Longitudinal Relationship Study of Depression and Self-Esteem in Postnatal Korean Women Using Autoregressive Cross-Lagged Modeling


Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Design
2.2. Research Subjects
2.3. Measurements
2.3.1. Depression
2.3.2. Self-Esteem
2.3.3. Study Groups
2.3.4. Exogenous Variables
Parenting Stress
Household Income
Employment Status
2.4. Data Collection and Analysis
3. Results
3.1. General Characteristics of the Subjects
3.2. Normality Test of Measurement Variables
3.3. Correlation between the Measurement Variables
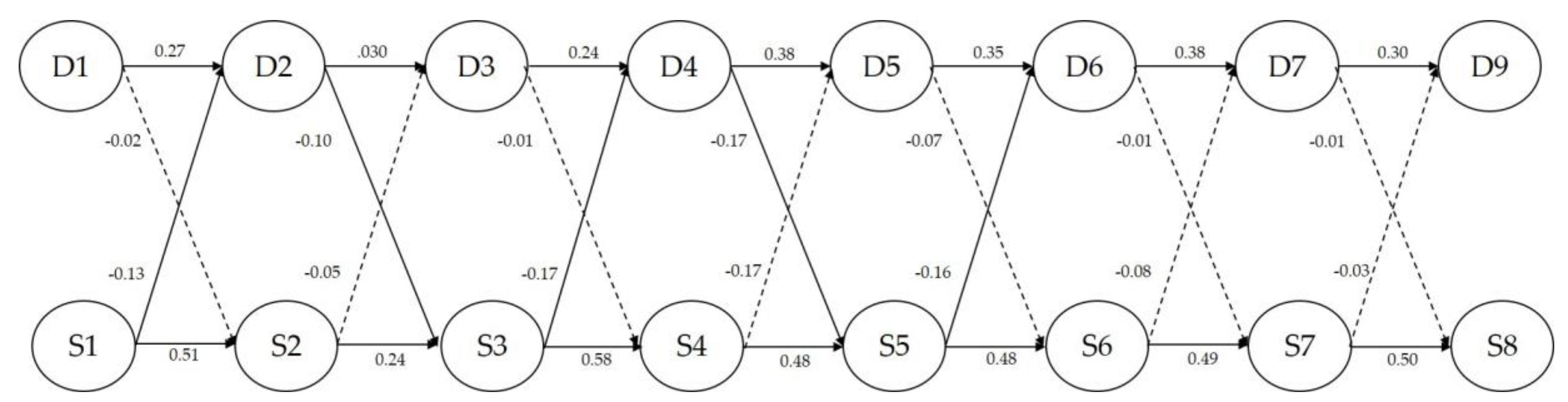
3.4. Relationship between the Measurement Variables
3.5. Difference in Weight Gain during Pregnancy between Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Vernon, M.M.; Young-Hyman, D.; Looney, S.W. Maternal stress, physical activity, and body mass index during new mothers’ first year postpartum. Women Health 2011, 50, 544–562. [Google Scholar] [CrossRef]
- Ahn, Y.M.; Kim, J.H. Comparison of maternal self-esteem, postpartal depression, and family function in mothers of normal and of low birth-weight infants. J. Korean Acad. Nurs. 2003, 33, 580–590. [Google Scholar] [CrossRef]
- Sowislo, J.F.; Orth, U. Does low self-esteem predict depression and anxiety? A meta-analysis of longitudinal studies. Psychol. Bull. 2013, 139, 213–240. [Google Scholar] [CrossRef]
- Shahar, G.; Davidson, L. Depressive symptoms erode self-esteem in severe mental illness: A three-wave, cross-lagged study. J. Consult. Clin. Psychol. 2003, 71, 890–900. [Google Scholar] [CrossRef]
- Orth, U.; Robins, R.W.; Roberts, B.W. Low self-esteem prospectively predicts depression in adolescence and young adulthood. J. Pers. Soc. Psychol. 2008, 95, 695–708. [Google Scholar] [CrossRef] [Green Version]
- Dolatian, M.; Mirrabzadeh, A.; Setareh Forouzan, A.; Sajjadi, H.; Alawimajd, H.; Maafi, F.; Zohreh, M. Correlation of self-esteem with perceived self-esteem in pregnancy and strategies to cope with stress. Pajoohandeh J. 2013, 18, 148–155. [Google Scholar]
- Garoosi, B.; Razavi, V.; Etminan, A.R. Investigating the relationship between depression and self-esteem in pregnant women in terms of their conception of their body. J. Health Dev. 2013, 6, 117–127. [Google Scholar]
- Logsdon, M.C.; Wisner, K.; Sit, D.; Luther, J.F.; Wisniewski, S.R. Depression treatment and maternal functioning. Depress. Anxiety 2011, 28, 1020–1026. [Google Scholar] [CrossRef]
- Kim, S.M.; Lee, J.; Ahn, B.H.; Park, S.B.; Kim, K.M.; Kim, H.S. A prospective study for weight changes associated with pregnancy. Korean J. Fam. Med. 2001, 22, 895–903. [Google Scholar]
- Schall, J.I.; Ances, I.G.; Smith, W.K. Gestational weight gain, pregnancy outcome, and postpartum weight retention. Obstet. Gynecol. 1995, 86, 423–427. [Google Scholar] [CrossRef]
- Lee, E.J.; Park, J.S. Development of a prediction model for postpartum depression: Based on the mediation effect of antepartum depression. J. Korean Acad. Nurs. 2015, 45, 211–220. [Google Scholar] [CrossRef] [Green Version]
- Lebel, C.; Walton, M.; Letourneau, N.; Giesbrecht, G.F.; Kaplan, B.J.; Dewey, D. Prepartum and postpartum maternal depressive symptoms are related to children’s brain structure in preschool. Biol. Psychiatry 2016, 80, 859–868. [Google Scholar] [CrossRef]
- American Pregnancy Association. Depression in Pregnancy: Depression during pregnancy: Signs, symptoms and treatment. Available online: http://americanpregnancy.org/pregnancy-health/depression-during-pregnancy. (accessed on 8 August 2019).
- Lim, C.C.; Mahmood, T. Obesity in pregnancy. Best Pract. Res. Clin. Obstet. Gynaecol. 2015, 29, 309–319. [Google Scholar] [CrossRef]
- Danielle, S.D.; Jennifer, M.; DiNallo, M.A.; Tiffany, L.; Kirner, B.S. Determinants of pregnancy and postpartum depression: Prospective influences of depressive symptoms, body image satisfaction, and exercise behavior. Ann. Behav. Med. 2008, 36, 54–63. [Google Scholar]
- De Wit, L.; Luppino, F.; Van Straten, A.; Penninx, B.; Zitman, F.; Cuijpers, P. Depression and obesity: A meta-analysis of community-based studies. Psychiatry Res. 2010, 178, 230–235. [Google Scholar] [CrossRef]
- Pedersen, P.; Baker, J.L.; Henriksen, T.B. Influence of psychosocial factors on postpartum weight retention. Obesity 2011, 19, 639–646. [Google Scholar] [CrossRef]
- Chung, C.W.; Kim, H.W.; Kim, H.J. Body weight changes and lifestyle in women within 1 year after childbirth. Perspect. Nurs. Sci. 2016, 13, 88–95. [Google Scholar] [CrossRef] [Green Version]
- Mehta, U.J.; Siega-Riz, A.M.; Herring, A.H. Effect of body image on pregnancy weight gain. Matern. Child. Health J. 2011, 15, 324–332. [Google Scholar] [CrossRef] [Green Version]
- Vaz, S.; Falkmer, M.; Parsons, R.; Passmore, A.E.; Parkin, T.; Falkmer, T. School belongingness and mental health functioning across the primary-secondary transition in a mainstream sample: Multi-group cross-lagged analyses. PLoS ONE 2014, 9, e99576. [Google Scholar] [CrossRef]
- Kessler, R.C.; Andrew, G.; Cople, L.J.; Hiripi, E.; Mroczek, D.K.; Normand, S.L.T.; Walters, E.E.; Zaslavsky, A.M. Short screening scales to monitor population prevalences and trends in nonspecific psychological distress. Psychol. Med. 2002, 32, 959–976. [Google Scholar] [CrossRef]
- Rosenberg, M. Society and the Adolescent Self-Image; Princeton University Press: Princeton, NJ, USA, 1965. [Google Scholar]
- Schauberg, C.W.; Rooney, B.L.; Brimer, L.M. Factors that influence weight loss in the puerperium. Obstet. Gynecol. 1992, 79, 424–429. [Google Scholar] [CrossRef]
- O’Keane, V.; Marsh, M.S. Depression during pregnancy. Br. Med. J. 2007, 334, 1003–1005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agoub, M.; Moussaoui, D.; Battas, O. Prevalence of postpartum depression in a Moroccan sample. Arch. Womens Ment. Health 2005, 8, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Alami, K.; Kadri, N.; Berrada, S. Prevalence and psychosocial correlates of depressed mood during pregnancy and after childbirth in a Moroccan sample. Arch. Womens Ment. Health 2006, 9, 343–346. [Google Scholar] [CrossRef] [PubMed]
- Cho, H.W.; Woo, J.Y. The relational structure modeling between variables related with postpartum depression. Korean J. Counsel. Psychotherapy 2013, 25, 549–573. [Google Scholar]
- Friedman, S.H.; Resnick, P.J. Children of depressed parents: An integrative review. Women’s Health 2009, 5, 287–295. [Google Scholar]
- Woolhouse, H.; Gartland, D.; Perlen, S.; Donath, S.; Brown, S.J. Physical health after childbirth and maternal depression in the first 12 months post-partum: Results of an Australian nulliparous pregnancy cohort study. Midwifery 2014, 30, 378–384. [Google Scholar] [CrossRef]
- Kim, C.K. A qualitative study on depression experience of middle aged depression women. Korean J. Counsel. 2010, 11, 1783–1806. [Google Scholar]
- Cho, Y.S. The relationship of postpartum mother’s self-esteem and depression. J. Korean Acad. Psychiatr. Nurs. 1992, 1, 97–110. [Google Scholar]
- Erikson, E.H. Identity and the Life Cycle; Norton & Company: New York, NY, USA, 1994; pp. 7–64. [Google Scholar]
- Kim, M.E.; Hur, M.H. Sleep quality, fatigue, and postpartum depression of mother at six months after delivery. Korean J. Women Health Nurs. 2014, 20, 266–276. (In Korean) [Google Scholar] [CrossRef] [Green Version]
- Park, Y.S.; Cho, D.S.; Lee, E.H.; Kim, J.I.; Shin, H.S.; Jung, J.W. Women’s Health Nursing II, 7th ed.; Paju: Soomoonsa, Korea, 2012; pp. 18–356. [Google Scholar]
- Askelsdottir, B.; Lam-de Jonge, W.; Edman, G.; Wiklund, I. Home care after early discharge: Impact on healthy mothers and newborns. Midwifery 2013, 29, 927–934. [Google Scholar] [CrossRef] [PubMed]
- Hasanpour, M.; Alavi, M.; Azizi, F.; Als, H.; Armanian, A.M. Iranian parent-staff communication and parental stress in the neonatal intensive care unit. J. Educ. Health Promot. 2017, 6, e49. [Google Scholar]
- Klainin, P.; Arthur, D.G. Postpartum depression in Asian cultures: A literature review. Int. J. Nurs Stud. 2009, 46, 1355–1373. [Google Scholar] [CrossRef] [PubMed]
- Dennis, C.L. Can we identify mothers at risk for postpartum depression in the immediate postpartum in the immediate postpartum period using the Edinburgh Postnatal Depression Scale? J. Affect. Disord. 2004, 78, 163–169. [Google Scholar] [CrossRef]
- Cuypers, K.; Kvaloy, K.; Bratberg, G.; Midthjell, K.; Holmen, J.; Holmen, T.L. Being normal weight but feeling overweight in adolescence may affect weight development into young adulthoodan 11-year follow up: The HUNT study, Norway. J. Obes. 2012, 2012, 601872. [Google Scholar]
- Choi, Y.K. Overview of women’s mental health: Gender bias and gender-specific risk factors. Gend. Cult. 2010, 3, 203–232. [Google Scholar]
- Seoul Citizens’ Perception Survey Report on Mental Health in 2013; Seoul Mental Health Promotion Center: Seoul, Korea, 2013.


{kind=link}
| Variables | n | % | |
|---|---|---|---|
| Age, years | <30 | 181 | 42.9 |
| (Mean ± SD = 30.59 ± 3.60) | 30–35 | 197 | 46.6 |
| <35 | 45 | 10.5 | |
| Duration of marriage, months | ≤12 | 53 | 12.6 |
| (Mean ± SD = 30.30 ± 23.80) | 13–24 | 179 | 42.4 |
| 25–36 | 100 | 23.7 | |
| ≤37 | 91 | 21.3 | |
| Education level | High school graduate or less | 101 | 23.9 |
| 2-year college degree | 130 | 30.7 | |
| Bachelor’s degree or higher | 192 | 45.4 | |
| Religion | No | 192 | 45.4 |
| Yes | 231 | 54.6 | |
| of Reproduction assistance techniques used | Naturally conceived | 396 | 93.6 |
| Received assistance | 27 | 6.4 | |
| Delivery type | Normal spontaneous delivery | 228 | 53.9 |
| Unplanned emergency C-sections | 138 | 32.6 | |
| Planned emergency C-sections | 57 | 13.5 | |
| BMI (before pregnancy), kg/m2 | <18.5 | 70 | 16.5 |
| 18.5–24.9 | 313 | 74.0 | |
| <25.0 | 40 | 9.5 | |
| Total weight gain during pregnancy, kg | Overweight | 98 | 23.2 |
| Maintained normal weight gain | 325 | 76.8 | |
| Variables | Mean | SD | Skewness | SE | Kurtosis | SE |
|---|---|---|---|---|---|---|
| Depression wave 1 | 1.78 | 0.66 | 0.93 | 0.12 | 1.34 | 0.24 |
| Depression wave 2 | 1.75 | 0.63 | 0.65 | 0.12 | 0.30 | 0.24 |
| Depression wave 3 | 1.82 | 0.58 | 0.65 | 0.12 | 1.30 | 0.24 |
| Depression wave 4 | 1.86 | 0.66 | 0.70 | 0.12 | 0.34 | 0.24 |
| Depression wave 5 | 1.88 | 0.64 | 0.61 | 0.12 | 0.19 | 0.24 |
| Depression wave 6 | 1.86 | 0.64 | 0.67 | 0.12 | 0.47 | 0.24 |
| Depression wave 7 | 1.82 | 0.66 | 0.77 | 0.12 | 0.85 | 0.24 |
| Depression wave 8 | 1.72 | 0.63 | 1.21 | 0.12 | 2.14 | 0.24 |
| Self-esteem wave 1 | 3.77 | 0.47 | −0.21 | 0.12 | 0.31 | 0.24 |
| Self-esteem wave 2 | 3.74 | 0.48 | −0.45 | 0.12 | 2.14 | 0.24 |
| Self-esteem wave 3 | 3.71 | 0.45 | 0.10 | 0.12 | 0.66 | 0.24 |
| Self-esteem wave 4 | 3.71 | 0.55 | −0.02 | 0.12 | -0.18 | 0.24 |
| Self-esteem wave 5 | 3.77 | 0.52 | −0.32 | 0.12 | 0.10 | 0.24 |
| Self-esteem wave 6 | 3.81 | 0.52 | −0.18 | 0.12 | 0.18 | 0.24 |
| Self-esteem wave 7 | 3.83 | 0.53 | −0.23 | 0.12 | 0.03 | 0.24 |
| Self-esteem wave 8 | 3.86 | 0.52 | −0.36 | 0.12 | 0.34 | 0.24 |
| Parenting stress wave 1 | 2.52 | 0.58 | 0.05 | 0.11 | 0.29 | 0.24 |
| Parenting stress wave 2 | 2.48 | 0.58 | 0.10 | 0.11 | 0.26 | 0.24 |
| Parenting stress wave 3 | 2.63 | 0.54 | 0.10 | 0.11 | 0.66 | 0.24 |
| Parenting stress wave 4 | 2.64 | 0.60 | 0.03 | 0.11 | 0.18 | 0.24 |
| Parenting stress wave 5 | 2.63 | 0.61 | 0.18 | 0.11 | 0.06 | 0.24 |
| Parenting stress wave 6 | 2.58 | 0.58 | -0.08 | 0.11 | 0.02 | 0.24 |
| Parenting stress wave 7 | 2.51 | 0.57 | 0.14 | 0.11 | 0.06 | 0.24 |
| Parenting stress wave 8 | 2.33 | 0.61 | 0.17 | 0.11 | 0.12 | 0.24 |
| Household income wave 1 | 2622.32 | 1106.71 | 1.32 | 0.12 | 2.77 | 0.24 |
| Household income wave 2 | 32596.15 | 1052.17 | 1.06 | 0.12 | 2.45 | 0.24 |
| Household income wave 3 | 3108.26 | 1505.09 | 1.89 | 0.12 | 2.94 | 0.24 |
| Household income wave 4 | 3243.82 | 1179.80 | 1.60 | 0.12 | 2.40 | 0.24 |
| Household income wave 5 | 3149.34 | 1072.62 | 1.53 | 0.12 | 0.24 | 0.24 |
| Household income wave 6 | 2624.19 | 1222.27 | 1.65 | 0.12 | 2.32 | 0.24 |
| Household income wave 7 | 2900.30 | 1563.37 | 2.05 | 0.12 | 2.49 | 0.24 |
| Household income wave 8 | 2828.65 | 1641.94 | 1.83 | 0.12 | 2.95 | 0.24 |
| Variables | X1 | X2 | X3 | X4 | X5 | X6 | X7 | X8 | X9 | X10 | X11 | X12 | X13 | X14 | X15 | X16 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| X1 | 1 | |||||||||||||||
| X2 | 0.46 * | 1 | ||||||||||||||
| X3 | 0.42 * | 0.40 * | 1 | |||||||||||||
| X4 | 0.46 * | 0.41 * | 0.42 * | 1 | ||||||||||||
| X5 | 0.46 * | 0.45 * | 0.40 * | 0.49 * | 1 | |||||||||||
| X6 | 0.41 * | 0.37 * | 0.41 * | 0.40 * | 0.53 * | 1 | ||||||||||
| X7 | 0.48 * | 0.42 * | 0.40 * | 0.42 * | 0.50 * | 0.56 * | 1 | |||||||||
| X8 | 0.39 * | 0.33 * | 0.33 * | 0.37 * | 0.40 * | 0.39 * | 0.50 * | 1 | ||||||||
| X9 | −0.53 * | −0.40 * | −0.23 * | −0.34 * | −0.32 * | −0.28 * | −0.43 * | −0.29 * | 1 | |||||||
| X10 | −0.34 * | −0.45 * | −0.21 * | −0.23 * | −0.27 * | −0.25 * | −0.31 * | −0.26 * | 0.58 * | 1 | ||||||
| X11 | −0.40 * | −0.34 * | −0.53 * | −0.39 * | −0.36 * | −0.36 * | −0.41 * | −0.32 * | 0.51 * | 0.41 * | 1 | |||||
| X12 | −0.40 * | −0.34 * | −0.32 * | −0.50 * | −0.31 * | −0.29 * | −0.34 * | −0.32 * | 0.56 * | 0.50 * | 0.63 * | 1 | ||||
| X13 | −0.38 * | −0.35 * | −0.29 * | −0.36 * | −0.56 * | −0.36 * | −0.43 * | −0.28 * | 0.50 * | 0.49 * | 0.54 * | 0.61 * | 1 | |||
| X14 | −0.31 * | −0.31 * | −0.25 * | −0.27 * | −0.37 * | −0.48 * | −0.45 * | −0.32 * | 0.46 * | 0.47 * | 0.45 * | 0.56 * | 0.63 * | 1 | ||
| X15 | −0.28 * | −0.26 * | −0.30 * | −0.29 * | −0.37 * | −0.36 * | −0.53 * | −0.33 * | 0.48 * | 0.39 * | 0.49 * | 0.52 * | 0.58 * | 0.64 * | 1 | |
| X16 | –0.29 * | –0.28 * | –0.33 * | –0.29 * | –0.35 * | –0.32 * | –0.43 * | –0.48 * | 0.43 * | 0.44 * | 0.53 * | 0.59 * | 0.55 * | 0.61 * | 0.66 * | 1 |
| Model | χ2 | df | NFI | CFI | TLI | RMSEA |
|---|---|---|---|---|---|---|
| Model 1 | 812.17 | 91 | 0.77 | 0.78 | 0.70 | 0.07 |
| Model 2 | 308.23 | 84 | 0.90 | 0.92 | 0.84 | 0.03 |
| Model 3 | 316.94 | 90 | 0.90 | 0.92 | 0.86 | 0.02 |
| Model 4 | 372.79 | 98 | 0.89 | 0.91 | 0.86 | 0.02 |
| Model 5 | 377.28 | 102 | 0.89 | 0.91 | 0.87 | 0.02 |
| Model 6 | 391.20 | 108 | 0.88 | 0.91 | 0.88 | 0.02 |
| Model 7 | 408.34 | 114 | 0.87 | 0.90 | 0.89 | 0.02 |
| Pathway | B | β | CR | p | Critical Ratio for Difference |
|---|---|---|---|---|---|
| Depression 1st -> Depression 2nd | 0.25 | 0.27 | 5.44 | <0.001 | −0.402 |
| Depression 2nd -> Depression 3rd | 0.27 | 0.30 | 6.28 | <0.001 | −0.889 |
| Depression 3rd -> Depression 4th | 0.27 | 0.24 | 5.13 | <0.001 | −0.434 |
| Depression 4th -> Depression 5th | 0.36 | 0.38 | 8.47 | <0.001 | 0.273 |
| Depression 5th -> Depression 6th | 0.35 | 0.35 | 7.89 | <0.001 | 0.104 |
| Depression 6th -> Depression 7th | 0.38 | 0.38 | 8.94 | <0.001 | −0.304 |
| Depression 7th -> Depression 8th | 0.30 | 0.30 | 7.05 | <0.001 | −3.204 * |
| Self-esteem 1st -> Self-esteem 2nd | 0.50 | 0.51 | 10.87 | <0.001 | 0.345 |
| Self-esteem 2nd -> Self-esteem 3rd | 0.22 | 0.24 | 5.15 | <0.001 | 1.662 |
| Self-esteem 3rd -> Self-esteem 4th | 0.51 | 0.58 | 14.09 | <0.001 | 0.432 |
| Self-esteem 4th -> Self-esteem 5th | 0.44 | 0.48 | 11.32 | <0.001 | −1.343 |
| Self-esteem 5th -> Self-esteem 6th | 0.47 | 0.48 | 11.11 | <0.001 | −0.460 |
| Self-esteem 6th -> Self-esteem 7th | 0.49 | 0.49 | 11.64 | <0.001 | −3.092 * |
| Self-esteem 7th -> Self-esteem 8th | 0.50 | 0.50 | 12.67 | <0.001 | −2.608 * |
| Depression 1st -> Self-esteem 2nd | −0.01 | −0.02 | 0.39 | 0.699 | 0.050 |
| Depression 2nd -> Self-esteem 3rd | −0.17 | −0.10 | −2.25 | 0.025 | 0.381 |
| Depression 3rd -> Self-esteem 4th | −0.01 | −0.01 | −0.24 | 0.972 | 0.496 |
| Depression 4th -> Self-esteem 5th | −0.26 | −0.17 | −1.65 | 0.049 | −0.852 |
| Depression 5th -> Self-esteem 6th | −0.05 | −0.07 | −1.61 | 0.108 | 1.148 |
| Depression 6th -> Self-esteem 7th | −0.01 | −0.01 | −0.24 | 0.813 | −0.453 |
| Depression 7th -> Self-esteem 8th | −0.01 | −0.01 | −0.29 | 0.771 | −1.608 |
| Self-esteem 1st -> Depression 2nd | −0.17 | −0.13 | −2.69 | 0.007 | −1.794 |
| Self-esteem 2nd -> Depression 3rd | −0.06 | −0.05 | −0.97 | 0.332 | −1.323 |
| Self-esteem 3rd -> Depression 4th | −0.25 | −0.17 | −3.60 | <0.001 | −0.626 |
| Self-esteem 4th -> Depression 5th | −0.06 | −0.17 | −1.09 | 0.275 | 0.808 |
| Self-esteem 5th -> Depression 6th | −0.17 | −0.16 | −1.71 | 0.040 | −0.343 |
| Self-esteem 6th -> Depression 7th | −0.09 | −0.08 | −1.75 | 0.081 | −0.409 |
| Self-esteem 7th -> Depression 8th | –0.04 | –0.03 | –0.79 | 0.429 | –1.794 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, J.-W.; Kim, D.-J. Longitudinal Relationship Study of Depression and Self-Esteem in Postnatal Korean Women Using Autoregressive Cross-Lagged Modeling. Int. J. Environ. Res. Public Health 2020, 17, 3743. https://doi.org/10.3390/ijerph17103743
Han J-W, Kim D-J. Longitudinal Relationship Study of Depression and Self-Esteem in Postnatal Korean Women Using Autoregressive Cross-Lagged Modeling. International Journal of Environmental Research and Public Health. 2020; 17(10):3743. https://doi.org/10.3390/ijerph17103743
Chicago/Turabian StyleHan, Jeong-Won, and Da-Jung Kim. 2020. "Longitudinal Relationship Study of Depression and Self-Esteem in Postnatal Korean Women Using Autoregressive Cross-Lagged Modeling" International Journal of Environmental Research and Public Health 17, no. 10: 3743. https://doi.org/10.3390/ijerph17103743