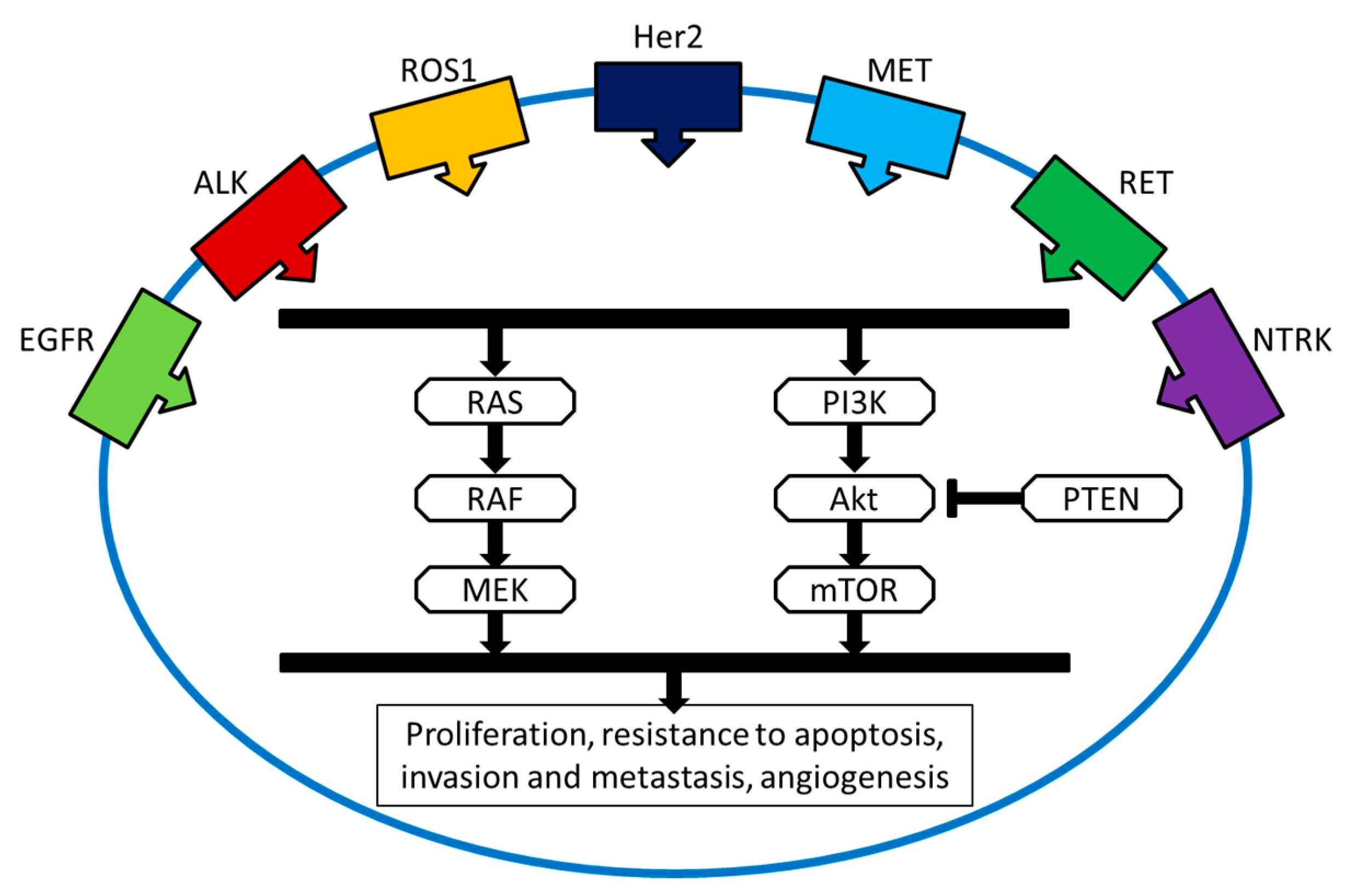
Despite novel treatment options, lung cancer still has a high mortality rate and short survival time, making it a devastating diagnosis for patients. Less than 20% will survive longer than 5 years, making it the leading cause of cancer-related death [1]. Non-small cell lung cancer (NSCLC) makes up the majority of cases, with most patients being (former) smokers. However, the number of NSCLC patients that have never smoked is increasing. These patients often only have less genomic aberrations than smokers, mostly single nucleotide mutation, rearrangements or deletions, in a tumor driver or tumor suppressor gene. These genes, such as an epidermal growth factor receptor (EGFR), are by themselves capable of driving a cell to survive and proliferate (Figure 1).
For those patients who present with advanced disease, prognosis is not only dependent on the patient but also on tumor characteristics, as these determine which treatments are effective. Chemotherapy can be given to all patients but is infamous for its side effects. In NSCLC it has limited efficacy, but is often the only option to suppress symptoms and improve the quality of life. Other therapies, i.e., targeted therapy and immunotherapy, which can have long lasting effects, have become available for NSCLC, but are only effective in a small proportion of patients. Patients with specific genomic aberrations (Figure 1), more often present in non-smoking patients, are eligible for targeted therapy [2,3,4,5]. Specific tyrosine kinase inhibitors (TKIs) provide impressive tumor responses, but not when their associated mutation is absent [4,6]. TKIs are capable of disturbing the kinase activity necessary for signal transmissions, inhibiting specific pathways and thereby tumor growth. While many tumors develop resistance within 1–2 years, many of these tumors contain secondary, resistent mutations for which also new specific TKIs are (becoming) available [4,6,7,8]. They are divided into on-target at the specific receptor and off-target resistance mechanisms, that are often unknown. Therefore, obtaining tumor biopsy material to monitor the presence of resistant mutations has become a vital part of quality care.
Immunotherapy with checkpoint inhibitors act by inhibiting an immune escape mechanism of tumor cells. The most common used therapeutics inhibit the programmed death receptor 1 and its ligand (PD-1 and PD-L1). PD-L1 restrains the immune system as a negative immune regulator and inhibits the lytic activity of effector immune cells. The inhibition of this receptor increases the recognition of tumor cells as foreign. This therapy has been recently introduced and although only 20%–25% of NSCLC patients respond to single agent immune checkpoint inhibitors, responses can last for years [9]. The presence of PD-L1 (the inhibited mechanism for immune evasion) is a major factor in determining the chance that a patient will respond, but it is not a robust predictor. Even when PD-L1 is present on the majority of tumor cells, response rates only reach 40%, while up to 10% of patients will respond to therapy when PD-L1 is not detected. Markers that can improve the prediction are therefore desperately required.
2. Tumor Tissue Obtained from Primary Tumors or Metastases
For optimal treatment decision-making, the histological classification, the presence of targetable mutations, immune cells and surface molecules (e.g., PD-L1) are important. This information is routinely obtained using formaline-fixed, paraffine-embedded tissue blocks from tumor biopsies. However, about 20%–25% of endoscopic biopsies do not provide enough tumor cells to perform molecular predictive testing or the DNA is of low quality [10]. Sometimes they do not even contain enough tumor cells for a well-established histopathological examination. Additionally, biopsies are invasive for the patient and not without complications.
3. Liquid Biopsies
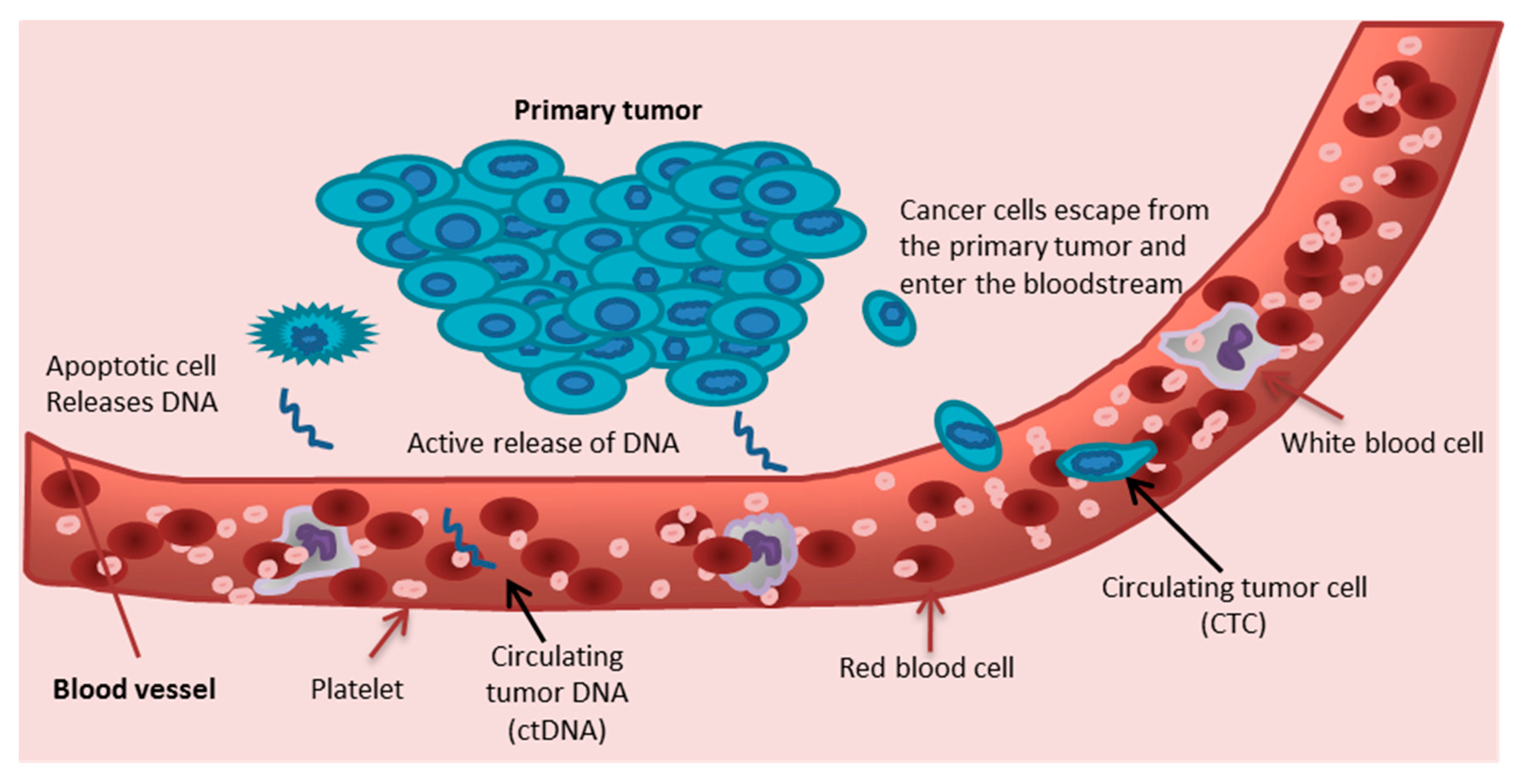
Possible alternatives for conventional biopsies are ‘liquid biopsies’, e.g., circulating tumor cells and circulating tumor DNA. As the tumor grows, tumor cells enter the bloodstream, and disseminate throughout the body (Figure 2). These so-called circulating tumor cells (CTCs) can be identified in the bloodstream by their different morphology, cell surface markers and genomic aberrations.
3.1. Circulating Tumor Cells
The predominant method of CTC detection is the CellSearch system which identifies CTCs by their expression of EpCAM and cytokeratin, while lacking CD45 [11]. In 2004 this system received FDA clearance and it is the only FDA-cleared technique to identify and enumerate CTC from a tube of blood (7.5 mL) for metastatic prostate, breast and colon carcinoma.
Not only in these malignancies but also in lung cancer, the number of CTCs is predictive for a shorter progression-free and overall survival [12,13,14]. CTC persistence after treatment is associated with therapy failure for many malignancies [12,15,16,17,18,19,20,21,22,23]. In fact, their counts and change after therapy are stronger correlated with survival than response evaluation by computed tomography (CT) in metastatic breast cancer patients [12,14,15]. In addition, several morphological changes in CTCs have been associated with chemotherapy resistance [23,24,25,26]. Moreover, in small cell lung cancer, genomic analysis (assessment of copy number anomalies (can)) of CTCs may be used to predict response to chemotherapy [27]. Driver mutations and PD-L1 expression can be detected in and on CTCs (therapeutic marker) [28,29,30,31,32].
However, while CTCs are a clear prognostic factor in NSCLC, it is a weak or not a predictor for tumor response at all (Table 1) [17,29,33,34,35,36]. Moreover, their clinical application is limited by the low detection rate [35]. Even in advanced stage NSCLC, CTCs are only detected in 30% of patients and in almost all cases in low numbers per 7.5 mL of peripheral blood (Table 1). Other limitations are the standardization of CTC isolation or enrichment, the laborious and time-consuming process of isolating CTCs, being less flexible than applying tests for the determination of circulating DNA.
When CTCs are captured in sufficient numbers, the heterogeneity of tumors can be studied by analyzing these cells at an individual cell level. They could be used to study tumor development and evolution. Unlike conventional biopsies, which can only contain tumor material from one location, CTCs probably represent the most relevant tumor cells in the body [37]. Another advantage of CTCs as compared with tumor biopsies is that they can be measured sequentially to assess tumor activity under therapy as they can be obtained in a minimally invasive manner [38].
3.2. Circulating Cell-Free DNA
Besides CTC, DNA also circulates in the bloodstream, either by active secretion or as a waste product from decaying or apoptotic cells [50]. In the bloodstream, circulating cell-free DNA (cfDNA) from healthy body cells is mixed with small amounts of circulating tumor DNA (ctDNA). Recently, sensitive next-generation sequencing methods have been developed that are able to accurately measure low mutant allele frequencies in plasma [51]. This development makes single-gene tests obsolete, though digital droplet PCR may still be usable for the detection of minimal residual disease in patients with known mutations. Mutations in DNA detected in the plasma show a strong correlation with the presence of mutations in the primary tumor [31,51]. When e.g., EGFR, ALK, BRAF, ROS1, RET aberrations are detected in plasma, this information can be used for treatment decision without the need for a tumor biopsy [32,52]. When the mutation is present in the plasma sample, the outcome is almost similar compared to those measured in biopsies. The role of ctDNA and immune-related mechanisms is evolving as a tumor mutational burden and genes related to immune resistance such as STK11 and KEAP1 which can be measured from plasma ctDNA.
4. Required Steps before Clinical Implementation Can Be Considered
While some may already be convinced that CTCs and ctDNA are ready for clinical application, many physicians are hesitant. Studies that compare CTCs and ctDNA with conventional methods are few [12,13,14]. Most studies are relatively small and often from a single center. Large, prospective multicenter comparative trials are lacking. Secondly, standard operating procedures for collecting and analyzing samples differ between centers. Thirdly, none have ever tested whether CTCs and ctDNA can actually be used to change clinical decisions. If we consider plasma ctDNA, however, there are many studies that prove the value of targeted next-generation sequencing for genes that are targetable with specific tyrosine kinase inhibitors [32,52]. These are already implemented in clinical practice. ctDNA can also be used to assess the presence of minimal residual disease (MRD), as in hematology. For hematology it has been shown that early interventions increase survival when based on MRD, indicating a monitoring role for cfDNA.
ctDNA tests are predictive, while CTCs are mainly prognostic. Therefore, physicians will refuse to implement liquid biopsies for CTCs. Only in a few malignancies have studies shown that CTCs can predict whether patients will not benefit from therapies [36,53,54,55,56,57]. Unfortunately, it is still unknown whether a switch to therapies should be implemented and would lead to a better outcome.
Another option for CTCs could be as a replacement for conventional biopsies (diagnosis) but in NSCLC CTCs are simply too rare, unless larger volumes of blood can be screened. Single-cell next generation sequencing may determine the specific DNA or even RNA aberrations that may have a clinical impact. These technologies are evolving but are not ready for the clinic.
All in all, liquid biopsies are used for ctDNA that finds its application in the clinic for targeted therapies, and for CTCs mainly as a prognostic biomarker.
Author Contributions
Writing/review/editing: M.T. & H.J.M.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Siegel, R.L.; Mioller, K.D.; Jemal, A. Cancer statistics 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collisson, E.A.; Campbell, J.D.; Brooks, A.N.; Berger, A.H.; Lee, W.; Chmielecki, J.; Beer, D.G.; Cope, L.; Creighton, C.J.; Danilova, L.; et al. Comprehensive molecular profiling of lung adenocarcinoma. Nature 2014, 511, 543–550. [Google Scholar]
- Hammerman, P.S.; Lawrence, M.S.; Voet, D.; Jing, R.; Cibulskis, K.; Sivachenko, A.; Stojanov, P.; McKenna, A.; Lander, E.S.; Gabriel, S.; et al. Comprehensive genomic characterization of squamous cell lung cancers. Nature 2012, 489, 519–525. [Google Scholar]
- Mok, T.S.; Wu, Y.L.; Ahn, M.J.; Garassino, M.C.; Kim, H.R.; Ramalingam, S.S.; Shepherd, F.A.; He, Y.; Akamatsu, H.; Theelen, W.S.M.E.; et al. Osimertinib or Platinum–Pemetrexed in EGFR T790M–Positive Lung Cancer. N. Engl. J. Med. 2017, 376, 629–640. [Google Scholar] [CrossRef] [Green Version]
- Solomon, B.J.; Mok, T.; Kim, D.W.; Kim, D.W.; Wu, Y.L.; Akagawa, K.; Mekhail, T.; Felip, E.; Capuzzo, F. First-Line Crizotinib versus Chemotherapy in ALK -Positive Lung Cancer. N. Engl. J. Med. 2014, 371, 2167–2177. [Google Scholar] [CrossRef] [Green Version]
- Mok, T.; Wu, Y.L.; Lee, J.S.; Yu, C.j.; Sriuranpong, V.; Sandoval-Tan, J.; Ladrera, G.; Thongprasert, S.; Srimuninnimit, V.; Liao, M.; et al. Detection and dynamic changes of EGFR mutations from circulating tumor DNA as a predictor of survival outcomes in NSCLC Patients treated with first-line intercalated erlotinib and chemotherapy. Clin. Cancer Res. 2015, 21, 3196–3203. [Google Scholar] [CrossRef] [Green Version]
- Gainor, J.F.; Dardaei, L.; Yoda, S.; Friboulet, L.; Leshchiner, I.; Katayama, R.; Dagogo-Jack, I.; Gadgeel, S.; Schulz, K.; Sing, M.; et al. Molecular mechanisms of resistance to first- and second- generation alk inhibitors in ALK-rearranged lung cancer. Cancer Discov. 2016, 6, 1118–1133. [Google Scholar] [CrossRef] [Green Version]
- Sequist, L.V.; Waltman, B.A.; Dias-Santagata, D.; Digumarthy, S.; Turke, A.B.; Fidias, P.; Bergethon, K.; Shaw, A.T.; Gettinger, S.; Cosper, A.; et al. Genotypic and histological evolution of lung cancers acquiring resistance to EGFR inhibitors. Sci. Transl. Med. 2011, 3, 75ra26. [Google Scholar] [CrossRef] [Green Version]
- Horn, L.; Spigel, D.R.; Vokes, E.E.; Holgado, E.; Ready, N.; Steins, M.; Poddubskaya, E.; Borghaei, H.; Felip, E.; Paz-Ares, L.; et al. Nivolumab versus docetaxel in previously treated patients with advanced non–small-cell lung cancer: Two-year outcomes from two randomized, open-label, phase III trials (ChecKmate 017 and CheckMate 057). J. Clin. Oncol. 2017, 35, 3924–3933. [Google Scholar] [CrossRef]
- Kerner, G.S.M.; Schuuring, E.; Sietsma, J.; Hiltermann, T.j.N.; Pieterman, R.M.; De Leede, G.P.J.; Van Putten, J.W.G.; Liesker, J.; Renkema, T.E.J.; Van Henge, P.; et al. Common and rare EGFR and KRAS mutations in a Dutch non-small-cell lung cancer population and their clinical outcome. PLoS ONE 2013, 8, e70346. [Google Scholar] [CrossRef] [Green Version]
- Cristofanilli, M.; Budd, T.; Ellis, M.J.; Stopeck, A.; Matera, J.; Miller, C.; Reuben, J.M.; Doyle, G.V.; Allard, J.; Terstappen, L.W.M.M.; et al. Circulating tumor cells, disease progression, and survival in metastatic breast cancer. N. Engl. J. Med. 2004, 351, 781–791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coumans, F.A.W.; Ligthart, S.T.; Uhr, J.W.; Terstappen, L.W. Challenges in the enumeration and phenotyping of CTC. Clin. Cancer Res. 2012, 18, 5711–5718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coumans, F.A.W.; Ligthart, S.T.; Terstappen, L.W.M.M. Interpretation of changes in circulating tumor cell counts. Transl. Oncol. 2012, 5, 486–491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Giorgi, U.; Valero, V.; Rohren, E.; Mego, M.; Doyle, G.V.; Miller, M.C.; Ueno, N.T.; Handy, B.C.; Reuben, J.M.; Macapinlac, H.A.; et al. Circulating tumor cells and bone metastases as detected by FDG-PET/CT in patients with metastatic breast cancer. Ann. Oncol. 2010, 21, 33–39. [Google Scholar] [CrossRef]
- Budd, G.T.; Cristofanilli, M.; Ellis, M.J.; Stopeck, A.; Borden, E.; Miller, M.C.; Matera, J.; Repollet, M.; Doyle, G.V.; Terstappen, L.W.M.M.; et al. Circulating tumor cells versus imaging—Predicting overall survival in metastatic breast cancer. Clin. Cancer Res. 2006, 12, 6403–6409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, M.C.; Shields, P.G.; Warren, R.D.; Cohen, P.; Wilkinson, M.; Ottaviano, Y.L.; Rao, S.B.; Eng-Wong, J.; Seillier-Moiseiwitsch, F.; Noone, A.M.; et al. Circulating tumor cells: A useful predictor of treatment efficacy in metastatic breast cancer. J. Clin. Oncol. 2009, 27, 5153–5159. [Google Scholar] [CrossRef] [Green Version]
- Messaritakis, I.; Politaki, E.; Koinis, F.; Stoltidis, D.; Apostolaki, S.; Plataki, M.; Dermitzaki, E.K.; Georgoulias, V.; Kotsakis, A. Dynamic changes of phenotypically different circulating tumor cells sub-populations in patients with recurrent/refractory small cell lung cancer treated with pazopanib. Sci. Rep. 2018, 8, 2238. [Google Scholar] [CrossRef] [Green Version]
- Krebs, M.G.; Sloane, R.; Priest, L.; Lee, L.; Hou, J.M.; Mei, J.; Alastair, G.; Ward, T.H.; Ferraldeschi, R.; Hughes, A.; et al. Evaluation and prognostic significance of circulating tumor cells in patients with non-small-cell lung cancer. J. Clin. Oncol. 2011, 29, 1556–1563. [Google Scholar] [CrossRef]
- Punnoose, E.A.; Atwal, S.; Liu, W.; Raja, R.; Fine, B.M.; Hughes, B.G.M.; Hicks, R.J.; Hampton, G.M.; Amler, L.C.; Pirzkall, A.; et al. Evaluation of circulating tumor cells and circulating tumor DNA in non-small cell lung cancer: Association with clinical endpoints in a phase II clinical trial of pertuzumab and erlotinib. Clin. Cancer Res. 2012, 18, 2391–2401. [Google Scholar] [CrossRef] [Green Version]
- Nicolazzo, C.; Raimondi, C.; Mancini, M.; Caponnetto, S.; Gradilone, A.; Gandini, O.; Mastromartino, M.; Del Bene, G.; Prete, A.; Longo, F.; et al. Monitoring PD-L1 positive circulating tumor cells in non-small cell lung cancer patients treated with the PD-1 inhibitor Nivolumab. Sci. Rep. 2016, 6, 317726. [Google Scholar] [CrossRef]
- Aggarwal, C.; Wang, X.; Ranganathan, A.; Torigian, D.; Troxel, A.; Evans, T.; Cohen, R.B.; Vaidya, B.; Rao, C.; Connelly, M.; et al. Circulating tumor cells as a predictive biomarker in patients with small cell lung cancer undergoing chemotherapy. Lung Cancer 2017, 112, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Stebbing, J.; Payne, R.; Reise, J.; Frampton, A.E.; Avery, M.; Woodley, L.; Di Leo, A.; Perstrin, M.; Krell, J.; Coombes, R.C. The efficacy of lapatinib in metastatic breast cancer with HER2 non-amplified primary tumors and EGFR positive circulating tumor cells: A proof-of-concept study. PLoS ONE 2013, 8. [Google Scholar] [CrossRef] [Green Version]
- Cohen, S.J.; Punt, C.J.A.; Iannotti, N.; Cohen, S.J.; Punt, C.J.A.; Iannotti, N.; Saidman, B.H.; Sabbath, K.D.; Gabrail, N.Y.; Picus, J.; et al. Relationship of circulating tumor cells to tumor response, progression-free survival, and overall survival in patients with metastatic colorectal cancer. J. Clin. Oncol. 2008, 26, 3213–3221. [Google Scholar] [CrossRef]
- Papadaki, M.A.; Stoupis, G.; Theodoropoulos, P.A.; Mavroudig, D.; Georgoulias, V.; Agelaki, S. Circulating tumor cells with stemness and epithelial-to-mesenchymal transition features are chemoresistant and predictive of poor outcome in metastatic breast cancer. Mol. Cancer Ther. 2019, 18, 437–447. [Google Scholar] [CrossRef] [Green Version]
- Hou, J.M.; Krebs, M.G.; Lancashire, L.; Sloane, R.; Backen, A.; Swain, R.K.; Priest, L.J.C.; Greystoke, A.; Zhou, C.; Morris, K.; et al. Clinical significance and molecular characteristics of circulating tumor cells and circulating tumor microemboli in patients with small-cell lung cancer. J. Clin. Oncol. 2012, 30, 525–532. [Google Scholar] [CrossRef] [PubMed]
- Hou, J.M.; Greystoke, A.; Lancashire, L.; Cummings, J.; Ward, T.; Board, R.; Amir, E.; Hughes, S.; Krebs, M.; Hughes, A.; et al. Evaluation of circulating tumor cells and serological cell death biomarkers in small cell lung cancer patients undergoing chemotherapy. Am. J. Pathol. 2009, 175, 808–816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carter, L.; Rothwell, D.G.; Mesquita, B.; Smowton, C.; Leong, H.S.; Fernandez-Gutierrez, F.F.; Li, Y.; Burt, D.J.; Antonello, J.; Morrow, C.J.; et al. Molecular analysis of circulating tumor cells identifies distinct copy-number profiles in patients with chemosensitive and chemorefractory small-cell lung cancer. Nat. Med. 2016, 23, 114–119. [Google Scholar] [CrossRef]
- Ilie, M.; Long, E.; Butori, C.; Hofman, V.; Coelle, C.; Mauro, V.; Zahaf, K.; Marquette, C.H.; Mouroux, J.; Paterlini-Bechot, P.; et al. ALK-gene rearrangement: A comparative analysis on circulating tumour cells and tumour tissue from patients with lung adenocarcinoma. Ann. Oncol. 2012, 23, 2907–2913. [Google Scholar] [CrossRef] [PubMed]
- Ilié, M.; Szafer-Glusman, E.; Hofman, V.; Chamorey, E.; Lalvée, S.; Selva, E.; Leroy, S.; Marquette, C.H.; Kowanetz, M.; Hedge, P.; et al. Detection of PD-L1 in circulating tumor cells and white blood cells from patients with advanced non-small-cell lung cancer. Ann. Oncol. 2018, 29, 193–199. [Google Scholar]
- Hofman, V.; Ilie, M.; Long-Mira, E.; Hofman, V.; Ilie, M.; Long-Mira, E.; Giacchero, D.; Butori, C.; Dadone, B.; Selva, E.; et al. Usefulness of immunocytochemistry for the detection of the BRAF(V600E) mutation in circulating tumor cells from metastatic melanoma patients. J. Investig. Dermatol. 2013, 133, 1378–1381. [Google Scholar] [CrossRef] [Green Version]
- Maheswaran, S.; Sequist, L.V.; Sunitha, N.; Ulkus, L.; Brannigan, B.; Collura, C.V.; Inserra, E.; Sven, D.; Iafrate, A.J.; Bell, D.W.; et al. Detection of mutations in EGFR in circulating lung-cancer cells. N. Engl. J. Med. 2008, 359, 366–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sundaresan, T.K.; Sequist, L.V.; Heymach, J.V.; Riely, G.J.; Janne, P.A.; Koch, W.H.; Sullivan, J.P.; Fox, D.B.; Maher, R.; Muzikansky, A.; et al. Detection of T790M, the acquired resistance EGFR mutation, by tumor biopsy versus noninvasive blood-based analyses. Clin. Cancer Res. 2016, 22, 1103–1110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hofman, V.; Long, E.; Ilie, M.; Bonnetaud, C.; Vignaud, J.M.; Flejou, J.F.; Lantuejoul, S.; Piaton, E.; Mourad, N.; Butori, C.; et al. Morphological analysis of circulating tumour cells in patients undergoing surgery for non-small cell lung carcinoma using the isolation by size of epithelial tumour cell (ISET) method. Cytopathology 2012, 23, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Krebs, M.G.; Hou, J.M.; Sloane, R.; Lancashire, L.; Priest, L.; Nonaka, D.; Ward, T.H.; Backen, A.; Clack, G.; Hughes, A.; et al. Analysis of circulating tumor cells in patients with non-small cell lung cancer using epithelial marker-dependent and -independent approaches. J. Thorac. Oncol. 2012, 7, 306–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tamminga, M.; De Wit, S.; Hiltermann, T.J.N.; Timens, W.; Schuuring, E.; Terstappen, L.W.M.M.; Groen, H.J.M. Circulating tumor cells in advanced non- small cell lung cancer patients are associated with worse tumor response to checkpoint inhibitors. J. Immunother. Cancer 2019, 7, 173. [Google Scholar] [CrossRef] [PubMed]
- Tamminga, M.; De Wit, S.; Schuuring, E.; Timens, W.; Terstappen, L.W.M.M.; Hiltermann, T.J.N.H.; Groen, H.J.M. Circulating tumor cells in lung cancer are prognostic and predictive for worse tumor response in both targeted- and chemotherapy. Transl. Lung Cancer Res. 2019, 8, 854–861. [Google Scholar] [CrossRef]
- Hanssen, A.; Loges, S.; Pantel, K.; Wikman, H. Detection of Circulating Tumor Cells in Non-Small Cell Lung Cancer. Front. Oncol. 2015, 5, 207. [Google Scholar] [CrossRef]
- Heitzer, E.; Haque, I.S.; Roberts, C.E.S.; Speicher, M.R. Current and future perspectives of liquid biopsies in genomics-driven oncology. Nat. Rev. Genet. 2019, 20, 71–88. [Google Scholar] [CrossRef]
- Hofman, V.; Ilie, M.I.; Long, E.; Selva, E.; Bonnetaud, C.; Molina, T.; Vénissac, N.; Mouroux, J.; Vielh, P.; Hofman, P. Detection of circulating tumor cells as a prognostic factor in patients undergoing radical surgery for non-small-cell lung carcinoma: Comparison of the efficacy of the CellSearch AssayTM and the isolation by size of epithelial tumor cell method. Int. J. Cancer 2010, 129, 1651–1660. [Google Scholar] [CrossRef]
- Lou, J.; Ben, S.; Yang, G.; Liang, X.; Wang, X.; Ni, S.; Han, B. Quantification of rare circulating tumor cells in non-small cell lung cancer by ligand-targeted PCR. PLoS ONE 2013, 8, e80458. [Google Scholar] [CrossRef] [Green Version]
- Nieva, J.; Wendel, M.; Luttgen, M. High-definition imaging of circulating tumor cells and associated cellular events in non-small cell lung cancer patients: A longitudinal analysis. Phys. Biol. 2012, 9, 016004. [Google Scholar] [CrossRef] [Green Version]
- Wendel, M.; Bazhenova, L.; Boshuizen, R.; Kolatkar, A.; Thistlethwaite, P.; Bethel, K.; Nieve, J.; Van den Heuvel, M. Fluid biopsy for Circulating Tumor Cell identification in Patients with early and late stage Non-Small Cell Lung Cancer: A glimpse into lung cancer biology. Phys. Biol. 2013, 9, 016005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, Y.; Chen, Z.; Dong, J.; Wie, P.; Hu, R.; Zhou, C.; Sun, N.; Luo, M.; Yang, W.; Yao, R.; et al. Folate receptor-positive circulating tumor cells as a novel diagnostic biomarker in non-small cell lung cancer. Transl. Oncol. 2013, 6, 697–702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juan, O.; Vidal, J.; Gisbert, R.; Muñoz, J.; Maciá, S.; Gómez-Codina, J. Prognostic significance of circulating tumor cells in advanced non-small cell lung cancer patients treated with docetaxel and gemcitabine. Clin. Transl. Oncol. 2014, 16, 637–643. [Google Scholar] [CrossRef] [PubMed]
- Muinelo-Romay, L.; Vieito, M.; Abalo, A.; Nocelo, M.A.; Barón, F.; Anido, U.; Brozos, E.; Vazquez, F.; Aquín, A.; Abal, M.; et al. Evaluation of circulating tumor cells and related events as prognostic factors and surrogate biomarkers in advanced NSCLC patients receiving first-line systemic treatment. Cancers 2014, 6, 153–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, X.; Zhou, F.; Li, X.; Yang, G.; Zhang, L.; Ren, S.; Zhao, C.; Deng, Q.; Li, W.; Gao, G.; et al. Folate receptor–positive circulating tumor cell detected by LT-PCR–based method as a diagnostic biomarker for non–small-cell lung cancer. J. Thorac. Oncol. 2015, 10, 1163–1171. [Google Scholar] [CrossRef] [Green Version]
- Wan, J.W.; Gao, M.Z.; Hu, R.J.; Huang, H.Y.; Wei, Y.Y.; Han, Z.J.; Yan, Z.H. A preliminary study on the relationship between circulating tumor cells count and clinical features in patients with non-small cell lung cancer. Ann. Transl. Med. 2015, 35, 6–10. [Google Scholar]
- De Wit, S.; Van Dalum, G.; Lenferink, A.T.M.; Tibbe, A.G.J.; Hiltermann, T.J.N.; Groen, H.J.M.; Van Rijn, C.J.M.; Terstappen, L.W.M.M. The detection of EpCAM+ and EpCAM–circulating tumor cells. Sci. Rep. 2015, 5, 12270. [Google Scholar] [CrossRef] [Green Version]
- Tamminga, M.; Groen, H.J.M.; Hiltermann, T.J.N. Investigating CTCs in NSCLC-a reaction to the study of Jia-Wei Wan: A preliminary study on the relationship between circulating tumor cells count and clinical features in patients with non-small cell lung cancer. J. Thorac. Dis. 2016, 8, 1032–1036. [Google Scholar] [CrossRef] [Green Version]
- Williamson, R. Properties of rapidly labelled deoxyribonucleic acid fragments isolated from the cytoplasm of primary cultures of embryonic mouse liver cells. J. Mol. Biol. 1970, 51, 157–168. [Google Scholar] [CrossRef]
- Newman, A.M.; Bratman, S.V.; To, J.; Wynne, J.F.; Eclov, N.C.W.; Modlin, L.A.; Liu, C.L.; Neal, J.W.; Wakalee, H.A.; MEritt, R.E.; et al. An ultrasensitive method for quantitaing circulating tumor DNA with braod patient coverage. Nat. Med. 2014, 20, 548–554. [Google Scholar] [CrossRef] [PubMed]
- Oxnard, G.R.; Thress, K.S.; Alden, R.S.; Lawrance, R.; Paweletz, C.P.; Cantarini, M.; Yang, J.C.H.; Barrett, J.C.; Jänne, P.A. Association between plasma genotyping and outcomes of treatment with osimertinib (AZD9291) in advanced non-small-cell lung cancer. J. Clin. Oncol. 2016, 34, 3375–3382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trapp, E.; Janni, W.; Schindlbeck, C.; Jückstock, J.; Andergassen, U.; De Gregorio, A.; Alunni-Fabbroni, M.; Tzschaschel, M.; Polasik, A.; Koch, J.G.; et al. Presence of circulating tumor cells in high-risk early breast cancer during follow-up and prognosis. J. Natl. Cancer Inst. 2019, 111, 380–387. [Google Scholar] [CrossRef]
- Janning, M.; Kobus, F.; Babayan, A.; Wikman, H.; Velthaus, J.; Bergmann, S.; Schatz, S.; Falk, M.; Berger, L.; Böttcher, L.; et al. Determination of PD-L1 expression in circulating tumor cells of NSCLC patients and correlation with response to PD-1/PD-L1 inhibitors. Cancers 2019, 11, 835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schramm, A.; Schochter, F.; Friedl, T.W.P.; de Gregorio, N.; Andergassen, U.; Alunni-Fabbroni, M.; Trapp, E.; Jaeger, B.; Heinrich, G.; Camara, O.; et al. Prevalence of circulating tumor cells after adjuvant chemotherapy with or without anthracyclines in patients With HER2-negative, hormone receptor-positive early breast cancer. Clin. Breast Cancer 2017, 17, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Bauer, E.C.A.; Schochter, F.; Widschwendter, P.; DeGregorio, A.; Andergassen, U.; Friedl, T.W.P.; Fasching, P.A.; Fehm, T.; Schneeweiss, A.; Beckmann, M.; et al. Prevalence of circulating tumor cells in early breast cancer patients 2 and 5 years after adjuvant treatment. Breast Cancer Res. Treat. 2018, 171, 571–580. [Google Scholar] [CrossRef] [PubMed]
- Garrel, R.; Mazel, M.; Perriard, F.; Vinches, M.; Cayrefourcq, L.; Guigay, J.; Digue, L.; Aubry, K.; Alfonsi, M.; Delord, J.P.; et al. Circulating tumor cells as a prognostic factor in recurrent or metastatic head and neck squamous cell carcinoma: The circutec prospective study. Clin. Chem. 2019, 65, 1267–1275. [Google Scholar] [CrossRef]
Figure 1.
Targetable genes and main pathways that lead to cellular proliferation.

Figure 2.
Different mechanisms that lead to the release of tumor cells and tumor DNA from the primary tumor into the blood stream. Circulating tumor cells (CTC) and circulating tumor DNA (ctDNA) can then be obtained by a normal blood draw.
Figure 2.
Different mechanisms that lead to the release of tumor cells and tumor DNA from the primary tumor into the blood stream. Circulating tumor cells (CTC) and circulating tumor DNA (ctDNA) can then be obtained by a normal blood draw.


{kind=link}
{kind=link}
Table 1.
Circulating tumor cells in non-small cell lung cancer (NSCLC) by different filtration techniques and the outcome.
Table 1.
Circulating tumor cells in non-small cell lung cancer (NSCLC) by different filtration techniques and the outcome.
| Author (Year) | Measurement Method | Population | Outcome |
| Hofman (2011) [39] | Cellsearch and ISET § | 210 NSCLC patients undergoing surgery, stage I–IV | Cellsearch (≥1 CTC): 82/210 positive (39%) ISET (≥1 CTC): 104/210 positive (50%) Both methods independently associated with diminished DFS |
| Krebbs (2011) [17] | Cellsearch | 101 NSCLC patients untreated stage III/IV, samples before and after treatment | ≥2 CTCs: 21 patients (21%) CTCs ≥5 CTCs baseline and treatment CTCs correlated with OS *, PFS * and disease stage. |
| Krebbs (2012) [34] | Cellsearch and ISET | 40 patients stage III/IV, paired blood samples for comparison | Cellsearch (≥2 CTC): 9/40 positive (23%) ISET (>1 CTC): 32/40 positive (80%) ISET: additionally, CTC clusters and subpopulation of EpCAM-CTCs ∆ |
| Punnoose (2012) [18] | Cellsearch method | 41 NSCLC patients, stage III/IV Treated with erlotinib and pertuzumab | ≥1 CTC: 28/37 positive (78%) CTC count decrease correlated with DFS |
| Lou (2013) [40] | LT-PCR + (folate α-receptors) | 72 NSCLC patients, stage I–IV 20 benign patients 24 healthy donors | Threshold 8.5 CTU †: detection of NSCLC: sensitivity 82%; specificity 93% |
| Nieva (2013) [41] | HD-CTC IF # | 28 NSCLC patients with metastatic disease, 66 blood samples during course study | ≥1 CTC per mL: 45 out of 66 (68%) blood samples CTCs ≥5 per mL a HR * OS 4.0. |
| Wendel (2013) [42] | HD-CTC | 78 NSCLC patients, chemotherapy-naïve, stage I–IV | ≥1 CTCs per 1 mL: 57/78 (73%) No correlation disease stage |
| Yue Yu (2013) [43] | LT-PCR (folate α-receptors) | 153 NSCLC patients, stage I–IV, 64 benign disease, 49 healthy controls | Threshold 8.64 CTU: detection of NSCLC: sensitivity 73%; specificity 84% |
| Juan (2014) [44] | Cellsearch | 37 NSCLC patients, stage IIIB/IV, measurements at baseline and after 2 months chemotherapy | ≥ 2 CTCs: 9/37 positive (24%) ≥ 1 CTCs: 15/39 (%) |
| Muinelo-Romoy (2014) [45] | Cellsearch | 43 NSCLC patients, stage IIIB or IV and undergoing first line chemotherapy | ≥1 CTCs: 18/43 positive (42%) ≥5 CTCs: 10/43 positive (23%) ≥5 CTCs correlated with OS and PFS |
| Chen (2015) [46] | LT-PCR (folate α-receptors) | Validation set: 237 NSCLC patients, stage I–IV 114 benign patients, 28 controls | Threshold 8.93 CTU: sensitivity of 76%; specificity 82% Correlated with disease stage |
| Wan (2015) [47] | LT-PCR (folate α-receptors) | 50 NSCLC patients, stage I–IV 35 benign patients, 28 healthy subjects | CTU correlated to disease stage |
| Wit (2015) [48] | Modified Cellsearch (+EPCAM- CTCs) | 27 patients (24 NSCLC patients) | ≥1 EpCAM+ CTC: 11/27 (41%) ≥5: 4/27 (15%) ≥1 EpCAM- or EpCAM+ CTCs: 20/27 (74%) ≥5: 11/27 (41%) EpCAM + cells ≥1 correlated with OS EpCAM- cells no significant difference in OS |
All CTC numbers are in 7.5 mL of whole blood, unless stated otherwise. *: OS: overall survival, PFS: progression-free survival, DFS: disease-free survival, HR: hazard ratio. §: ISET: isolation by size of epithelial tumor. ∆: EpCAM- CTCs: epithelial cell adhesion molecule negative circulating tumor cells. #: HD-CTC IF: high definition-CTC immunofluorescence. +: LT-PCR: ligand-targeted PCR. † CTU: circulating tumor cell unit (designation of amount of CTCs per 3 mL blood by Yu Y. and Chen X.). Adapted from Tamminga et al., Journal of thoracic disease 2019 [49].
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Tamminga, M.; Groen, H.J.M. Required Evidence for Clinical Applications of Liquid Biopsy Using Especially CTCs in Lung Cancer. Appl. Sci. 2020, 10, 3704. https://doi.org/10.3390/app10113704
AMA Style
Tamminga M, Groen HJM. Required Evidence for Clinical Applications of Liquid Biopsy Using Especially CTCs in Lung Cancer. Applied Sciences. 2020; 10(11):3704. https://doi.org/10.3390/app10113704
Chicago/Turabian StyleTamminga, Menno, and Harry J.M. Groen. 2020. "Required Evidence for Clinical Applications of Liquid Biopsy Using Especially CTCs in Lung Cancer" Applied Sciences 10, no. 11: 3704. https://doi.org/10.3390/app10113704
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.