Association Between Gout and Injury Risk: A National Retrospective Cohort Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Study Design
2.3. Data Analysis
3. Results
3.1. Sample Size
3.2. Baseline Characteristics
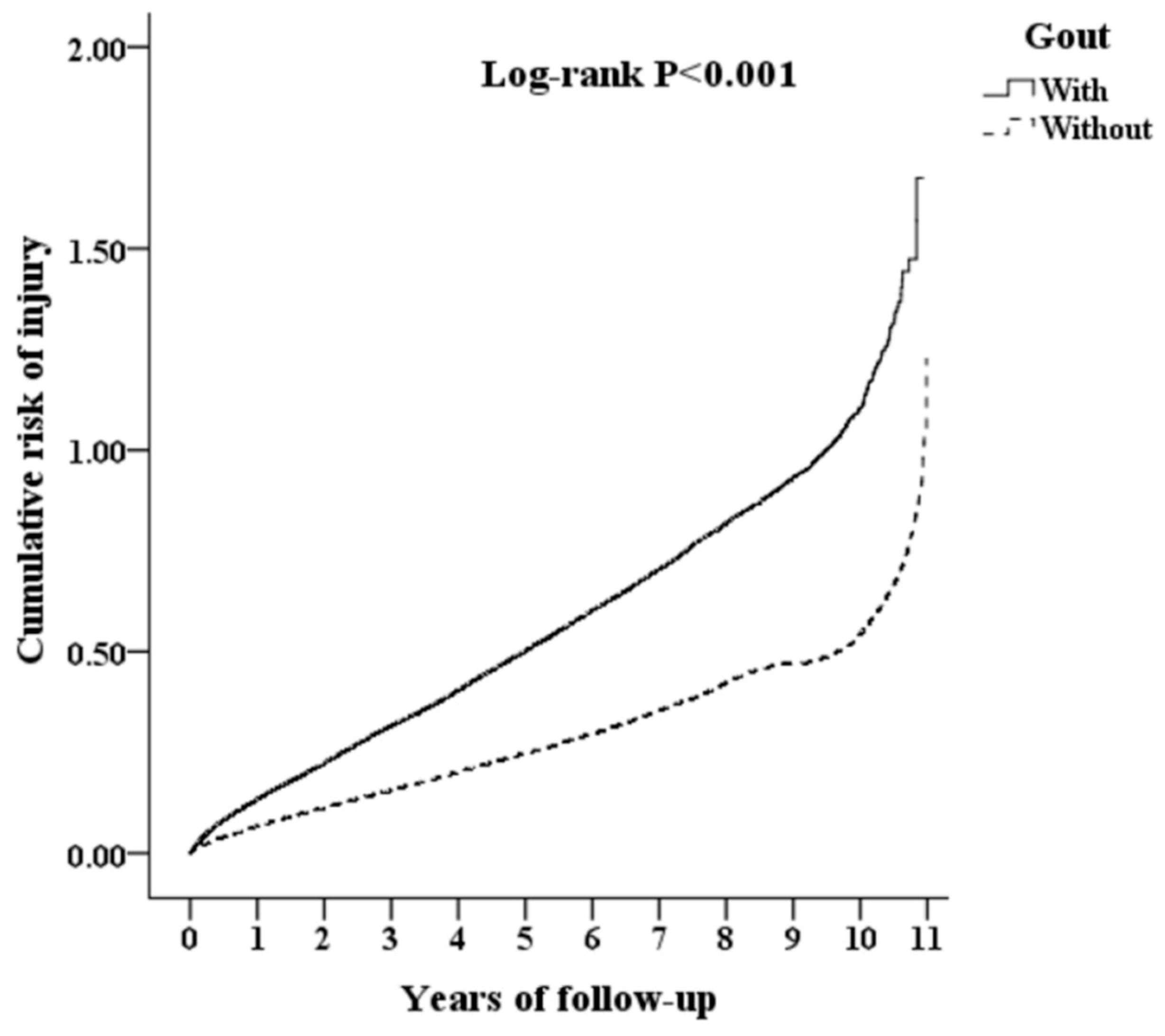
3.3. Differences in Injuries between Groups CFG and C at the End of Follow-Up
3.4. Risk Factors for the Occurrence of Injuries
3.5. Factors for the Occurrence of Injuries by Cox Regression Analysis
3.6. Relationship between the Occurrence of Subgroup Injuries and Gout
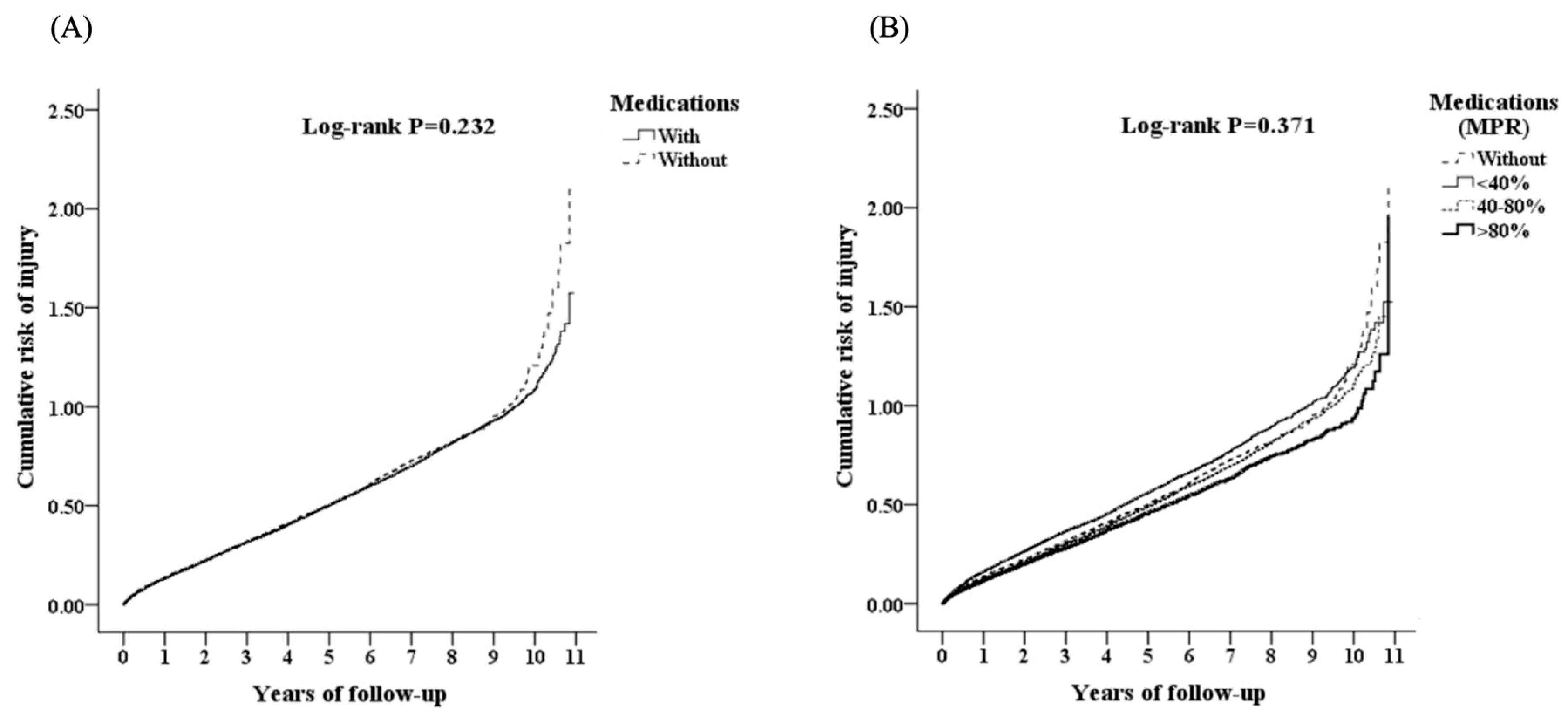
3.7. Difference in the Occurrence of Injuries in Group CFG with Medication (M) and without Medication (NM)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Kuo, C.F.; Grainge, M.J.; Zhang, W.; Doherty, M. Global epidemiology of gout: Prevalence, incidence and risk factors. Nat. Rev. Rheumatol. 2015, 11, 649–662. [Google Scholar] [CrossRef]
- Joo, K.; Kwon, S.R.; Lim, M.J.; Jung, K.H.; Joo, H.; Park, W. Prevention of comorbidity and acute attack of gout by uric acid lowering therapy. J. Korean Med. Sci. 2014, 29, 657–661. [Google Scholar] [CrossRef] [Green Version]
- Wandell, P.; Carlsson, A.C.; Ljunggren, G. Gout and its comorbidities in the total population of Stockholm. Prev. Med. 2015, 81, 387–391. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, S.S.; Victora, C.G.; Halpern, R.; Barros, A.J.; Lima, R.C.; Monteiro, L.A.; Barros, F. Risk factors for accidental injuries in preschool children. J. Pediatr. 2002, 78, 97–104. [Google Scholar] [CrossRef]
- Zhang, H.; Wei, F.; Han, M.; Chen, J.; Peng, S.; Du, Y. Risk factors for unintentional injuries among the rural elderly: A county-based cross-sectional survey. Sci. Rep. 2017, 7, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuo, C.F.; Luo, S.F. Gout: Risk of premature death in gout unchanged for years. Nat. Rev. Rheumatol. 2017, 13, 200. [Google Scholar] [CrossRef] [PubMed]
- Lalli, P.; Chan, A.; Garven, A.; Midha, N.; Chan, C.; Brady, S.; Block, E.; Hu, B.; Toth, C. Increased gait variability in diabetes mellitus patients with neuropathic pain. J. Diabetes Complicat. 2013, 27, 248–254. [Google Scholar] [CrossRef] [PubMed]
- Avin, K.G.; Moorthi, R.N. Bone is not alone: The effects of skeletal muscle dysfunction in chronic kidney disease. Curr. Osteoporos. Rep. 2015, 13, 173–179. [Google Scholar] [CrossRef] [Green Version]
- Choi, H.J.; Lee, C.H.; Lee, J.H.; Yoon, B.Y.; Kim, H.A.; Suh, C.H.; Choi, S.T.; Song, J.S.; Joo, H.; Choi, S.J.; et al. Seasonality of gout in Korea: A multicenter study. J. Korean Med. Sci. 2015, 30, 240–244. [Google Scholar] [CrossRef] [Green Version]
- Elliot, A.J.; Cross, K.W.; Fleming, D.M. Seasonality and trends in the incidence and prevalence of gout in England and Wales 1994–2007. Ann. Rheum. Dis. 2009, 68, 1728–1733. [Google Scholar] [CrossRef]
- Åkerblom, A.; Helmersson-Karlqvist, J.; Weitoft, T.; Larsson, A. Seasonal variations of urate in a Swedish adult population. Clin. Rheumatol. 2017, 36, 1595–1598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuo, C.F.; Grainge, M.J.; See, L.C.; Yu, K.H.; Luo, S.F.; Zhang, W.; Doherty, M. Epidemiology and management of gout in Taiwan: A nationwide population study. Arthritis Res. Ther. 2015, 17, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Odden, M.C.; Amadu, A.R.; Smit, E.; Lo, L.; Peralta, C.A. Uric acid levels, kidney function, and cardiovascular mortality in US adults: National Health and Nutrition Examination Survey (NHANES) 1988–1994 and 1999–2002. Am. J. Kidney Dis. 2014, 64, 550–557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharaf El Din, U.A.A.; Salem, M.M.; Abdulazim, D.O. Uric acid in the pathogenesis of metabolic, renal, and cardiovascular diseases: A review. J. Adv. Res. 2017, 8, 537–548. [Google Scholar] [CrossRef]
- Cristóbal-García, M.; García-Arroyo, F.E.; Tapia, E.; Osorio, H.; Arellano-Buendía, A.S.; Madero, M.; Rodríguez-Iturbe, B.; Pedraza-Chaverrí, J.; Correa, F.; Zazueta, C.; et al. Renal oxidative stress induced by long-term hyperuricemia alters mitochondrial function and maintains systemic hypertension. Oxid. Med. Cell. Longev. 2015, 2015, 535686. [Google Scholar] [CrossRef] [Green Version]
- Cai, W.; Duan, X.M.; Liu, Y.; Yu, J.; Tang, Y.L.; Liu, Z.L.; Jiang, S.; Zhang, C.P.; Liu, J.Y.; Xu, J.X. Uric acid induces endothelial dysfunction by activating the HMGB1/RAGE signaling pathway. Biomed. Res. Int. 2017. [Google Scholar] [CrossRef]
- Kanbay, M.; Segal, M.; Afsar, B.; Kang, D.H.; Rodriguez-Iturbe, B.; Johnson, R.J. The role of uric acid in the pathogenesis of human cardiovascular disease. Heart 2013, 99, 759–766. [Google Scholar] [CrossRef] [Green Version]
- Johnson, R.J.; Bakris, G.L.; Borghi, C.; Chonchol, M.B.; Feldman, D.; Lanaspa, M.A.; Merriman, T.R.; Moe, O.W.; Mount, D.B.; Lozada, L.G.; et al. Hyperuricemia, acute and chronic kidney disease, hypertension, and cardiovascular disease: Report of a scientific workshop organized by the National Kidney Foundation. Am. J. Kidney Dis. 2018, 71, 851–865. [Google Scholar] [CrossRef]
- Stewart, S.; Dalbeth, N.; Vandal, A.C.; Rome, K. The first metatarsophalangeal joint in gout: A systematic review and meta-analysis. BMC Musculoskelet. Disord. 2016, 17, 69. [Google Scholar] [CrossRef] [Green Version]
- López-Soto, P.J.; De Giorgi, A.; Senno, E.; Tiseo, R.; Ferraresi, A.; Canella, C.; Rodríguez-Borrego, M.A.; Manfredini, R.; Fabbian, F. Renal disease and accidental falls: A review of published evidence. BMC Nephrol. 2015, 16, 176. [Google Scholar] [CrossRef] [Green Version]
- Kwan, M.M.; Close, J.C.; Wong, A.K.; Lord, S.R. Falls incidence, risk factors, and consequences in Chinese older people: A systematic review. J. Am. Geriatr. Soc. 2011, 59, 536–543. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.; Zhang, H.; Ma, A. Association of gout and depression: A systematic review and meta-analysis. Int. J. Geriatr. Psychiatry 2018, 33, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Igel, T.F.; Krasnokutsky, S.; Pillinger, M.H. Recent advances in understanding and managing gout. F1000Research 2017, 6, 247. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Gout | Total | Group CFG | Group C | p Value | ||||
|---|---|---|---|---|---|---|---|---|
| Variables | n | % | n | % | n | % | ||
| Total | 257,442 | 85,814 | 33.33 | 171,628 | 66.67 | |||
| Sex | 0.999 | |||||||
| Male | 206,907 | 80.37 | 68,969 | 80.37 | 137,938 | 80.37 | ||
| Female | 50,535 | 19.63 | 16,845 | 19.63 | 33,690 | 19.63 | ||
| Age (Years) (Mean ± SD) | 64.15 ± 16.69 | 63.90 ± 16.13 | 64.28 ± 16.97 | 0.041 | ||||
| Season | <0.001 | |||||||
| Spring (March–May) | 62,939 | 24.45 | 19,672 | 22.92 | 43,267 | 25.21 | ||
| Summer (June–August) | 64,590 | 25.09 | 21,974 | 25.61 | 42,616 | 24.83 | ||
| Autumn (September–November) | 68,327 | 26.54 | 24,952 | 29.08 | 43,375 | 25.27 | ||
| Winter (December–February) | 61,586 | 23.92 | 19,216 | 22.39 | 42,370 | 24.69 | ||
| Location | <0.001 | |||||||
| Northern Taiwan | 101,639 | 39.48 | 32,547 | 37.93 | 69,092 | 40.26 | ||
| Central Taiwan | 73,304 | 28.47 | 24,929 | 29.05 | 48,375 | 28.19 | ||
| Southern Taiwan | 64,734 | 25.15 | 21,637 | 25.21 | 43,097 | 25.11 | ||
| Eastern Taiwan | 16,564 | 6.43 | 6208 | 7.23 | 10,356 | 6.03 | ||
| Outlying islands | 1201 | 0.47 | 493 | 0.57 | 708 | 0.41 | ||
| Insured Premium (NT$) | 0.001 | |||||||
| <15,840 | 253,900 | 98.62 | 84,517 | 98.49 | 169,383 | 98.69 | ||
| 15,841–25,000 | 2832 | 1.10 | 1077 | 1.26 | 1755 | 1.02 | ||
| ≥25,001 | 710 | 0.28 | 220 | 0.26 | 490 | 0.29 | ||
| Diabetes Mellitus (DM) | <0.001 | |||||||
| Without | 212,846 | 82.68 | 69,797 | 81.34 | 143,049 | 83.35 | ||
| With | 44,596 | 17.32 | 16,017 | 18.66 | 28,579 | 16.65 | ||
| Hypertension | <0.001 | |||||||
| Without | 197,472 | 76.71 | 56,906 | 66.31 | 140,566 | 81.90 | ||
| With | 59,970 | 23.29 | 28,908 | 33.69 | 31,062 | 18.10 | ||
| Stroke | <0.001 | |||||||
| Without | 233,003 | 90.51 | 77,098 | 89.84 | 155,905 | 90.84 | ||
| With | 24,441 | 9.49 | 8718 | 10.16 | 15,723 | 9.16 | ||
| Chronic Renal Disease | <0.001 | |||||||
| Without | 248,622 | 96.57 | 82,486 | 96.12 | 166,136 | 96.80 | ||
| With | 8820 | 3.43 | 3328 | 3.88 | 5492 | 3.20 | ||
| Coronary Artery Disease (CAD) | <0.001 | |||||||
| Without | 230,456 | 89.52 | 75,336 | 87.79 | 155,120 | 90.38 | ||
| With | 26,986 | 10.48 | 10,478 | 12.21 | 16,508 | 9.62 | ||
| Gout | Total | Group CFG | Group C | p Value | ||||
|---|---|---|---|---|---|---|---|---|
| Variables | n | % | n | % | n | % | ||
| Total | 257,442 | 85,814 | 33.33 | 171,628 | 66.67 | |||
| Injury | <0.001 | |||||||
| Without | 210,610 | 81.81 | 69,576 | 81.08 | 141,034 | 82.17 | ||
| With | 46,832 | 18.19 | 16,238 | 18.92 | 30,594 | 17.83 | ||
| Cause of injury | <0.001 | |||||||
| Traffic Injuries | 6615 | 14.12 | 2141 | 13.19 | 4474 | 14.62 | ||
| Poisoning | 586 | 1.25 | 234 | 1.44 | 352 | 1.15 | ||
| Falls | 10,044 | 21.45 | 3322 | 20.46 | 6722 | 21.97 | ||
| Burns and Fires | 73 | 0.16 | 19 | 0.12 | 54 | 0.18 | ||
| Drowning | 9 | 0.02 | 3 | 0.02 | 6 | 0.02 | ||
| Suffocation | 217 | 0.46 | 68 | 0.42 | 149 | 0.49 | ||
| Crushing/Cutting/Piercing | 1452 | 3.10 | 512 | 3.15 | 940 | 3.07 | ||
| Excessive Heat | 12 | 0.03 | 4 | 0.02 | 8 | 0.03 | ||
| Injury Caused by Animals | 96 | 0.03 | 44 | 0.05 | 52 | 0.03 | ||
| Electric Current Injury | 21 | 0.04 | 4 | 0.02 | 17 | 0.06 | ||
| Other Unintentional Injuries | 9472 | 20.23 | 3768 | 23.20 | 5704 | 18.64 | ||
| Suicide | 555 | 1.19 | 179 | 1.10 | 376 | 1.23 | ||
| Homicide/Abuse | 449 | 0.96 | 140 | 0.86 | 309 | 1.01 | ||
| Intention Unknown | 305 | 0.65 | 110 | 0.68 | 195 | 0.64 | ||
| No Provided E-Code | 16,926 | 36.14 | 5690 | 35.04 | 11,236 | 36.73 | ||
| Injury Severity Score (ISS) ≥ 16 | <0.001 | |||||||
| Without | 257,056 | 99.85 | 85,631 | 99.79 | 171,425 | 99.88 | ||
| With | 386 | 0.15 | 183 | 0.21 | 203 | 0.12 | ||
| Variables | Crude HR | 95% CI | 95% CI | p | Adjusted HR | 95% CI | 95% CI | p |
|---|---|---|---|---|---|---|---|---|
| Gout | ||||||||
| Without | Reference | Reference | ||||||
| With | 1.992 | 1.953 | 2.031 | <0.001 | 2.034 | 1.995 | 2.074 | <0.001 |
| Sex | ||||||||
| Male | 0.912 | 0.892 | 0.932 | <0.001 | 0.889 | 0.869 | 0.909 | <0.001 |
| Female | Reference | Reference | ||||||
| Age (Years) | 0.989 | 0.988 | 0.990 | <0.001 | 0.993 | 0.992 | 0.994 | <0.001 |
| Diabetes Mellitus (DM) | ||||||||
| Without | Reference | Reference | ||||||
| With | 0.856 | 0.836 | 0.876 | <0.001 | 0.894 | 0.873 | 0.916 | <0.001 |
| Hypertension | ||||||||
| Without | Reference | Reference | ||||||
| With | 0.751 | 0.735 | 0.768 | <0.001 | 0.787 | 0.769 | 0.806 | <0.001 |
| Stroke | ||||||||
| Without | Reference | Reference | ||||||
| With | 0.618 | 0.596 | 0.642 | <0.001 | 0.649 | 0.626 | 0.674 | <0.001 |
| Chronic Renal Disease | ||||||||
| Without | Reference | Reference | ||||||
| With | 1.484 | 1.422 | 1.548 | <0.001 | 1.302 | 1.247 | 1.360 | <0.001 |
| Coronary Artery Disease (CAD) | ||||||||
| Without | Reference | Reference | ||||||
| With | 0.612 | 0.592 | 0.633 | <0.001 | 0.661 | 0.639 | 0.685 | <0.001 |
| Season | ||||||||
| Spring (March–May) | Reference | Reference | ||||||
| Summer (June–August) | 0.944 | 0.920 | 0.968 | <0.001 | 0.932 | 0.909 | 0.956 | <0.001 |
| Autumn (September–November) | 0.813 | 0.792 | 0.834 | <0.001 | 0.803 | 0.783 | 0.824 | <0.001 |
| Winter (December–February) | 0.911 | 0.887 | 0.935 | <0.001 | 0.919 | 0.896 | 0.943 | <0.001 |
| Location | ||||||||
| Northern Taiwan | Reference | Reference | ||||||
| Central Taiwan | 1.228 | 1.201 | 1.256 | <0.001 | 1.169 | 1.143 | 1.196 | <0.001 |
| Southern Taiwan | 1.215 | 1.186 | 1.243 | <0.001 | 1.184 | 1.156 | 1.212 | <0.001 |
| Eastern Taiwan | 1.314 | 1.268 | 1.361 | <0.001 | 1.201 | 1.159 | 1.245 | <0.001 |
| Outlying Islands | 1.313 | 1.156 | 1.492 | <0.001 | 1.174 | 1.033 | 1.334 | 0.014 |
| Insured premium (NT$) | ||||||||
| <15,840 | Reference | Reference | ||||||
| 15,841–25,000 | 0.980 | 0.903 | 1.063 | 0.622 | 0.899 | 0.828 | 0.975 | 0.010 |
| ≥25,001 | 0.718 | 0.572 | 0.902 | 0.004 | 0.622 | 0.495 | 0.782 | <0.001 |
| Gout | Group CFG | Group C | Ratio | Adjusted HR | 95%CI | 95%CI | p | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variables | Event | PYs | Rate (per 105 PYs) | Event | PYs | Rate (per 105 PYs) | ||||||
| Total | 16,238 | 150,342.08 | 10,800.70 | 30,594 | 322,350.39 | 9490.91 | 1.138 | 2.034 | 1.995 | 2.074 | <0.0011 | |
| Sex | ||||||||||||
| Male | 12,534 | 118,736.14 | 10,556.18 | 23,960 | 256,463.93 | 9342.44 | 1.130 | 2.021 | 1.976 | 2.066 | <0.001 | |
| Female | 3704 | 31,605.94 | 11,719.32 | 6634 | 65,886.46 | 10,068.84 | 1.164 | 2.077 | 1.993 | 2.165 | <0.001 | |
| Diabetes mellitus (DM) | ||||||||||||
| Without | 13,201 | 116,597.02 | 11,321.90 | 24,862 | 254,643.69 | 9763.45 | 1.160 | 2.082 | 2.037 | 2.127 | <0.001 | |
| With | 3037 | 33,745.06 | 8999.84 | 5732 | 67,706.70 | 8465.93 | 1.063 | 1.834 | 1.753 | 1.919 | <0.001 | |
| Hypertension | ||||||||||||
| Without | 11,736 | 98,684.39 | 11,892.46 | 24,703 | 238,757.71 | 10,346.47 | 1.149 | 2.000 | 1.955 | 2.045 | <0.001 | |
| With | 4502 | 51,657.69 | 8715.06 | 5891 | 83,592.68 | 7047.27 | 1.237 | 2.184 | 2.097 | 2.274 | <0.001 | |
| Stroke | ||||||||||||
| Without | 15,258 | 134,176.20 | 11,371.61 | 28,531 | 284,544.60 | 10,026.90 | 1.134 | 2.060 | 2.019 | 2.103 | <0.001 | |
| With | 980 | 16,165.88 | 6062.15 | 2063 | 37,805.79 | 5456.84 | 1.111 | 1.667 | 1.542 | 1.802 | <0.001 | |
| Chronic renal disease | ||||||||||||
| Without | 15,325 | 143,313.20 | 10,693.36 | 29,281 | 307,574.55 | 9519.97 | 1.123 | 2.076 | 2.035 | 2.119 | <0.001 | |
| With | 913 | 7028.89 | 12,989.25 | 1313 | 14,775.84 | 8886.13 | 1.462 | 1.492 | 1.368 | 1.627 | <0.001 | |
| Coronary artery disease (CAD) | ||||||||||||
| Without | 14,873 | 129,957.13 | 11,444.54 | 28332 | 284,501.30 | 9958.48 | 1.149 | 2.039 | 1.998 | 2.082 | <0.001 | |
| With | 1365 | 20,384.95 | 6696.12 | 2262 | 37,849.09 | 5976.37 | 1.120 | 1.940 | 1.810 | 2.079 | <0.001 | |
| Season | ||||||||||||
| Spring (March–May) | 3967 | 33,203.35 | 11,947.59 | 7760 | 75,299.86 | 10,305.46 | 1.159 | 2.061 | 1.981 | 2.143 | <0.001 | |
| Summer (June–August) | 4271 | 37,283.12 | 11,455.59 | 7792 | 80,649.66 | 9661.54 | 1.186 | 2.096 | 2.016 | 2.178 | <0.001 | |
| Autumn (September–November) | 4326 | 45,283.44 | 9553.16 | 7590 | 89,206.10 | 8508.39 | 1.123 | 1.985 | 1.910 | 2.063 | <0.001 | |
| Winter (December–February) | 3674 | 34,572.18 | 10,627.04 | 7452 | 77,194.77 | 9653.50 | 1.101 | 1.999 | 1.919 | 2.082 | <0.001 | |
| Location | ||||||||||||
| Northern Taiwan | 5326 | 55,338.61 | 9624.38 | 10,761 | 127,610.68 | 8432.68 | 1.141 | 2.074 | 2.004 | 2.145 | <0.001 | |
| Central Taiwan | 5147 | 44,678.27 | 11,520.14 | 9259 | 91,204.09 | 10,151.96 | 1.135 | 2.082 | 2.010 | 2.156 | <0.001 | |
| Southern Taiwan | 4277 | 37,643.40 | 11,361.89 | 8075 | 79,540.46 | 10,152.07 | 1.119 | 1.967 | 1.894 | 2.043 | <0.001 | |
| Eastern Taiwan | 1391 | 11,782.55 | 11,805.59 | 2357 | 21,562.39 | 10,931.07 | 1.080 | 1.932 | 1.804 | 2.069 | <0.001 | |
| Outlying Islands | 97 | 899.26 | 10,786.65 | 142 | 2432.78 | 5836.94 | 1.848 | 1.779 | 1.358 | 2.330 | <0.001 | |
| Insured premium (NT$) | ||||||||||||
| <15,840 | 15,975 | 147,884.48 | 10,802.35 | 30,197 | 317,543.94 | 9509.55 | 1.136 | 2.029 | 1.989 | 2.069 | <0.001 | |
| 15,841–25,000 | 238 | 2122.27 | 11,214.41 | 348 | 4087.90 | 8512.93 | 1.317 | 2.539 | 2.136 | 3.020 | <0.001 | |
| ≥25,001 | 25 | 335.33 | 7455.34 | 49 | 718.56 | 6819.19 | 1.093 | 2.946 | 1.695 | 5.121 | <0.001 | |
| Gout | Group CFG | Group C | Ratio | Adjusted HR | 95%CI | 95%CI | p | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Subgroups of Injury | Event | PYs | Rate (per 10 5 PYs) | Event | PYs | Rate (per 10 5 PYs) | ||||||
| Total | 16,238 | 150,342.08 | 10,800.70 | 30,594 | 322,350.39 | 9,490.91 | 1.138 | 2.034 | 1.995 | 2.074 | <0.001 | |
| Cause of injury | ||||||||||||
| Traffic injuries | 2141 | 150,342.08 | 1424.09 | 4,74 | 322,350.39 | 1387.93 | 1.026 | 1.575 | 1.494 | 1.861 | <0.001 | |
| Poisoning | 234 | 150,342.08 | 155.65 | 352 | 322,350.39 | 109.20 | 1.425 | 1.650 | 1.382 | 1.970 | <0.001 | |
| Falls | 3322 | 150,342.08 | 2209.63 | 6722 | 322,350.39 | 2085.31 | 1.060 | 1.743 | 1.670 | 1.820 | <0.001 | |
| Burns and fires | 19 | 150,342.08 | 12.64 | 54 | 322,350.39 | 16.75 | 0.754 | 0.637 | 0.215 | 8.189 | 0.721 | |
| Drowning | 3 | 150,342.08 | 2.00 | 6 | 322,350.39 | 1.86 | 1.072 | 1.022 | 0.674 | 3.571 | 0.166 | |
| Suffocation | 68 | 150,342.08 | 45.23 | 149 | 322,350.39 | 46.22 | 0.979 | 0.942 | 0.328 | 2.554 | 0.402 | |
| Crushing/Cutting/Piercing | 512 | 150,342.08 | 340.56 | 940 | 322,350.39 | 291.61 | 1.168 | 1.879 | 1.662 | 2.123 | <0.001 | |
| Excessive Heat | 4 | 150,342.08 | 2.66 | 8 | 322,350.39 | 2.48 | 1.072 | 1.145 | 0.976 | 2.447 | 0.435 | |
| Injury Caused by Animals | 44 | 150,342.08 | 29.27 | 52 | 322,350.39 | 16.13 | 1.814 | 1.976 | 1.013 | 3.001 | 0.026 | |
| Electric Current Injury | 4 | 150,342.08 | 2.66 | 17 | 322,350.39 | 5.27 | 0.504 | 0.976 | 0.432 | 1.434 | 0.556 | |
| Other Unintentional Injuries | 3768 | 150,342.08 | 2506.28 | 5704 | 322,350.39 | 1769.50 | 1.416 | 1.511 | 1.126 | 2.138 | <0.001 | |
| Suicide | 179 | 150,342.08 | 119.06 | 376 | 322,350.39 | 116.64 | 1.021 | 1.506 | 1.247 | 1.820 | <0.001 | |
| Homicide/Abuse | 140 | 150,342.08 | 93.12 | 309 | 322,350.39 | 95.86 | 0.971 | 0.618 | 0.301 | 1.012 | 0.058 | |
| Intention Unknown | 110 | 150,342.08 | 73.17 | 195 | 322,350.39 | 60.49 | 1.209 | 1.447 | 1.119 | 1.876 | 0.005 | |
| No Provided E-Code | 5690 | 150,342.08 | 3784.70 | 11,236 | 322,350.39 | 3485.65 | 1.086 | 1.473 | 1.426 | 1.552 | <0.001 | |
| Injury Severity Score (ISS) ≥16 | ||||||||||||
| Without | 16,055 | 150,342.08 | 10,678.98 | 30,391 | 322,350.39 | 9427.94 | 1.133 | 2.025 | 1.986 | 2.066 | <0.001 | |
| With | 183 | 150,342.08 | 121.72 | 203 | 322,350.39 | 62.97 | 1.933 | 2.114 | 1.692 | 2.641 | <0.001 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ou, S.-H.; Chou, C.-L.; Lin, C.-W.; Chien, W.-C.; Fang, T.-C.; Lu, K.-C.; Chen, J.-S. Association Between Gout and Injury Risk: A National Retrospective Cohort Study. Int. J. Environ. Res. Public Health 2020, 17, 3679. https://doi.org/10.3390/ijerph17103679
Ou S-H, Chou C-L, Lin C-W, Chien W-C, Fang T-C, Lu K-C, Chen J-S. Association Between Gout and Injury Risk: A National Retrospective Cohort Study. International Journal of Environmental Research and Public Health. 2020; 17(10):3679. https://doi.org/10.3390/ijerph17103679
Chicago/Turabian StyleOu, Shih-Hsiang, Chu-Lin Chou, Chia-Wei Lin, Wu-Chien Chien, Te-Chao Fang, Kuo-Cheng Lu, and Jin-Shuen Chen. 2020. "Association Between Gout and Injury Risk: A National Retrospective Cohort Study" International Journal of Environmental Research and Public Health 17, no. 10: 3679. https://doi.org/10.3390/ijerph17103679