Optimizing the Interaction of Exercise Volume and Metformin to Induce a Clinically Significant Reduction in Metabolic Syndrome Severity: A Randomised Trial

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
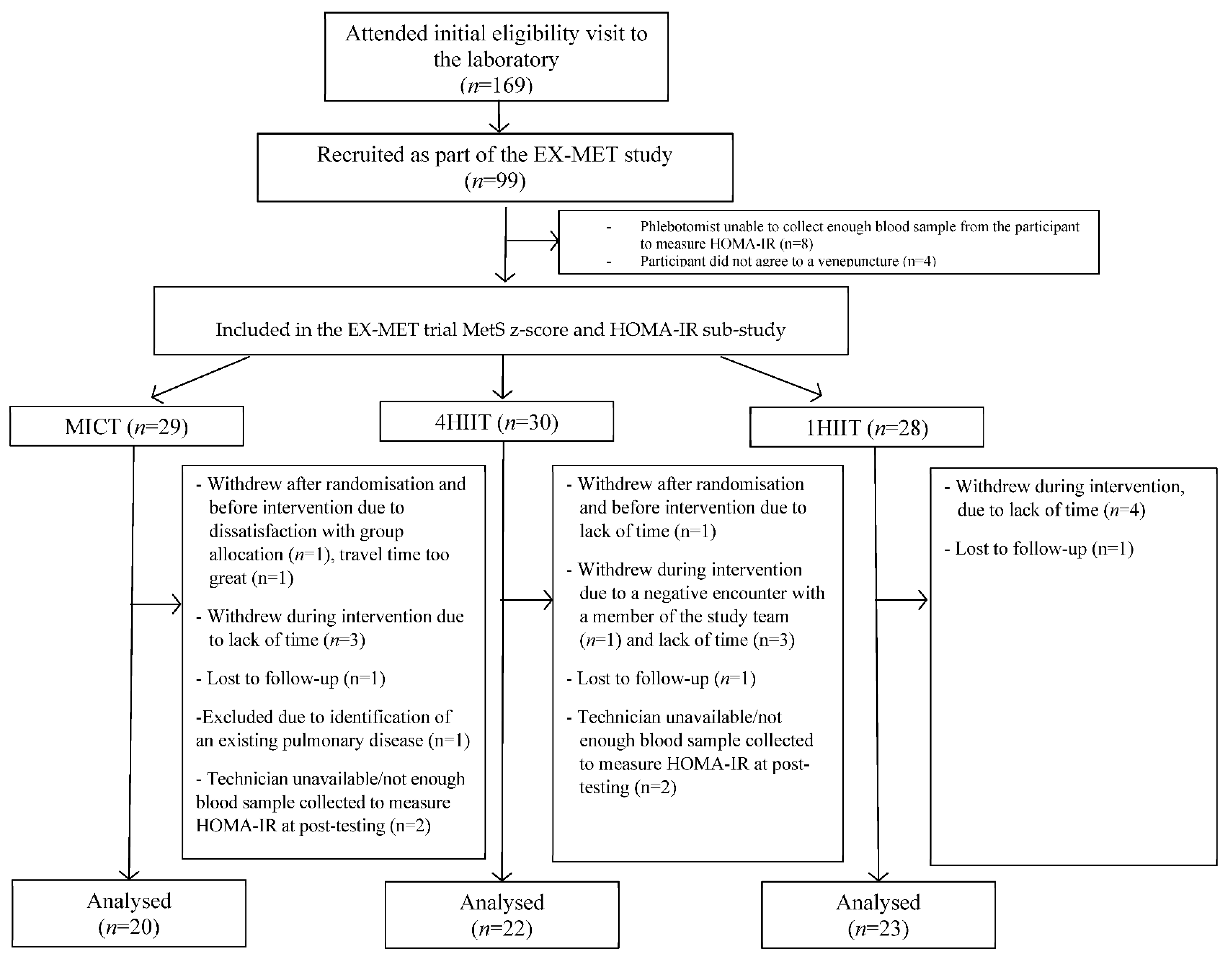
2.1. Participants and Study Design
2.2. Metabolic Syndrome Severity and Insulin Resistance
2.3. Cardiorespiratory Fitness (CRF)
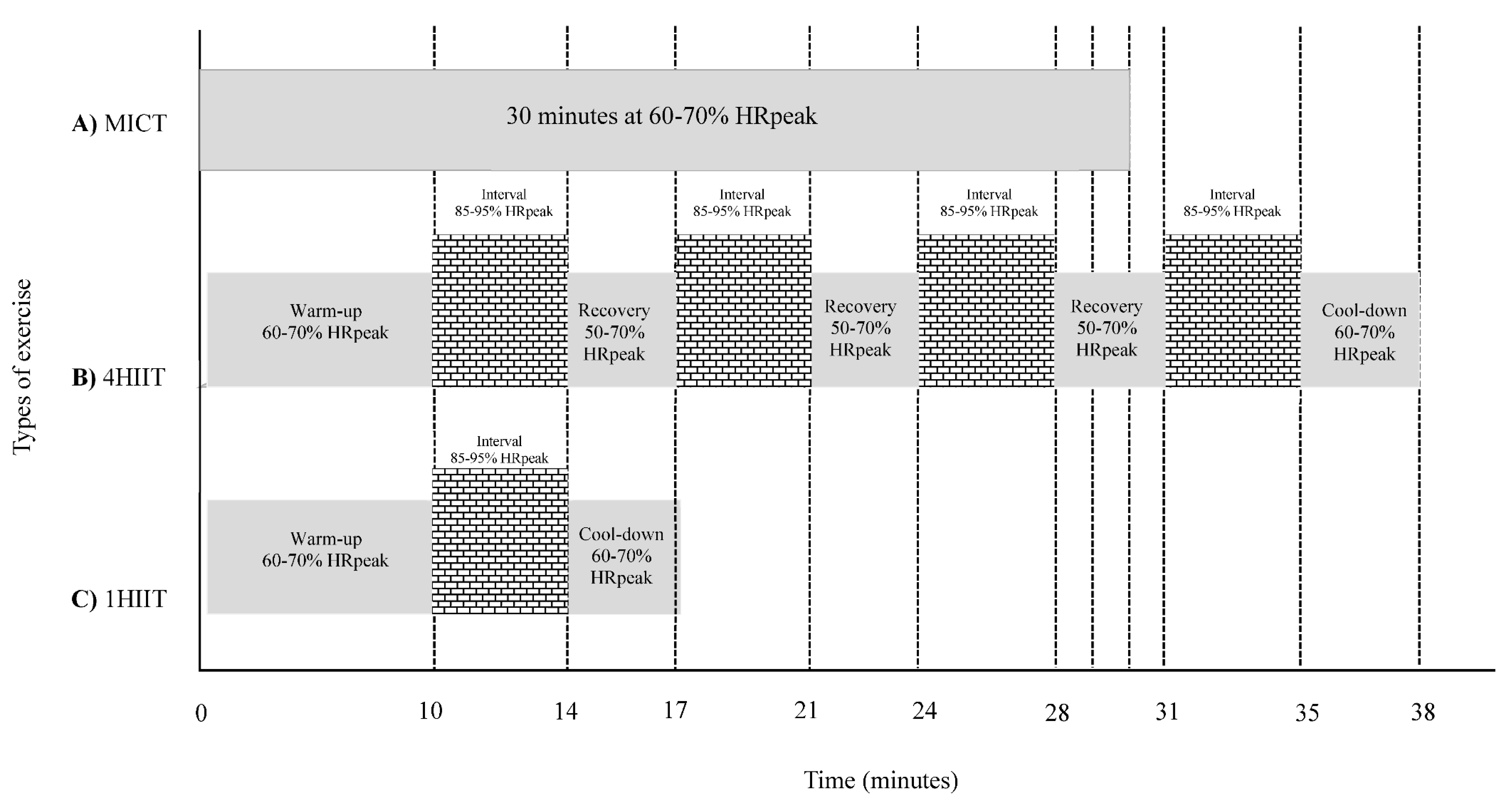
2.4. Training Protocol
2.5. Statistical Analysis
3. Results
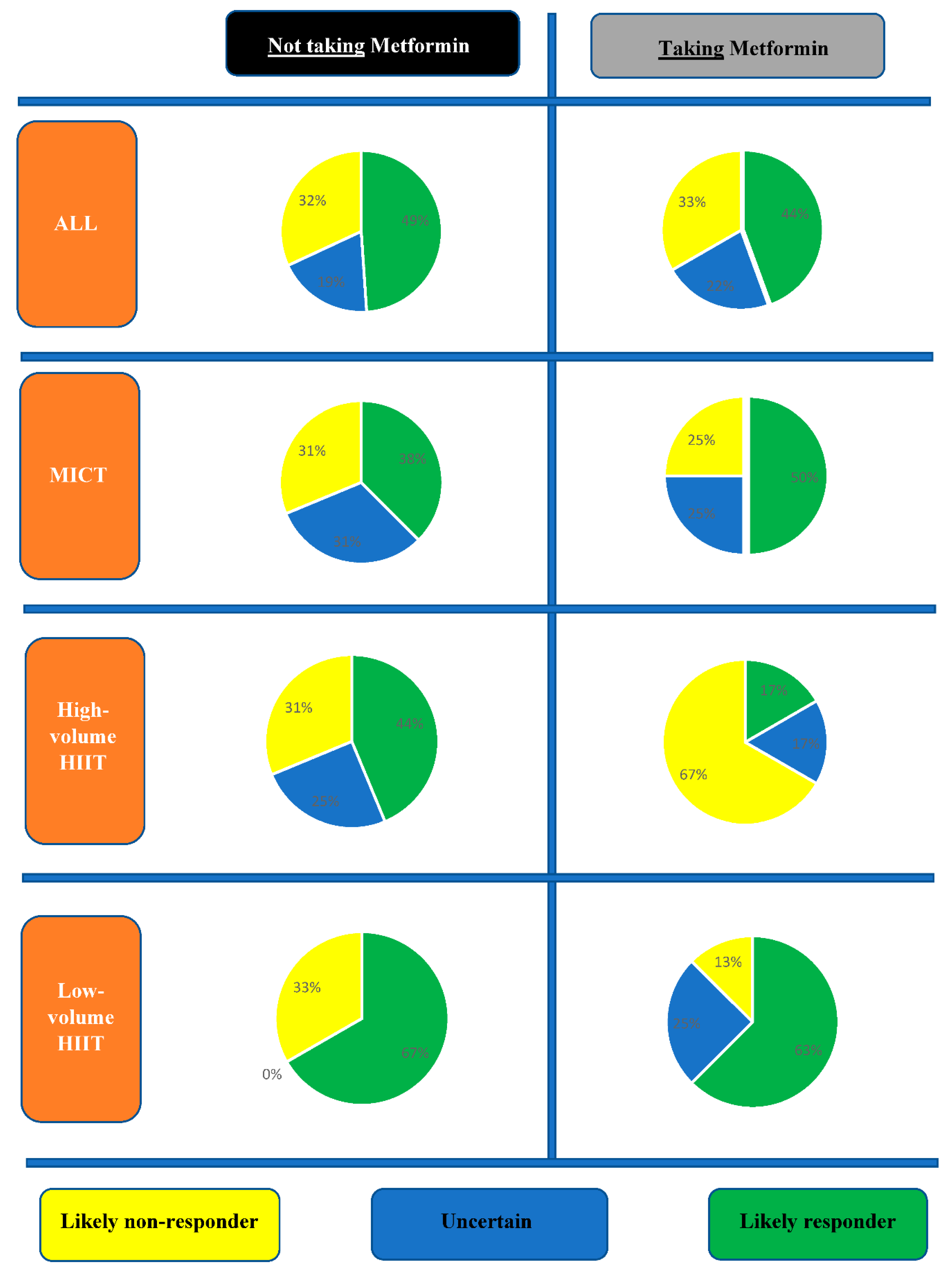
3.1. Inter-Individual Variability in MetS Severity Change
3.2. Inter-Individual Variability in Cardiorespiratory Fitness Changes
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C., Jr. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reaven, G.M. Insulin resistance, the insulin resistance syndrome, and cardiovascular disease. Panminerva Med. 2005, 47, 201–210. [Google Scholar] [PubMed]
- Knowler, W.C.; Barrett-Connor, E.; Fowler, S.E.; Hamman, R.F.; Lachin, J.M.; Walker, E.A.; Nathan, D.M. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N. Engl. J. Med. 2002, 346, 393–403. [Google Scholar] [CrossRef] [PubMed]
- Pattyn, N.; Cornelissen, V.A.; Eshghi, S.R.; Vanhees, L. The effect of exercise on the cardiovascular risk factors constituting the metabolic syndrome: A meta-analysis of controlled trials. Sports Med. 2013, 43, 121–133. [Google Scholar] [CrossRef] [Green Version]
- Delamater, A. Improving patient adherence. Clin. Diabetes J. 2012, 24, 71–77. [Google Scholar] [CrossRef] [Green Version]
- Iuga, A.O.; McGuire, M.J. Adherence and health care costs. Risk Manag. Healthc. Policy 2014, 7, 35. [Google Scholar]
- Nathan, D.M.; Buse, J.B.; Davidson, M.B.; Ferrannini, E.; Holman, R.R.; Sherwin, R.; Zinman, B. Medical management of hyperglycemia in type 2 diabetes: A consensus algorithm for the initiation and adjustment of therapy: A consensus statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care 2009, 32, 193–203. [Google Scholar] [CrossRef] [Green Version]
- Cheng, A.; Canadian Diabetes Association Clinical Practice Guidelines Expert Committee. Canadian Diabetes Association 2013 clinical practice guidelines for the prevention and management of diabetes in Canada. Introduction. Can. J. Diabetes 2013, 37, S1. [Google Scholar] [CrossRef] [Green Version]
- Boule, N.G. Exercise Plus Metformin in the Fight Against Diabetes. Exerc. Sport Sci. Rev. 2016, 44, 2. [Google Scholar] [CrossRef]
- Rena, G.; Lang, C.C. Repurposing Metformin for Cardiovascular Disease. Circulation 2018, 137, 422–424. [Google Scholar] [CrossRef] [Green Version]
- Katzmarzyk, P.T.; Church, T.S.; Blair, S.N. Cardiorespiratory fitness attenuates the effects of the metabolic syndrome on all-cause and cardiovascular disease mortality in men. Arch. Intern. Med. 2004, 164, 1092–1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malin, S.K.; Braun, B. Impact of Metformin on Exercise-Induced Metabolic Adaptations to Lower Type 2 Diabetes Risk. Exerc. Sport Sci. Rev. 2016, 44, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Earnest, C.P.; Artero, E.G.; Sui, X.; Lee, D.C.; Church, T.S.; Blair, S.N. Maximal estimated cardiorespiratory fitness, cardiometabolic risk factors, and metabolic syndrome in the aerobics center longitudinal study. Mayo Clin. Proc. 2013, 88, 259–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeBoer, M.D.; Filipp, S.L.; Gurka, M.J. Use of a Metabolic Syndrome Severity Z Score to Track Risk During Treatment of Prediabetes: An Analysis of the Diabetes Prevention Program. Diabetes Care 2018, 41, 2421–2430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malin, S.K.; Nightingale, J.; Choi, S.E.; Chipkin, S.R.; Braun, B. Metformin modifies the exercise training effects on risk factors for cardiovascular disease in impaired glucose tolerant adults. Obesity 2013, 21, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.L.; Slentz, C.A.; Houmard, J.A.; Samsa, G.P.; Duscha, B.D.; Aiken, L.B.; McCartney, J.S.; Tanner, C.J.; Kraus, W.E. Exercise training amount and intensity effects on metabolic syndrome (from Studies of a Targeted Risk Reduction Intervention through Defined Exercise). Am. J. Cardiol. 2007, 100, 1759–1766. [Google Scholar] [CrossRef] [Green Version]
- Tjonna, A.E.; Ramos, J.S.; Pressler, A.; Halle, M.; Jungbluth, K.; Ermacora, E.; Salvesen, O.; Rodrigues, J.; Bueno, C.R., Jr.; Munk, P.S.; et al. EX-MET study: Exercise in prevention on of metabolic syndrome-a randomized multicenter trial: Rational and design. BMC Public Health 2018, 18, 437. [Google Scholar] [CrossRef]
- Gurka, M.J.; Lilly, C.L.; Oliver, M.N.; DeBoer, M.D. An examination of sex and racial/ethnic differences in the metabolic syndrome among adults: A confirmatory factor analysis and a resulting continuous severity score. Metabolism 2014, 63, 218–225. [Google Scholar] [CrossRef] [Green Version]
- TOCfD, D.T.U. Endocrinology and Metabolism HOMA2 Calculator. Ph.D. Thesis, The University of Oxford, Oxford, UK, 2011. [Google Scholar]
- Fletcher, G.F.; Balady, G.J.; Amsterdam, E.A.; Chaitman, B.; Eckel, R.; Fleg, J.; Froelicher, V.F.; Leon, A.S.; Pina, I.L.; Rodney, R.; et al. Exercise standards for testing and training: A statement for healthcare professionals from the American Heart Association. Circulation 2001, 104, 1694–1740. [Google Scholar] [CrossRef] [Green Version]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- Hecksteden, A.; Pitsch, W.; Rosenberger, F.; Meyer, T. Repeated testing for the assessment of individual response to exercise training. J. Appl. Physiol. 2018, 124, 1567–1579. [Google Scholar] [CrossRef] [PubMed]
- Weatherwax, R.M.; Ramos, J.S.; Harris, N.K.; Kilding, A.E.; Dalleck, L.C. Changes in Metabolic Syndrome Severity Following Individualized Versus Standardized Exercise Prescription: A Feasibility Study. Int. J. Environ. Res. Public Health 2018, 15, 2594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Konopka, A.R.; Laurin, J.L.; Schoenberg, H.M.; Reid, J.J.; Castor, W.M.; Wolff, C.A.; Musci, R.V.; Safairad, O.D.; Linden, M.A.; Biela, L.M.; et al. Metformin inhibits mitochondrial adaptations to aerobic exercise training in older adults. Aging Cell 2019, 18, e12880. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tonkonogi, M.; Walsh, B.; Svensson, M.; Sahlin, K. Mitochondrial function and antioxidative defence in human muscle: Effects of endurance training and oxidative stress. J. Physiol. 2000, 528 Pt 2, 379–388. [Google Scholar] [CrossRef]
- Jeppesen, J.; Jordy, A.B.; Sjoberg, K.A.; Fullekrug, J.; Stahl, A.; Nybo, L.; Kiens, B. Enhanced fatty acid oxidation and FATP4 protein expression after endurance exercise training in human skeletal muscle. PLoS ONE 2012, 7, e29391. [Google Scholar] [CrossRef] [Green Version]
- Vincent, G.; Lamon, S.; Gant, N.; Vincent, P.J.; MacDonald, J.R.; Markworth, J.F.; Edge, J.A.; Hickey, A.J. Changes in mitochondrial function and mitochondria associated protein expression in response to 2-weeks of high intensity interval training. Front. Physiol. 2015, 6, 51. [Google Scholar] [CrossRef] [Green Version]
- Perry, C.G.; Lally, J.; Holloway, G.P.; Heigenhauser, G.J.; Bonen, A.; Spriet, L.L. Repeated transient mRNA bursts precede increases in transcriptional and mitochondrial proteins during training in human skeletal muscle. J. Physiol. 2010, 588, 4795–4810. [Google Scholar] [CrossRef]
- Brunmair, B.; Staniek, K.; Gras, F.; Scharf, N.; Althaym, A.; Clara, R.; Roden, M.; Gnaiger, E.; Nohl, H.; Waldhausl, W.; et al. Thiazolidinediones, like metformin, inhibit respiratory complex I: A common mechanism contributing to their antidiabetic actions? Diabetes 2004, 53, 1052–1059. [Google Scholar] [CrossRef] [Green Version]
- Wessels, B.; Ciapaite, J.; van den Broek, N.M.; Nicolay, K.; Prompers, J.J. Metformin impairs mitochondrial function in skeletal muscle of both lean and diabetic rats in a dose-dependent manner. PLoS ONE 2014, 9, e100525. [Google Scholar] [CrossRef] [Green Version]
- Alshawi, A.; Agius, L. Low metformin causes a more oxidized mitochondrial NADH/NAD redox state in hepatocytes and inhibits gluconeogenesis by a redox-independent mechanism. J. Biol. Chem. 2019, 294, 2839–2853. [Google Scholar] [CrossRef] [Green Version]
- Madiraju, A.K.; Erion, D.M.; Rahimi, Y.; Zhang, X.-M.; Braddock, D.T.; Albright, R.A.; Prigaro, B.J.; Wood, J.L.; Bhanot, S.; MacDonald, M.J. Metformin suppresses gluconeogenesis by inhibiting mitochondrial glycerophosphate dehydrogenase. Nature 2014, 510, 542–546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boulé, N.G.; Robert, C.; Bell, G.J.; Johnson, S.T.; Bell, R.C.; Lewanczuk, R.Z.; Gabr, R.Q.; Brocks, D.R. Metformin and exercise in type 2 diabetes: Examining treatment modality interactions. Diabetes Care 2011, 34, 1469–1474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malin, S.K.; Stephens, B.R.; Sharoff, C.G.; Hagobian, T.A.; Chipkin, S.R.; Braun, B. Metformin’s effect on exercise and postexercise substrate oxidation. Int. J. Sport Nutr. Exerc. Metab. 2010, 20, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Andreadis, E.A.; Katsanou, P.M.; Georgiopoulos, D.X.; Tsourous, G.I.; Yfanti, G.K.; Gouveri, E.T.; Diamantopoulos, E.J. The effect of metformin on the incidence of type 2 diabetes mellitus and cardiovascular disease risk factors in overweight and obese subjects--the Carmos study. Exp. Clin. Endocrinol. Diabetes 2009, 117, 175–180. [Google Scholar] [CrossRef] [PubMed]
- Gurka, M.J.; Filipp, S.L.; Pearson, T.A.; DeBoer, M.D. Assessing Baseline and Temporal Changes in Cardiometabolic Risk Using Metabolic Syndrome Severity and Common Risk Scores. J. Am. Heart Assoc. 2018, 7, e009754. [Google Scholar] [CrossRef] [Green Version]
- Ramos, J.S.; Dalleck, L.C.; Tjonna, A.E.; Beetham, K.S.; Coombes, J.S. The impact of high-intensity interval training versus moderate-intensity continuous training on vascular function: A systematic review and meta-analysis. Sports Med. 2015, 45, 679–692. [Google Scholar] [CrossRef]
- Weston, K.S.; Wisloff, U.; Coombes, J.S. High-intensity interval training in patients with lifestyle-induced cardiometabolic disease: A systematic review and meta-analysis. Br. J. Sports Med. 2014, 48, 1227–1234. [Google Scholar] [CrossRef]
- Cassidy, S.; Thoma, C.; Houghton, D.; Trenell, M.I. High-intensity interval training: A review of its impact on glucose control and cardiometabolic health. Diabetologia 2017, 60, 7–23. [Google Scholar] [CrossRef] [Green Version]
- Tjonna, A.E.; Lee, S.J.; Rognmo, O.; Stolen, T.O.; Bye, A.; Haram, P.M.; Loennechen, J.P.; Al-Share, Q.Y.; Skogvoll, E.; Slordahl, S.A.; et al. Aerobic interval training versus continuous moderate exercise as a treatment for the metabolic syndrome: A pilot study. Circulation 2008, 118, 346–354. [Google Scholar] [CrossRef] [Green Version]
- Halperin, I.; Emanuel, A. Rating of Perceived Effort: Methodological Concerns and Future Directions. Sports Med. 2020, 50, 679–687. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Participant Characteristics/Outcome Variable | Not taking Metformin (n = 47) | Taking Metformin (n = 18) | |||
|---|---|---|---|---|---|
| Baseline | Post | Baseline | Post | Between Group Diff (p-Value) | |
| Age (year) | 56 ± 9 | -- | 59 ± 7 | -- | 0.13 |
| T2D, % | 17 | -- | 100 | -- | <0.001 |
| Body mass (kg) | 96 ± 19 | 94 ± 19 | 98 ± 20 | 97 ± 20 | 0.61 |
| BMI (kg/m2) | 32 ± 5 | 32 ± 5 | 33 ± 6 | 32 ± 6 | 0.59 |
| Waist circumference (cm) | 104 ± 12 | 102 ± 11 | 108 ± 12 | 105 ± 12 | 0.82 |
| Systolic BP (mm Hg) | 132 ± 13 | 124 ± 10 | 133 ± 13 | 130 ± 13 | 0.03 |
| Diastolic BP (mm Hg) | 85 ± 9 | 81 ± 7 | 82 ± 7 | 79 ± 8 | 0.55 |
| Triglycerides (mmol/L) | 1.9 ± 1.0 | 1.8 ± 0.9 | 2.0 ± 0.7 | 1.9 ± 1.0 | 0.88 |
| HDL-C (mmol/L) | 1.2 ± 0.4 | 1.2 ± 0.4 | 1.0 ± 0.2 | 1.1 ± 0.3 | 0.83 |
| Glucose (mmol/L) | 5.9 ± 1.2# | 5.8 ± 1.3 | 8.3 ± 2.5 | 7.9 ± 2.4 | 0.48 |
| HOMA-IR | 2.3 ± 1.1 | 1.9 ± 1.1 | 1.9 ± 0.9 | 1.6 ± 0.8 | 0.79 |
| MetS z-score | 1.6 ± 2.3# | 0.8 ± 2.1 | 4.2 ± 2.5 | 3.0 ± 3.2 | 0.81 |
| VO2peak (mL/kg/min) | 26.4 ± 6.6 | 28.4 ± 6.9 | 24.9 ± 6.6 | 27.4 ± 6.6 | 0.78 |
| Participant Characteristics/Outcome Variable | MICT (n = 16) | 4HIIT (n = 16) | 1HIIT (n = 15) | ||||
|---|---|---|---|---|---|---|---|
| Baseline | Post | Baseline | Post | Baseline | Post | Between Group Difference (p-Value) | |
| Age (year) | 56 ± 9 | -- | 55 ± 10 | -- | 57 ± 9 | -- | 0.72 |
| T2D, % | 6 | -- | 19 | -- | 27 | -- | 0.31 |
| Body mass (kg) | 99 ± 20 | 98 ± 21 | 97 ± 16 | 96 ± 16 | 91 ± 20 | 89 ± 19 | 0.81 |
| BMI (kg/m2) | 32 ± 6 | 32 ± 6 | 33 ± 4 | 33 ± 4 | 30 ± 5 | 30 ± 4 | 0.87 |
| Waist circumference (cm) | 107 ± 13 | 105 ± 14 | 104 ± 10 | 103 ± 8 | 102 ± 13 | 99 ± 11 | 0.43 |
| Systolic BP (mm Hg) | 131 ± 15 | 124 ± 10 | 131 ± 12 | 126 ± 11 | 133 ± 13 | 123 ± 10 | 0.26 |
| Diastolic BP (mm Hg) | 87 ± 11 | 82 ± 8 | 85 ± 7 | 81 ± 7 | 83 ± 7 | 80 ± 4 | 0.86 |
| Triglycerides (mmol/L) | 1.7 ± 0.8 | 1.7 ± 1.0 | 2.4 ± 1.3 | 2.1 ± 1.1 | 1.7 ± 0.7 | 1.6 ± 0.6 | 0.81 |
| HDL-C (mmol/L) | 1.2 ± 0.4 | 1.2 ± 0.3 | 1.0 ± 0.4 | 1.2 ± 0.4 | 1.2 ± 0.5 | 1.3 ± 0.5 | 0.39 |
| Glucose (mmol/L) | 5.8 ± 0.8 | 5.5 ± 0.6 | 6.0 ± 1.9 | 6.1 ± 1.9 | 5.8 ± 0.9 | 5.9 ± 0.7 | 0.24 |
| HOMA-IR | 2.4 ± 1.4 | 1.8 ± 1.2 | 2.2 ± 1.0 | 1.8 ± 0.8 | 2.2 ± 1.0 | 2.2 ± 1.3 | 0.17 |
| MetS z-score | 1.5 ± 2.0 | 0.6 ± 1.9 | 2.1 ± 2.6 | 1.3 ± 2.6 | 1.3 ± 2.3 | 0.3 ± 1.7 | 0.60 |
| VO2peak (mL/kg/min) | 27.9 ± 7.3 | 28.9 ± 6.7 | 24.5 ± 4.5 | 27.9 ± 6.5 | 26.4 ± 7.5 | 28.3 ± 7.8 | 0.39 |
| Outcome Variable | MICT (n = 4) | 4HIIT (n = 6) | 1HIIT (n = 8) | ||||
|---|---|---|---|---|---|---|---|
| Baseline | Post | Baseline | Post | Baseline | Post | Between Group Difference (p-Value) | |
| Age (year) | 63 ± 6 | -- | 58 ± 9 | -- | 58 ± 4 | -- | 0.44 |
| T2D, % | 100 | -- | 100 | -- | 100 | -- | >0.05 |
| Body mass (kg) | 103 ± 11 | 98 ± 15 | 102 ± 20 | 101 ± 20 | 93 ± 24 | 92 ± 24 | 0.46 |
| BMI (kg/m2) | 33 ± 4 | 32 ± 4 | 34 ± 7 | 34 ± 8 | 32 ± 7 | 31 ± 7 | 0.73 |
| Waist circumference (cm) | 111 ± 9 | 107 ± 9 | 109 ± 12 | 107 ± 14 | 105 ± 13 | 102 ± 13 | 0.56 |
| Systolic BP (mm Hg) | 136 ± 10 | 129 ± 15 | 123 ± 8 | 129 ± 6 | 138 ± 14 | 132 ± 18 | 0.14 |
| Diastolic BP (mm Hg) | 84 ± 5 | 78 ± 7 | 82 ± 7 | 79 ± 7 | 80 ± 7 | 79 ± 10 | 0.94 |
| Triglycerides (mmol/L) | 1.8 ± 0.7 | 1.3 ± 0.4 | 2.0 ± 0.9 | 2.3 ± 1.5 | 2.1 ± 0.7 | 1.8 ± 0.6 | 0.17 |
| HDL-C (mmol/L) | 1.0 ± 0.4 | 1.1 ± 0.5 | 0.9 ± 0.2 | 0.9 ± 0.02 | 1.0 ± 0.2 | 1.2 ± 0.2 | 0.13 |
| Glucose (mmol/L) | 6.4 ± 1.0 | 6.9 ± 2.3 | 8.6 ± 3.0 | 8.5 ± 2.3 | 9.1 ± 2.4 | 8.1 ± 2.8 | 0.64 |
| HOMA-IR | 1.7 ± 0.8 | 1.3 ± 0.7 | 1.9 ± 0.7 | 1.9 ± 0.8 | 1.9 ± 1.1 | 1.5 ± 0.9 | 0.12 |
| MetS z-score | 2.7 ± 1.3 | 1.7 ± 2.6 | 4.3 ± 1.9 | 4.2 ± 1.9 | 4.8 ± 3.2 | 2.8 ± 4.1 | 0.26 |
| VO2peak (mL/kg/min) | 25.6 ± 8.6 | 25.9 ± 6.6 | 24.7 ± 8.7 | 28.8 ± 9.6 | 24.6 ± 4.4 | 27.1 ± 4.3 | 0.33 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramos, J.S.; Dalleck, L.C.; Keith, C.E.; Fennell, M.; Lee, Z.; Drummond, C.; Keating, S.E.; Fassett, R.G.; Coombes, J.S. Optimizing the Interaction of Exercise Volume and Metformin to Induce a Clinically Significant Reduction in Metabolic Syndrome Severity: A Randomised Trial. Int. J. Environ. Res. Public Health 2020, 17, 3695. https://doi.org/10.3390/ijerph17103695
Ramos JS, Dalleck LC, Keith CE, Fennell M, Lee Z, Drummond C, Keating SE, Fassett RG, Coombes JS. Optimizing the Interaction of Exercise Volume and Metformin to Induce a Clinically Significant Reduction in Metabolic Syndrome Severity: A Randomised Trial. International Journal of Environmental Research and Public Health. 2020; 17(10):3695. https://doi.org/10.3390/ijerph17103695
Chicago/Turabian StyleRamos, Joyce S., Lance C. Dalleck, Caitlin E. Keith, Mackenzie Fennell, Zoe Lee, Claire Drummond, Shelley E. Keating, Robert G. Fassett, and Jeff S. Coombes. 2020. "Optimizing the Interaction of Exercise Volume and Metformin to Induce a Clinically Significant Reduction in Metabolic Syndrome Severity: A Randomised Trial" International Journal of Environmental Research and Public Health 17, no. 10: 3695. https://doi.org/10.3390/ijerph17103695