Risk for Irritable Bowel Syndrome in Patients with Helicobacter Pylori Infection: A Nationwide Population-Based Study Cohort Study in Taiwan

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
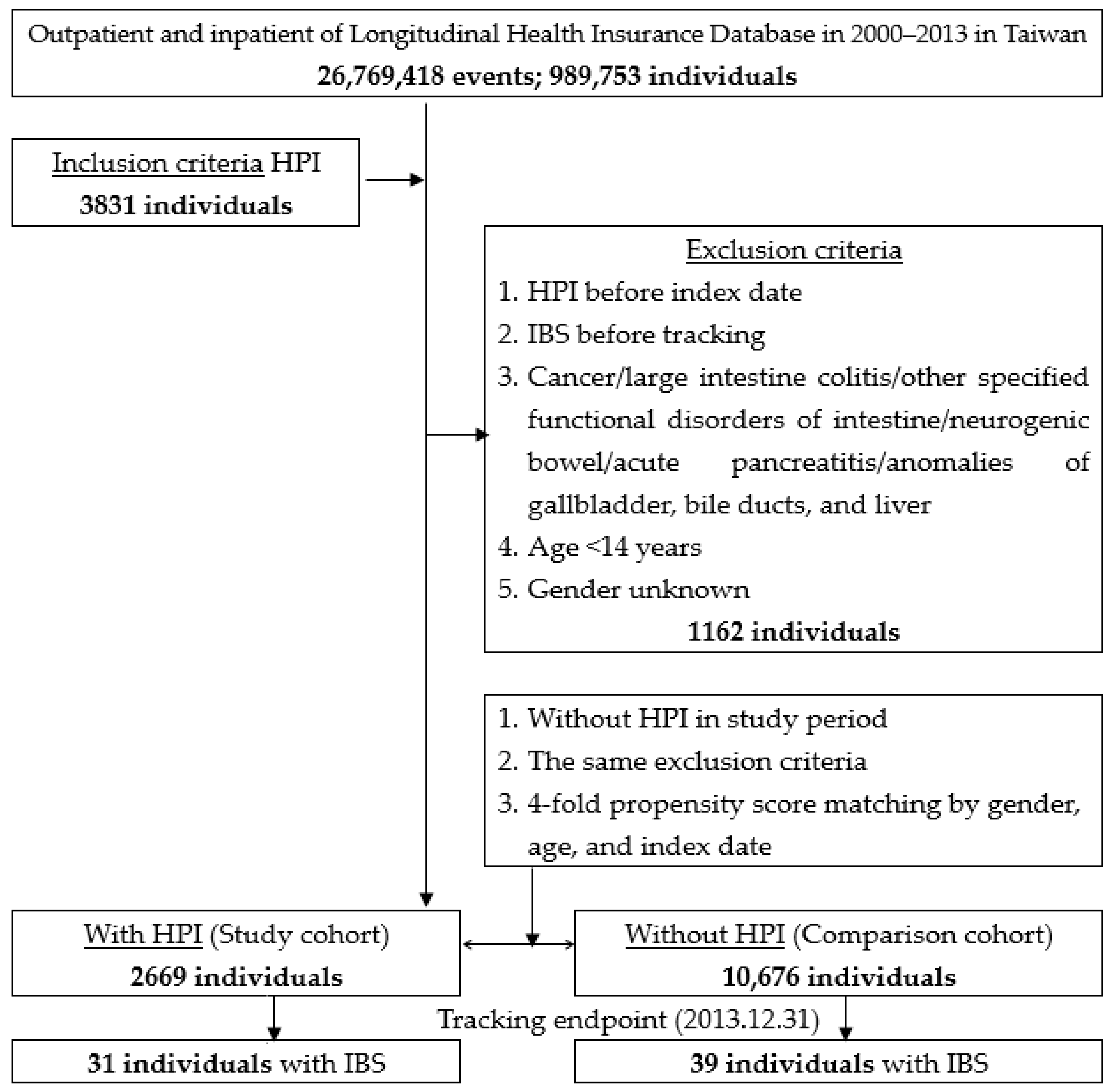
2.2. Sample Participants
2.3. Variables of Interest
2.4. Statistical Analysis
2.5. Data Availability
2.6. Ethics Statement
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Camilleri, M.; Choi, M.G. Irritable bowel syndrome. Aliment. Pharmacol. Ther. 1997, 11, 3–15. [Google Scholar] [CrossRef]
- Defrees, D.N.; Bailey, J. Irritable Bowel Syndrome: Epidemiology, Pathophysiology, Diagnosis, and Treatment. Prim. Care 2017, 44, 655–671. [Google Scholar] [CrossRef]
- Drossman, D.A.; Camilleri, M.; Mayer, E.A.; Whitehead, W.E. AGA technical review on irritable bowel syndrome. Gastroenterology 2002, 123, 2108–2131. [Google Scholar] [CrossRef]
- Lu, C.L.; Chen, C.Y.; Lang, H.C.; Luo, J.C.; Wang, S.S.; Chang, F.Y.; Lee, S.D. Current patterns of irritable bowel syndrome in Taiwan: The Rome II questionnaire on a Chinese population. Aliment. Pharmacol. Ther. 2003, 18, 1159–1169. [Google Scholar] [CrossRef]
- Camilleri, M. Peripheral mechanisms in irritable bowel syndrome. N. Engl. J. Med. 2012, 367, 1626–1635. [Google Scholar] [CrossRef]
- Bellini, M.; Gambaccini, D.; Stasi, C.; Urbano, M.T.; Marchi, S.; Usai-Satta, P. Irritable bowel syndrome: A disease still searching for pathogenesis, diagnosis and therapy. World J. Gastroenterol. 2014, 20, 8807–8820. [Google Scholar]
- Mohammed, I.; Cherkas, L.F.; Riley, S.A.; Spector, T.D.; Trudgill, N.J. Genetic influences in irritable bowel syndrome: A twin study. Am. J. Gastroenterol. 2005, 100, 1340–1344. [Google Scholar] [CrossRef]
- Van Oudenhove, L.; Levy, R.L.; Crowell, M.D.; Drossman, D.A.; Halpert, A.D.; Keefer, L.; Lackner, J.M.; Murphy, T.B.; Naliboff, B.D. Biopsychosocial aspects of functional gastrointestinal disorders: How central and environmental processes contribute to the development and expression of functional gastrointestinal disorders. Gastroenterology 2016, 150, 1355–1367. [Google Scholar] [CrossRef]
- Vanner, S.J.; Greenwood-Van Meerveld, B.; Mawe, G.M.; Shea-Donohue, T.; Verdu, E.F.; Wood, J.; Grundy, D. Fundamentals of neurogastroenterology: Basic science. Gastroenterology 2016, 150, 1280–1291. [Google Scholar] [CrossRef] [Green Version]
- Agréus, L.; Svärdsudd, K.; Nyrén, O.; Tibblin, G. Irritable bowel syndrome and dyspepsia in the general population: Overlap and lack of stability over time. Gastroenterology 1995, 109, 671–680. [Google Scholar] [CrossRef]
- Zamani, M.; Ebrahimtabar, F.; Zamani, V.; Miller, W.; Alizadeh-Navaei, R.; Shokri-Shirvani, J.; Derakhshan, M. Systematic review with meta-analysis: The worldwide prevalence of Helicobacter pylori infection. Aliment. Pharmacol. Ther. 2018, 47, 868–876. [Google Scholar] [CrossRef] [Green Version]
- Bamford, K.B.; Fan, X.; Crowe, S.E.; Leary, J.F.; Gourley, W.K.; Luthra, G.K.; Brooks, E.G.; Graham, D.Y.; Reyes, V.E.; Ernst, P.B. Lymphocytes in the human gastric mucosa during Helicobacter pylori have a T helper cell 1 phenotype. Gastroenterology 1998, 114, 482–492. [Google Scholar] [CrossRef]
- Mattapallil, J.J.; Dandekar, S.; Canfield, D.R.; Solnick, J.V. A predominant Th1 type of immune response is induced early during acute Helicobacter pylori infection in rhesus macaques. Gastroenterology 2000, 118, 307–315. [Google Scholar] [CrossRef]
- Abdelrazak, M.; Walid, F.; Abdelrahman, M.; Mahmoud, M. Interrelation between helicobacter pylori infection, infantile colic, and irritable bowel syndrome in pediatric patients. J. Gastrointest Dig. Syst. 2015, 25, 5702–5710. [Google Scholar]
- Yang, Y.; Chen, L. Role of Helicobacter pylori Eradication in Diarrhea-predominant Irritable Bowel Syndrome. Chin. J. Gastroenterol. 2017, 22, 482–485. [Google Scholar]
- Ng, Q.X.; Foo, N.X.; Loke, W.; Koh, Y.Q.; Seah, V.J.M.; Soh, A.Y.S.; Yeo, W.S. Is there an association between Helicobacter pylori infection and irritable bowel syndrome? A meta-analysis. World J. Gastroenterol. 2019, 25, 5702. [Google Scholar] [CrossRef]
- Malinen, E.; Rinttilä, T.; Kajander, K.; Mättö, J.; Kassinen, A.; Krogius, L.; Saarela, M.; Korpela, R.; Palva, A. Analysis of the fecal microbiota of irritable bowel syndrome patients and healthy controls with real-time PCR. Am. J. Gastroenterol. 2005, 100, 373–382. [Google Scholar] [CrossRef]
- Chan, W.S.H. Taiwan’s healthcare report 2010. EPMA J. 2010, 1, 563–585. [Google Scholar] [CrossRef] [Green Version]
- Cheng, C.L.; Kao, Y.H.Y.; Lin, S.J.; Lee, C.H.; Lai, M.L. Validation of the National Health Insurance Research Database with ischemic stroke cases in Taiwan. Pharmacoepidemiol. Drug Saf. 2011, 20, 236–242. [Google Scholar] [CrossRef]
- Lai, M.-N.; Wang, S.-M.; Chen, P.-C.; Chen, Y.-Y.; Wang, J.-D. Population-based case–control study of Chinese herbal products containing aristolochic acid and urinary tract cancer risk. J. Natl. Cancer Inst. 2010, 102, 179–186. [Google Scholar] [CrossRef] [Green Version]
- Wu, C.-Y.; Chen, Y.-J.; Ho, H.J.; Hsu, Y.-C.; Kuo, K.N.; Wu, M.-S.; Lin, J.-T. Association between nucleoside analogues and risk of hepatitis B virus–related hepatocellular carcinoma recurrence following liver resection. JAMA 2012, 308, 1906–1913. [Google Scholar] [CrossRef] [Green Version]
- Hsieh, C.-Y.; Su, C.-C.; Shao, S.-C.; Sung, S.-F.; Lin, S.-J.; Yang, Y.-H.K.; Lai, E.C.-C. Taiwan’s National Health Insurance Research Database: Past and future. Clin. Epidemiol. 2019, 11, 349. [Google Scholar] [CrossRef] [Green Version]
- Pan, C.H.; Chang, C.C.; Su, C.T.; Tsai, P.S. Trends in Irritable Bowel Syndrome Incidence among Taiwanese Adults during 2003-2013: A Population-Based Study of Sex and Age Differences. PLoS ONE 2016, 11, e0166922. [Google Scholar] [CrossRef]
- National Health Insurance Administration. National Health Insurance Reimbursement Regulations 2018. Available online: https://law.moj.gov.tw/LawClass/LawAll.aspx?pcode=L0060006 (accessed on 14 March 2018).
- Mobley, H.L.T. The role of Helicobacter pylori urease in the pathogenesis of gastritis and peptic ulceration. Aliment. Pharmacol. Ther. 1996, 10, 57–64. [Google Scholar] [CrossRef]
- Lee, Y.; Chiang, T.-H.; Chou, C.-K.; Tu, Y.; Liao, W.-C.; Wu, M.-S.; Graham, D.Y. Association Between Helicobacter pylori Eradication and Gastric Cancer Incidence: A Systematic Review and Meta-analysis. Gastroenterology 2016, 150, 1113–1124. [Google Scholar] [CrossRef] [Green Version]
- Liu, I.-L.; Tsai, C.-H.; Hsu, C.-H.; Hu, J.-M.; Chen, Y.-C.; Tian, Y.-F.; You, S.-L.; Chen, C.-Y.; Hsiao, C.-W.; Lin, C.-Y.; et al. Helicobacter pylori infection and the risk of colorectal cancer: A nationwide population-based cohort study. Qjm Int. J. Med. 2019, 112, 787–792. [Google Scholar] [CrossRef]
- Suerbaum, S.; Michetti, P. Helicobacter pyloriInfection. N. Engl. J. Med. 2002, 347, 1175–1186. [Google Scholar] [CrossRef] [Green Version]
- Chey, W.; Leontiadis, G.I.; Howden, C.W.; Moss, S.F. ACG Clinical Guideline: Treatment of Helicobacter pylori Infection. Am. J. Gastroenterol. 2017, 112, 212–239. [Google Scholar] [CrossRef] [PubMed]
- Crowe, S.E. Helicobacter infection, chronic inflammation, and the development of malignancy. Curr. Opin. Gastroenterol. 2005, 21, 32–38. [Google Scholar]
- Jackson, L.; Britton, J.; Lewis, S.A.; McKeever, T.; Atherton, J.; Fullerton, D.; Fogarty, A.W. A Population-Based Epidemiologic Study of Helicobacter Pylori Infection and its Association with Systemic Inflammation. Helicobacter 2009, 14, 460–465. [Google Scholar] [CrossRef]
- Montemurro, P.; Nishioka, H.; Dundon, W.G.; De Bernard, M.; Del Giudice, G.; Rappuoli, R.; Montecucco, C. The neutrophil-activating protein (HP-NAP) of Helicobacter pylori is a potent stimulant of mast cells. Eur. J. Immunol. 2002, 32, 671. [Google Scholar] [CrossRef]
- Stead, R.H.; Hewlett, B.R.; Lhotak, S.; Colley, E.C.C.; Frendo, M.; Dixon, M.F. Do Gastric Mucosal Nerves Remodel in H. pylori Gastritis? Springer: Berlin/Heidelberg, Germany, 1994; pp. 281–291. [Google Scholar]
- Supajatura, V.; Ushio, H.; Wada, A.; Yahiro, K.; Okumura, K.; Ogawa, H.; Hirayama, T.; Ra, C. Cutting edge: VacA, a vacuolating cytotoxin of Helicobacter pylori, directly activates mast cells for migration and production of proinflammatory cytokines. J. Immunol. 2002, 168, 2603–2607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerards, C.; Leodolter, A.; Glasbrenner, B.; Malfertheiner, P.H. pylori infection and visceral hypersensitivity in patients with irritable bowel syndrome. Dig. Dis. 2001, 19, 170–173. [Google Scholar] [CrossRef] [PubMed]
- Öhman, L.; Simrén, M. Pathogenesis of IBS: Role of inflammation, immunity and neuroimmune interactions. Nat. Rev. Gastroenterol. Hepatol. 2010, 7, 163–173. [Google Scholar] [CrossRef]
- Rao, S.; Read, N.; Brown, C.; Bruce, C.; Holdsworth, C. Studies on the mechanism of bowel disturbance in ulcerative colitis. Gastroenterology 1987, 93, 934–940. [Google Scholar] [CrossRef]
- Stanghellini, V.; Barbara, G.; De Giorgio, R.; Tosetti, C.; Cogliandro, R.; Cogliandro, L.; Salvioli, B.; Corinaldesi, R. Helicobacter pylori, mucosal inflammation and symptom perception-new insights into an old hypothesis. Aliment. Pharmacol. Ther. 2001, 15, 28–32. [Google Scholar] [CrossRef]
- Xiong, F.; Xiong, M.; Ma, Z.; Huang, S.; Li, A.; Liu, S. Lack of association found between Helicobacter pylori infection and diarrhea-predominant irritable bowel syndrome: A multicenter retrospective study. Gastroenterol. Res. Pract. 2016, 2016, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Hooi, J.K.; Lai, W.Y.; Ng, W.K.; Suen, M.M.; Underwood, F.E.; Tanyingoh, D.; Malfertheiner, P.; Graham, D.Y.; Wong, V.W.; Wu, J.C.; et al. Global Prevalence of Helicobacter pylori Infection: Systematic Review and Meta-Analysis. Gastroenterology 2017, 153, 420–429. [Google Scholar] [CrossRef] [Green Version]
- Savoldi, A.; Carrara, E.; Graham, D.Y.; Conti, M.; Tacconelli, E. Prevalence of Antibiotic Resistance in Helicobacter pylori: A Systematic Review and Meta-analysis in World Health Organization Regions. Gastroenterology 2018, 155, 1372–1382. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| HPI | Total | With | Without | P | |||
|---|---|---|---|---|---|---|---|
| Variables | n | % | n | % | n | % | |
| Total | 13,345 | 2669 | 20.00 | 10,676 | 80.00 | ||
| Gender | 0.999 | ||||||
| Male | 8790 | 65.87 | 1758 | 65.87 | 7032 | 65.87 | |
| Female | 4555 | 34.13 | 911 | 34.13 | 3644 | 34.13 | |
| Age (years) | 57.54 ± 18.13 | 57.71 ± 17.01 | 57.70 ± 18.40 | 0.593 | |||
| Age group (years) | 0.999 | ||||||
| <44 | 3350 | 25.10 | 670 | 25.10 | 2680 | 25.10 | |
| 44–64 | 4715 | 35.33 | 943 | 35.33 | 3772 | 35.33 | |
| ≧65 | 5280 | 39.57 | 1056 | 39.57 | 4224 | 39.57 | |
| Insured premium (NT$) | 0.136 | ||||||
| <18,000 | 13,111 | 98.25 | 2613 | 97.90 | 10,498 | 98.33 | |
| 18,000–34,999 | 192 | 1.44 | 49 | 1.84 | 143 | 1.34 | |
| ≧35,000 | 42 | 0.31 | 7 | 0.26 | 35 | 0.33 | |
| CAD | <0.001 | ||||||
| Without | 12,087 | 90.57 | 2508 | 93.97 | 9579 | 89.72 | |
| With | 1258 | 9.43 | 161 | 6.03 | 1097 | 10.28 | |
| CVA | <0.001 | ||||||
| Without | 12,312 | 92.26 | 2583 | 96.78 | 9729 | 91.13 | |
| With | 1033 | 7.74 | 86 | 3.22 | 947 | 8.87 | |
| HTN | <0.001 | ||||||
| Without | 10,738 | 80.46 | 2247 | 84.19 | 8491 | 79.53 | |
| With | 2607 | 19.54 | 422 | 15.81 | 2185 | 20.47 | |
| Hyperlipidemia | 0.001 | ||||||
| Without | 12,904 | 96.70 | 2609 | 97.75 | 10,295 | 96.43 | |
| With | 441 | 3.30 | 60 | 2.25 | 381 | 3.57 | |
| DM | 0.031 | ||||||
| Without | 11,238 | 84.21 | 2284 | 85.58 | 8954 | 83.87 | |
| With | 2107 | 15.79 | 385 | 14.42 | 1722 | 16.13 | |
| ESRD | - | ||||||
| Without | 13,345 | 100.00 | 2669 | 100.00 | 10,676 | 100.00 | |
| With | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | |
| Asthma | 0.001 | ||||||
| Without | 13,098 | 98.15 | 2640 | 98.91 | 10,458 | 97.96 | |
| With | 247 | 1.85 | 29 | 1.09 | 218 | 2.04 | |
| CCI_R | 0.47 ± 0.81 | 1.27 ± 0.77 | 0.27 ± 0.69 | <0.001 | |||
| Season | <0.001 | ||||||
| Spring (Mar–May) | 3466 | 25.97 | 628 | 23.53 | 2838 | 26.58 | |
| Summer (Jun–Aug) | 3264 | 24.46 | 674 | 25.25 | 2590 | 24.26 | |
| Autumn (Sep–Nov) | 3019 | 22.62 | 696 | 26.08 | 2323 | 21.76 | |
| Winter (Dec–Feb) | 3596 | 26.95 | 671 | 25.14 | 2925 | 27.40 | |
| Location | <0.001 | ||||||
| Northern Taiwan | 4850 | 36.34 | 835 | 31.29 | 4015 | 37.61 | |
| Middle Taiwan | 3674 | 27.53 | 462 | 17.31 | 3212 | 30.09 | |
| Southern Taiwan | 3744 | 28.06 | 1,005 | 37.65 | 2739 | 25.66 | |
| Eastern Taiwan | 1014 | 7.60 | 366 | 13.71 | 648 | 6.07 | |
| Outlets islands | 63 | 0.47 | 1 | 0.04 | 62 | 0.58 | |
| Urbanization level | <0.001 | ||||||
| 1 (The highest) | 4030 | 30.20 | 762 | 28.55 | 3268 | 30.61 | |
| 2 | 5998 | 44.95 | 1328 | 49.76 | 4670 | 43.74 | |
| 3 | 1202 | 9.01 | 360 | 13.49 | 842 | 7.89 | |
| 4 (The lowest) | 2115 | 15.85 | 219 | 8.21 | 1896 | 17.76 | |
| Level of care | <0.001 | ||||||
| Hospital center | 4019 | 30.12 | 685 | 25.67 | 3334 | 31.23 | |
| Regional hospital | 5786 | 43.36 | 1374 | 51.48 | 4412 | 41.33 | |
| Local hospital | 3540 | 26.53 | 610 | 22.86 | 2930 | 27.44 | |
| Variables | Crude HR | 95% CI | 95% CI | P | Adjusted HR | 95% CI | 95% CI | P |
|---|---|---|---|---|---|---|---|---|
| HPI | ||||||||
| Without | Reference | Reference | ||||||
| With | 2.887 | 1.801 | 4.626 | <0.001 | 3.108 | 1.934 | 4.995 | <0.001 |
| Gender | ||||||||
| Male | 0.873 | 0.539 | 1.412 | 0.579 | 1.075 | 0.474 | 1.268 | 0.310 |
| Female | Reference | Reference | ||||||
| Age group (years) | ||||||||
| <44 | Reference | Reference | ||||||
| 44–64 | 0.877 | 0.457 | 1.683 | 0.693 | 1.112 | 0.566 | 2.187 | 0.757 |
| ≧65 | 0.700 | 0.378 | 1.295 | 0.256 | 0.817 | 0.416 | 1.605 | 0.557 |
| Insured premium (NT$) | ||||||||
| <18,000 | Reference | Reference | ||||||
| 18,000–34,999 | 0.000 | - | - | 0.507 | 0.000 | - | - | 0.966 |
| ≧35,000 | 0.000 | - | - | 0.777 | 0.000 | - | - | 0.987 |
| CAD | ||||||||
| Without | Reference | Reference | ||||||
| With | 0.994 | 0.409 | 1.952 | 0.778 | 1.194 | 0.535 | 2.663 | 0.665 |
| CVA | ||||||||
| Without | Reference | Reference | ||||||
| With | 2.279 | 1.268 | 4.094 | 0.006 | 3.121 | 1.670 | 5.834 | <0.001 |
| HTN | ||||||||
| Without | Reference | Reference | ||||||
| With | 1.537 | 0.298 | 2.094 | 0.285 | 1.552 | 0.286 | 2.065 | 0.077 |
| Hyperlipidemia | ||||||||
| Without | Reference | Reference | ||||||
| With | 1.042 | 0.506 | 2.894 | 0.366 | 1.048 | 0.561 | 3.317 | 0.432 |
| DM | ||||||||
| Without | Reference | Reference | ||||||
| With | 1.462 | 0.921 | 2.965 | 0.054 | 1.488 | 0.729 | 2.042 | 0.064 |
| ESRD | ||||||||
| Without | Reference | Reference | ||||||
| With | - | - | - | - | - | - | - | - |
| Asthma | ||||||||
| Without | Reference | Reference | ||||||
| With | 1.475 | 0.361 | 6.018 | 0.588 | 1.809 | 0.433 | 7.550 | 0.416 |
| CCI_R | 0.905 | 0.775 | 1.058 | 0.209 | 1.017 | 0.875 | 1.184 | 0.309 |
| Season | ||||||||
| Spring | Reference | Reference | ||||||
| Summer | 2.068 | 0.668 | 2.942 | 0.829 | 2.142 | 0.626 | 2.886 | 0.665 |
| Autumn | 1.532 | 0.573 | 2.037 | 0.064 | 1.543 | 0.578 | 2.147 | 0.074 |
| Winter | 1.389 | 1.175 | 1.864 | 0.020 | 1.413 | 1.186 | 1.919 | 0.030 |
| Location | ||||||||
| Northern Taiwan | Reference | |||||||
| Middle Taiwan | 2.289 | 1.238 | 4.231 | 0.008 | ||||
| Southern Taiwan | 1.532 | 0.788 | 2.980 | 0.209 | ||||
| Eastern Taiwan | 1.893 | 0.779 | 4.605 | 0.159 | ||||
| Outlets islands | 0.000 | - | - | 0.968 | ||||
| Urbanization level | ||||||||
| 1 (The highest) | 2.294 | 1.190 | 4.423 | 0.013 | 1.536 | 0.259 | 1.701 | 0.092 |
| 2 | 1.378 | 0.535 | 3.551 | 0.507 | 1.331 | 0.291 | 1.696 | 0.084 |
| 3 | 1.092 | 0.581 | 2.052 | 0.785 | 0.581 | 0.235 | 1.438 | 0.240 |
| 4 (The lowest) | Reference | Reference | ||||||
| Level of care | ||||||||
| Hospital center | 2.514 | 1.280 | 4.937 | 0.007 | 1.790 | 0.498 | 2.698 | 0.396 |
| Regional hospital | 1.690 | 0.890 | 3.212 | 0.109 | 1.590 | 0.275 | 2.224 | 0.177 |
| Local hospital | Reference | Reference | ||||||
| With HPI | Without HPI | With vs. Without | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Event | PYs | Rate | Event | PYs | Rate | Ratio | Adjusted HR | 95% CI | 95% CI | P | |
| Total | 31 | 28,376.11 | 109.25 | 39 | 115,278.73 | 33.83 | 3.229 | 3.108 | 1.934 | 4.995 | <0.001 |
| Gender | |||||||||||
| Male | 19 | 18,081.31 | 105.08 | 24 | 74,553.61 | 32.19 | 3.264 | 3.228 | 1.487 | 7.010 | 0.003 |
| Female | 12 | 10,294.81 | 116.56 | 15 | 40,725.13 | 36.83 | 3.165 | 3.074 | 1.678 | 5.629 | <0.001 |
| Age group (years) | |||||||||||
| <44 | 7 | 5265.65 | 132.94 | 8 | 20,134.93 | 39.73 | 3.346 | 3.269 | 1.130 | 9.458 | 0.029 |
| 44–64 | 13 | 8407.04 | 154.63 | 10 | 34,593.43 | 28.91 | 5.349 | 4.971 | 2.148 | 11.503 | <0.001 |
| ≧65 | 11 | 14,703.42 | 74.81 | 21 | 60,550.38 | 34.68 | 2.157 | 2.201 | 1.506 | 4.589 | 0.035 |
| Insured premium (NT$) | |||||||||||
| <18,000 | 31 | 27,747.83 | 111.72 | 39 | 113,542.93 | 34.35 | 3.253 | 3.108 | 1.934 | 4.995 | <0.001 |
| 18,000–34,999 | 0 | 624.29 | 0.00 | 0 | 1380.70 | 0.00 | - | - | - | - | - |
| ≧35,000 | 0 | 4.00 | 0.00 | 0 | 355.11 | 0.00 | - | - | - | - | - |
| CAD | |||||||||||
| Without | 26 | 25,383.09 | 102.43 | 34 | 102,503.61 | 33.17 | 3.088 | 1.654 | 0.246 | 11.141 | 0.605 |
| With | 5 | 2993.02 | 167.06 | 5 | 12,775.13 | 39.14 | 4.268 | 3.268 | 1.986 | 5.378 | <0.001 |
| CVA | |||||||||||
| Without | 22 | 25,674.01 | 85.69 | 29 | 103,869.28 | 27.92 | 3.069 | 2.475 | 1.427 | 5.098 | 0.039 |
| With | 9 | 2702.10 | 333.07 | 10 | 11,409.45 | 87.65 | 3.800 | 3.605 | 2.127 | 6.110 | <0.001 |
| HTN | |||||||||||
| Without | 24 | 20,486.19 | 117.15 | 34 | 83,677.62 | 40.63 | 2.883 | 2.775 | 1.639 | 4.697 | <0.001 |
| With | 7 | 7889.93 | 88.72 | 5 | 31,601.12 | 15.82 | 5.607 | 4.702 | 1.463 | 15.116 | <0.001 |
| Hyperlipidemia | |||||||||||
| Without | 31 | 27,470.42 | 112.85 | 38 | 111,100.13 | 34.20 | 3.299 | 3.186 | 1.977 | 5.133 | <0.001 |
| With | 0 | 905.70 | 0.00 | 1 | 4178.61 | 23.93 | 0.000 | 0.000 | - | - | 0.752 |
| DM | |||||||||||
| Without | 25 | 22,236.72 | 112.43 | 37 | 90,656.96 | 40.81 | 2.755 | 2.655 | 1.592 | 4.427 | <0.001 |
| With | 6 | 6139.39 | 97.73 | 2 | 24,621.78 | 8.12 | 12.031 | 15.952 | 2.797 | 90.961 | <0.001 |
| ESRD | |||||||||||
| Without | 31 | 28,376.11 | 109.25 | 39 | 115,278.73 | 33.83 | 3.229 | 3.108 | 1.934 | 4.995 | <0.001 |
| With | 0 | 0.00 | - | 0 | 0.00 | - | - | - | - | - | - |
| Asthma | |||||||||||
| Without | 30 | 27,885.94 | 107.58 | 38 | 113,027.76 | 33.62 | 3.200 | 3.050 | 1.884 | 4.937 | <0.001 |
| With | 1 | 490.17 | 204.01 | 1 | 2250.98 | 44.43 | 4.592 | 4.497 | 0.009 | 12.589 | 0.747 |
| Season | |||||||||||
| Spring | 7 | 5786.86 | 120.96 | 12 | 24,237.41 | 49.51 | 2.443 | 2.197 | 0.847 | 5.700 | 0.105 |
| Summer | 12 | 6943.36 | 172.83 | 13 | 28,874.00 | 45.02 | 3.839 | 4.035 | 1.809 | 8.999 | 0.001 |
| Autumn | 8 | 9022.10 | 88.67 | 9 | 34,938.86 | 25.76 | 3.442 | 3.594 | 1.367 | 9.447 | 0.009 |
| Winter | 4 | 6623.80 | 60.39 | 5 | 27,228.47 | 18.36 | 3.289 | 2.658 | 0.685 | 10.312 | 0.158 |
| Urbanization level | |||||||||||
| 1 (The highest) | 9 | 7304.40 | 123.21 | 6 | 32,885.51 | 18.25 | 6.753 | 6.726 | 2.272 | 19.907 | 0.001 |
| 2 | 13 | 14,376.62 | 90.42 | 14 | 51,741.11 | 27.06 | 3.342 | 3.069 | 1.434 | 6.568 | 0.004 |
| 3 | 2 | 2293.89 | 87.19 | 4 | 9283.94 | 43.09 | 2.024 | 1.936 | 0.336 | 11.480 | 0.453 |
| 4 (The lowest) | 7 | 4401.19 | 159.05 | 15 | 21,368.18 | 70.20 | 2.266 | 1.947 | 0.779 | 4.865 | 0.154 |
| Level of care | |||||||||||
| Hospital center | 7 | 8402.69 | 83.31 | 6 | 36,328.46 | 16.52 | 5.044 | 5.402 | 1.774 | 16.446 | 0.003 |
| Regional hospital | 17 | 13,757.36 | 123.57 | 16 | 52,465.12 | 30.50 | 4.052 | 3..462 | 1.735 | 6.909 | <0.001 |
| Local hospital | 7 | 6216.06 | 112.61 | 17 | 26,485.15 | 64.19 | 1.754 | 1.590 | 0.645 | 3.917 | 0.313 |
| HPI Cohort and Comparison Cohort | HPI Cohort | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Study Population | Event | PYs | Rate | Adjusted HR | 95% CI | 95% CI | P | Adjusted HR | 95% CI | 95% CI | P |
| Without HPI | 39 | 28,376.11 | 137.44 | Reference | |||||||
| With HPI | 31 | 28,376.11 | 109.25 | ||||||||
| without medication | 25 | 16,605.68 | 150.55 | 4.160 | 2.508 | 6.900 | <0.001 | Reference | |||
| with medication | 6 | 11,770.44 | 50.98 | 0.916 | 0.241 | 2.590 | 0.344 | 0.464 | 0.148 | 0.963 | 0.037 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liang, C.-M.; Hsu, C.-H.; Chung, C.-H.; Chen, C.-Y.; Wang, L.-Y.; Hsu, S.-D.; Chang, P.-K.; Hong, Z.-J.; Chien, W.-C.; Hu, J.-M. Risk for Irritable Bowel Syndrome in Patients with Helicobacter Pylori Infection: A Nationwide Population-Based Study Cohort Study in Taiwan. Int. J. Environ. Res. Public Health 2020, 17, 3737. https://doi.org/10.3390/ijerph17103737
Liang C-M, Hsu C-H, Chung C-H, Chen C-Y, Wang L-Y, Hsu S-D, Chang P-K, Hong Z-J, Chien W-C, Hu J-M. Risk for Irritable Bowel Syndrome in Patients with Helicobacter Pylori Infection: A Nationwide Population-Based Study Cohort Study in Taiwan. International Journal of Environmental Research and Public Health. 2020; 17(10):3737. https://doi.org/10.3390/ijerph17103737
Chicago/Turabian StyleLiang, Chia-Ming, Chih-Hsiung Hsu, Chi-Hsiang Chung, Chao-Yang Chen, Lin-Yin Wang, Sheng-Der Hsu, Pi-Kai Chang, Zhi-Jie Hong, Wu-Chien Chien, and Je-Ming Hu. 2020. "Risk for Irritable Bowel Syndrome in Patients with Helicobacter Pylori Infection: A Nationwide Population-Based Study Cohort Study in Taiwan" International Journal of Environmental Research and Public Health 17, no. 10: 3737. https://doi.org/10.3390/ijerph17103737