Health-Risk Behaviours and Injuries among Youth and Young Adults in Chiang Mai, Thailand: A Population-Based Survey

 , ,
, ,
Abstract
:1. Introduction
2. Material and Methods
2.1. The Dataset
2.2. Variables and Measurements
2.3. Statistical Analysis
2.4. Ethics Approval
3. Results
3.1. Study Participants
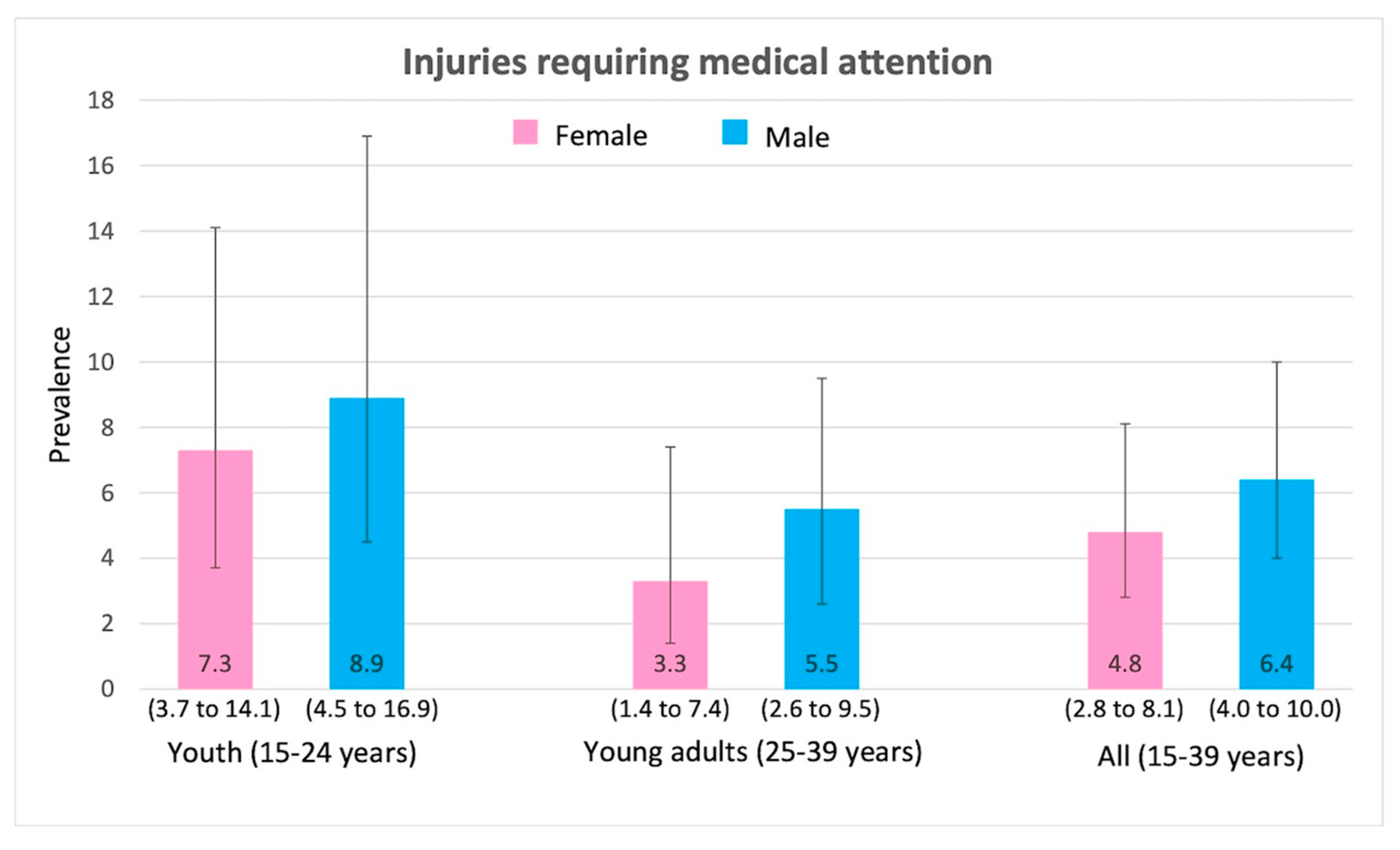
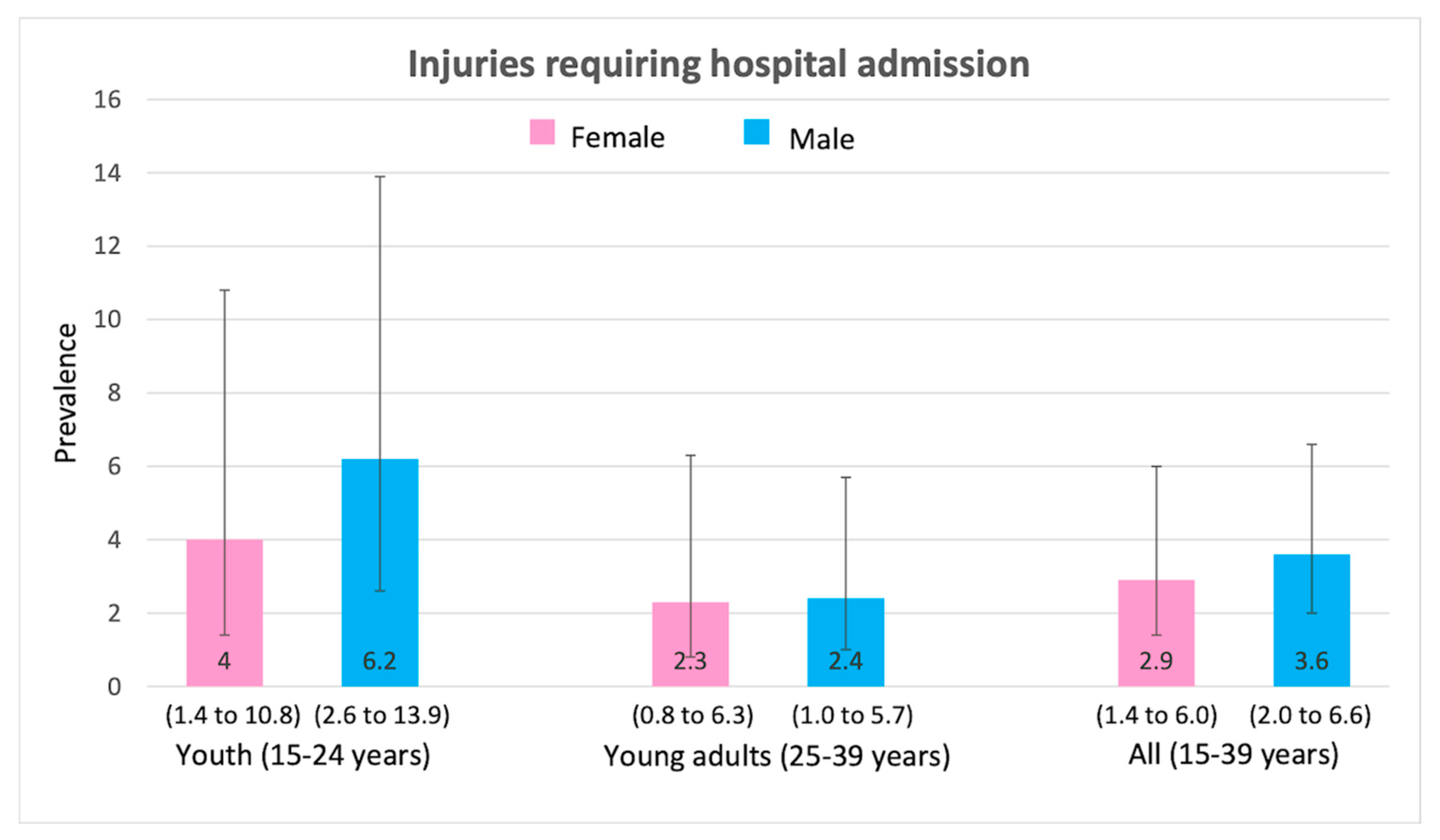
3.2. Prevalence of Health-Risk Behaviours and Injuries
3.3. Health-Risk Behaviours and Injuries
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- GBD 2017 Causes of Death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef] [Green Version]
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [Green Version]
- Yiengprugsawan, V.; Stephan, K.; McClure, R.; Kelly, M.; Seubsman, S.; Bain, C.; Sleigh, A.C. Risk factors for injury in a national cohort of 87,134 Thai adults. Public Health 2012, 126, 33–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ditsuwan, V.; Veerman, L.J.; Barendregt, J.J.; Bertram, M.; Vos, T. The national burden of road traffic injuries in Thailand. Popul. Health Metr. 2011, 9, 2. [Google Scholar] [CrossRef] [Green Version]
- Chadbunchachai, W.; Suphanchaimaj, W.; Settasatien, A.; Jinwong, T. Road traffic injuries in Thailand: Current situation. J. Med. Assoc. Thai. 2012, 95, S274–S281. [Google Scholar]
- Yiengprugsawan, V.; Berecki-Gisolf, J.; Bain, C.; McClure, R.; Seubsman, S.-A.; Sleigh, A.C.; Thai Cohort Study, T. Predictors of injury mortality: Findings from a large national cohort in Thailand. BMJ Open 2014, 4, e004668. [Google Scholar] [CrossRef]
- Dos Santos Silva, R.J.; Soares, N.M.M.; Cabral de Oliveira, A.C. Factors associated with violent behavior among adolescents in northeastern Brazil. Sci. World J. 2014, 2014, 863918. [Google Scholar] [CrossRef]
- Pickett, W.; Schmid, H.; Boyce, W.F.; Simpson, K.; Scheidt, P.C.; Mazur, J.; Aszmann, A. Multiple risk behavior and injury: An international analysis of young people. Arch. Pediatr. Adolesc. Med. 2002, 156, 786–793. [Google Scholar] [CrossRef]
- Kann, L.; McManus, T.; Harris, W.A.; Shanklin, S.L.; Flint, K.H.; Queen, B.; Lowry, R.; Chyen, D.; Whittle, L.; Thornton, J.; et al. Youth Risk Behavior Surveillance—United States, 2017. Morb. Mortal. Wkly. Report Surveill. Summ. 2018, 67, 1–114. [Google Scholar] [CrossRef]
- Cremonte, M.; Cherpitel, C.J. Alcohol intake and risk of injury. Medicina 2014, 74, 287–292. [Google Scholar]
- Taylor, B.; Irving, H.M.; Kanteres, F.; Room, R.; Borges, G.; Cherpitel, C.; Greenfield, T.; Rehm, J. The more you drink, the harder you fall: A systematic review and meta-analysis of how acute alcohol consumption and injury or collision risk increase together. Drug Alcohol Depend. 2010, 110, 108–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, K.-C.; Kim, S.A.; Kim, N.R.; Shin, M.-H. Association between Smoking and Unintentional Injuries among Korean Adults. Chonnam Med. J. 2018, 54, 184–189. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.; Heinz, A. Alcohol-related aggression-social and neurobiological factors. Dtsch. Arztebl. Int. 2013, 110, 711–715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Field, M.; Wiers, R.W.; Christiansen, P.; Fillmore, M.T.; Verster, J.C. Acute alcohol effects on inhibitory control and implicit cognition: Implications for loss of control over drinking. Alcohol. Clin. Exp. Res. 2010, 34, 1346–1352. [Google Scholar] [CrossRef] [PubMed]
- Rehm, J. The risks associated with alcohol use and alcoholism. Alcohol Res. Health 2011, 34, 135–143. [Google Scholar]
- Vingilis, E.; Pederson, L.L.; Seeley, J.; Ialomiteanu, A.R.; Wickens, C.M.; Ferrence, R.; Mann, R.E. Is there a link between motor vehicle collisions and being a cigarette smoker in Canada? Analysis of survey data from Ontario from 2002 to 2014. Traffic Inj. Prev. 2018, 19, 364–370. [Google Scholar] [CrossRef]
- Pederson, L.L.; Koval, J.; Vingilis, E.; Seeley, J.; Ialomiteanu, A.R.; Wickens, C.M.; Ferrence, R.; Mann, R.E. The relationship between motor vehicle collisions and cigarette smoking in Ontario: Analysis of CAMH survey data from 2002 to 2016. Prev. Med. Rep. 2019, 13, 327–331. [Google Scholar] [CrossRef]
- Sacks, J.J.; Nelson, D.E. Smoking and injuries: An overview. Prev. Med. 1994, 23, 515–520. [Google Scholar] [CrossRef]
- Latvala, T.; Lintonen, T.; Konu, A. Public health effects of gambling—Debate on a conceptual model. BMC Public Health 2019, 19, 1077. [Google Scholar] [CrossRef] [Green Version]
- Abbott, M.; Bellringer, M.; Garrett, N.; Mundy-McPherson, S. New Zealand 2012 National Gambling Study: Gambling Harm and Problem Gambling; Auckland University of Technology: Auckland, New Zealand, 2014. [Google Scholar]
- Roberts, A.; Coid, J.; King, R.; Murphy, R.; Turner, J.; Bowden-Jones, H.; Du Preez, K.P.; Landon, J. Gambling and violence in a nationally representative sample of UK men. Addiction 2016, 111, 2196–2207. [Google Scholar] [CrossRef] [Green Version]
- Slavin, M.; Pilver, C.E.; Hoff, R.A.; Krishnan-Sarin, S.; Steinberg, M.A.; Rugle, L.; Potenza, M.N. Serious physical fighting and gambling-related attitudes and behaviors in adolescents. J. Behav. Addict. 2013, 2, 167. [Google Scholar] [CrossRef] [Green Version]
- Zhai, Z.W.; Hoff, R.A.; Magruder, C.F.; Steinberg, M.A.; Wampler, J.; Krishnan-Sarin, S.; Potenza, M.N. Weapon-carrying is associated with more permissive gambling attitudes and perceptions and at-risk/problem gambling in adolescents. J. Behav. Addict. 2019, 8, 508–521. [Google Scholar] [CrossRef]
- Dowling, N.; Suomi, A.; Jackson, A.; Lavis, T.; Patford, J.; Cockman, S.; Thomas, S.; Bellringer, M.; Koziol-Mclain, J.; Battersby, M.; et al. Problem gambling and intimate partner violence: A systematic review and meta-analysis. Trauma Violence Abuse 2016, 17, 43–61. [Google Scholar] [CrossRef] [Green Version]
- Assanangkornchai, S.; McNeil, E.B.; Tantirangsee, N.; Kittirattanapaiboon, P. Gambling disorders, gambling type preferences, and psychiatric comorbidity among the Thai general population: Results of the 2013 National Mental Health Survey. J. Behav. Addict. 2016, 5, 410–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagata, J.M.; Ferguson, B.J.; Ross, D.A. Research priorities for eight areas of adolescent health in low- and middle-income countries. J. Adolesc. Health 2016, 59, 50–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagata, J.M.; Hathi, S.; Ferguson, B.J.; Hindin, M.J.; Yoshida, S.; Ross, D.A. Research priorities for adolescent health in low- and middle-income countries: A mixed-methods synthesis of two separate exercises. J. Glob. Health 2018, 8, 010501. [Google Scholar] [CrossRef] [PubMed]
- Assanangkornchai, S.; Saingam, D.; Jitpiboon, W.; Geater, A.F. Comparison of drinking prevalence among Thai youth before and after implementation of the Alcoholic Beverage Control Act. Am. J. Drug Alcohol Abuse 2020, 1–8. [Google Scholar] [CrossRef]
- Intarut, N.; Sangthong, R.; Chongsuvivatwong, V. Smoking trends among Thailand’syouths from 1996-2015: An age-period-cohort analysis of national health surveys. Iran J. Public Health 2019, 48, 429–434. [Google Scholar]
- Sirirassamee, T.; Sirirassamee, B. Health risk behavior among Thai youth: National survey 2013. Asia Pac. J. Public Health 2014, 27, 76–84. [Google Scholar] [CrossRef]
- Angkurawaranon, C.; Pateekhum, C.; Thaikla, K. Probability sampling in population-based behavioral health surveys: Lessons from Thailand. In SAGE Research Methods Cases; SAGE: London, UK, 2020. [Google Scholar]
- Pinyopornpanish, K.; Thanamee, S.; Jiraporncharoen, W.; Thaikla, K.; McDonald, J.; Aramrattana, A.; Angkurawaranon, C. Sexual health, risky sexual behavior and condom use among adolescents young adults and older adults in Chiang Mai, Thailand: Findings from a population based survey. BMC Res. Notes 2017, 10, 682. [Google Scholar] [CrossRef] [Green Version]
- Thanamee, S.; Pinyopornpanish, K.; Wattanapisit, A.; Suerungruang, S.; Thaikla, K.; Jiraporncharoen, W.; Angkurawaranon, C. A population-based survey on physical inactivity and leisure time physical activity among adults in Chiang Mai, Thailand, 2014. Arch. Public Health 2017, 75, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. The Alcohol, Smoking and Substance Involvement Screening Test (ASSIST): Manual for use in Primary Care; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Aekplakorn, W.; Nitiyanant, W.; Sornpaisarn, B.; Khananuraksa, P. Bureau of Non Communicble Disease Ministry of Public Health. Thai National Health Examination Survey, NHES V. Available online: http://kb.hsri.or.th/dspace/handle/11228/4604?locale-attribute=th (accessed on 30 March 2020).
- Babor, T.F.; Higgins-Biddle, J.C.; Saunders, J.B.; Monteiro, M.G. AUDIT The Alcohol Use Disorders Identification Test Guidelines for Use in Primary Care, 2nd ed.; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Center for Gambling Studies. Stituations, Behaviours, and Impacts of Gambling in Thailand, 2013: A Study in Higher Education Institutions [in Thai]. Available online: http://www.gamblingstudy-th.org/imgadmins/research_file/2556-Monrudee-surveystudent.pdf (accessed on 29 March 2020).
- Ranstam, J. Multiple P-values and Bonferroni correction. Osteoarthr. Cartil. 2016, 24, 763–764. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viner, R.M.; Taylor, B. Adult outcomes of binge drinking in adolescence: Findings from a UK national birth cohort. J. Epidemiol. Community Health 2007, 61, 902–907. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schulte, M.T.; Ramo, D.; Brown, S.A. Gender differences in factors influencing alcohol use and drinking progression among adolescents. Clin. Psychol. Rev. 2009, 29, 535–547. [Google Scholar] [CrossRef] [Green Version]
- Slade, T.; Chapman, C.; Swift, W.; Keyes, K.; Tonks, Z.; Teesson, M. Birth cohort trends in the global epidemiology of alcohol use and alcohol-related harms in men and women: Systematic review and metaregression. BMJ Open 2016, 6, e011827. [Google Scholar] [CrossRef]
- World Health Organization. Global Status Report on Alcohol and Health 2018; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Peters, S.A.E.; Huxley, R.R.; Woodward, M. Do smoking habits differ between women and men in contemporary Western populations? Evidence from half a million people in the UK Biobank study. BMJ Open 2014, 4, e005663. [Google Scholar] [CrossRef] [Green Version]
- Syamlal, G.; Mazurek, J.M.; Dube, S.R. Gender differences in smoking among U.S. working adults. Am. J. Prev. Med. 2014, 47, 467–475. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. WHO Report on the Global Tobacco Epidemic, 2017: Monitoring Tobacco use and Prevention Policies; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Castrén, S.; Heiskanen, M.; Salonen, A.H. Trends in gambling participation and gambling severity among Finnish men and women: Cross-sectional population surveys in 2007, 2010 and 2015. BMJ Open 2018, 8, e022129. [Google Scholar] [CrossRef] [Green Version]
- Wong, G.; Zane, N.; Saw, A.; Chan, A.K.K. Examining gender differences for gambling engagement and gambling problems among emerging adults. J. Gambl. Stud. 2013, 29, 171–189. [Google Scholar] [CrossRef]
- World Health Organization. Injuries and Violence: The facts; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Ng, C.J.; Teo, C.H.; Ho, C.C.K.; Tan, W.P.; Tan, H.M. The status of men’s health in Asia. Prev. Med. 2014, 67, 295–302. [Google Scholar] [CrossRef] [Green Version]
- Steen, K.; Hunskaar, S. Gender and physical violence. Soc. Sci. Med. 2004, 59, 567–571. [Google Scholar] [CrossRef] [PubMed]
- Bose, D.; Segui-Gomez, M.; Crandall, J.R. Vulnerability of female drivers involved in motor vehicle crashes: An analysis of US population at risk. Am. J. Public Health 2011, 101, 2368–2373. [Google Scholar] [CrossRef] [PubMed]
- Harris, K.; Gordon-Larsen, P.; Chantala, K.; Udry, J. Longitudinal trends in race/ethnic disparities in leading health indicators from adolescence to young adulthood. Arch. Pediatr. Adolesc. Med. 2006, 160, 74–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moure-Rodríguez, L.; Caamaño-Isorna, F.; Doallo, S.; Juan-Salvadores, P.; Corral, M.; Rodríguez-Holguín, S.; Cadaveira, F. Heavy drinking and alcohol-related injuries in college students. Gac. Sanit. 2014, 28, 376–380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, R.; Campbell, R.; Hildon, Z.; Hobbs, L.; Michie, S. Theories of behaviour and behaviour change across the social and behavioural sciences: A scoping review. Health Psychol. Rev. 2015, 9, 323–344. [Google Scholar] [CrossRef] [PubMed]
- Korman, L.M.; Collins, J.; Dutton, D.; Dhayananthan, B.; Littman-Sharp, N.; Skinner, W. Problem gambling and intimate partner violence. J. Gambl. Stud. 2008, 24, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Williams, W.H.; Cordan, G.; Mewse, A.J.; Tonks, J.; Burgess, C.N. Self-reported traumatic brain injury in male young offenders: A risk factor for re-offending, poor mental health and violence? Neuropsychol. Rehabil. 2010, 20, 801–812. [Google Scholar] [CrossRef]
- Maccallum, F.; Blaszczynski, A.; Ladouceur, R.; Nower, L. Functional and dysfunctional impulsivity in pathological gambling. Pers. Individ. Dif. 2007, 43, 1829–1838. [Google Scholar] [CrossRef]
- Hale, D.R.; Viner, R.M. The correlates and course of multiple health risk behaviour in adolescence. BMC Public Health 2016, 16, 458. [Google Scholar] [CrossRef] [Green Version]
- Sleet, D.A.; Ballesteros, M.F.; Borse, N.N. A review of unintentional injuries in adolescents. Annu. Rev. Public Health 2010, 31, 195–212. [Google Scholar] [CrossRef]
- Sanci, L.; Grabsch, B.; Chondros, P.; Shiell, A.; Pirkis, J.; Sawyer, S.; Hegarty, K.; Patterson, E.; Cahill, H.; Ozer, E.; et al. The prevention access and risk taking in young people (PARTY) project protocol: A cluster randomised controlled trial of health risk screening and motivational interviewing for young people presenting to general practice. BMC Public Health 2012, 12, 400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romer, D. Adolescent risk taking, impulsivity, and brain development: Implications for prevention. Dev. Psychobiol. 2010, 52, 263–276. [Google Scholar] [CrossRef] [PubMed]
- Shore, J.; Janssen, I. Adolescents’ engagement in multiple risk behaviours is associated with concussion. Inj. Epidemiol. 2020, 7, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Number in Sample |
|---|---|
| n (%) | |
| Total participants | 630 |
| Age group | |
| Youth (15–24 years) | 224 (35.6) |
| Young adults (25–39 years) | 406 (64.4) |
| Gender | |
| Female | 329 (52.2) |
| Male | 301 (47.8) |
| Marital status | |
| Single | 288 (45.7) |
| Married/partnered | 306 (48.6) |
| Divorced/separated/widowed | 36 (5.7) |
| Highest education | |
| None or primary | 76 (12.1) |
| Early secondary | 113 (17.9) |
| Late secondary | 256 (40.6) |
| Bachelor’s or higher | 185 (29.4) |
| Living location | |
| Urban location | 215 (34.1) |
| Rural location | 415 (65.9) |
| Health-Risk Behaviours By Age Group and Gender | Youth | Young Adults | All | |||
|---|---|---|---|---|---|---|
| (15–24 Years) | (25–39 Years) | (15–39 Years) | ||||
| Female | Male | Female | Male | Female | Male | |
| Number in sample | 127 | 97 | 202 | 204 | 329 | 301 |
| Alcohol Use (prevalence and 95% confidence interval) | ||||||
| Had used alcohol in their lifetime | 18.2 | 58.0 * | 29 | 80.2 * | 24.9 | 72.8 * |
| (12.3 to 26.1) | (47.3 to 48.0) | (22.8 to 36.2) | (73.9 to 85.2) | (20.2 to 30.1) | (67.2 to 77.7) | |
| Alcohol use in the past 3 months | 8.1 | 39.4 * | 14.7 | 60.0 * | 12.3 | 53.0 * |
| (4.4 to 14.4) | (29.7 to 50.0) | (10.2 to 20.6) | (52.7 to 66.7) | (8.9 to16.3) | (47.1 to 58.9) | |
| Heavy alcohol use in the past 30 days | 2.4 | 12.6 * | 1.9 | 24.2* | 2.1 | 20.3 * |
| (0.7 to 7.5) | (7.9 to 22.0) | (0.7 to 5.1) | (18.5 to 31.0) | (1.0 to 4.4) | (15.9 to 25.6) | |
| Tobacco Smoking (prevalence and 95% confidence interval) | ||||||
| Had smoked in their lifetime | 0.8 | 27.2 * | 4.2 | 56.9 * | 2.8 | 47.0 * |
| (0.1 to 5.5) | (19.1 to 37.3) | (1.9 to 8.8) | (49.7 to 63.9) | (1.4 to 5.8) | (41.1 to 53.0) | |
| Smoking in the past 3 months | 0 | 23.3 * | 1.1 | 46.2 * | 0.7 | 38.5 * |
| (15.7 to 33.1) | (0.3 to 4.5) | (39.1 to 53.4) | (0.2 to 2.8) | (33.0 to 44.4) | ||
| Gambling (prevalence and 95% confidence interval) | ||||||
| Ever gambled (legal and illegal) | 14.9 | 21.9 | 34.4 | 39.8 | 26.9 | 33.8 |
| (9.6 to 22.3) | (14.7 to 31.4) | (27.9 to 41.6) | (32.9 to 47.1) | (22.2 to 32.2) | (28.5 to 39.7) | |
| Legal gambling in the past 12 months | 3.8 | 8.3 | 25 | 24.9 | 16.9 | 19.4 |
| (1.6 to 9.1) | (4.2 to 14.7) | (19.3 to 31.7) | (19.2 to 31.8) | (13.1 to 21.4) | (15.1 to 24.5) | |
| Illegal gambling in the past 12 months | 6.5 | 12.1 | 13.4 | 17.2 | 10.8 | 15.5 |
| (3.3 to 12.3) | (6.9 to 20.4) | (9.3 to 19.0) | (12.3 to 23.5) | (7.8 to 14.7) | (11.7 to 20.3) | |
| Gambling (legal and illegal) in the past 12 months | 9.4 | 15.4 | 26.2 | 30.1 | 19.8 | 25.2 |
| (5.4 to 15.8) | (9.4 to 24.4) | (20.4 to 33.0) | (23.9 to 37.1) | (15.7 to 24.5) | (20.4 to 30.7) | |
| Health-Risk Behaviours | Health-Risk Behaviour Categories | Injuries Requiring Medical Attention aOR (95% CI), p-Value | Injuries Requiring Hospital Admission aOR (95% CI), p-Value | Injuries from Road Traffic Accidents Requiring Medical Attention aOR (95% CI), p-Value | |||
|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 1 | Model 2 | Model 1 | Model 2 | ||
| Alcohol Use | Never | Reference | Reference | Reference | Reference | Reference | Reference |
| Not in the past 3 months | 1.51 (0.46 to 4.91), p = 0.491 | 1.05 (0.27 to 4.27), p = 0.941 | 2.51 (0.68 to 9.27), p = 0.165 | 2.12 (0.45 to 9.93), p = 0.337 | 2.06 (0.59 to 7.21), p = 0.257 | 1.58 (0.37 to 6.88), p = 0.538 | |
| In the past 3 months but no heavy drinking in the past 30 day | 3.51 (1.32 to 9.33), p = 0.012 | 2.20 (0.74 to 6.56) p = 0.157 | 2.20 (0.58 to 8.37), p = 0.248 | 1.68 (0.34 to 8.30), p = 0.524) | 3.71 (1.27 to 10.9), p = 0.017 | 2.57 (0.73 to 9.14), p = 0.143 | |
| Heavy drinking in the past 30 days | 2.64 (0.87 to 7.97), p = 0.086 | 1.15 (0.34 to 3.89), p = 0.820 | 2.31 (0.52 to 10.2), p = 0.267 | 1.58 (0.31 to 8.08), p = 0.581 | 11.62 (0.40 to 6.51), p = 0.403 | 0.94 (0.19 to 4.69), p = 0.947 | |
| p-value * | 0.078 | 0.448 | 0.467 | 0.812 | 0.117 | 0.358 | |
| Smoking | Never | Reference | Reference | Reference | Reference | Reference | Reference |
| Not in the past 3 months | 7.67 (1.83 to 30.4), p = 0.004 | 6.50 (1.171 to 25.3), p = 0.014 | 5.51 (1.01 to 30.1), p = 0.049 | 4.69 (0.67 to 32.8), p = 0.119 | 5.29 (1.12 to 24.9), p = 0.035 | 4.22 (0.75 to 23.8), p = 0.103 | |
| In the past 3 months | 4.11 (1.19 to 14.3), p = 0.026 | 3.20 (0.81 to 12.6), p = 0.097 | 4.03 (1.03 to 15.8), p = 0.045 | 3.98 (0.78 to 20.0), p = 0.094 | 3.26 (0.89 to 11.9), p = 0.075 | 2.48 (0.58 to 10.5), p = 0.219 | |
| p-value * | 0.011 | 0.039 | 0.061 | 0.174 | 0.071 | 0.217 | |
| Gambling | Never | Reference | Reference | Reference | Reference | Reference | Reference |
| Legal gambling in the past 12 months | 2.59 (0.76 to 8.84), p = 0.128 | 2.23 (0.62 to 8.07), p = 0.220 | – | – | 1.68 (0.34 to 8.30), p = 0.522 | 1.52 (0.27 to 8.56), p = 0.637 | |
| Illegal gambling in the past 12 months | 1.27 (0.26 to 6.08), p = 0.762 | 1.05 (0.22 to 4.99), p = 0.954 | 1.84 (0.36 to 9.34), p = 0.463 | 1.69 (0.34 to 8.52), p = 0.523 | 1.42 (0.29 to 6.86), p = 0.661 | 1.21 (0.26 to 5.53), p = 0.803 | |
| Both legal and illegal in the past 12 months | 3.16 (1.13 to 8.83), p = 0.028 | 3.09 (1.05 to 9.05), p = 0.039 | 2.20 (0.63 to 7.62), p = 0.211 | 2.15 (0.64 to 7.22), p = 0.215 | 1.93 (0.57 to 6.50), p = 0.289 | 2.00 (0.52 to 7.71), p = 0.315 | |
| p-value * | 0.116 | 0.173 | 0.389 | 0.425 | 0.691 | 0.777 | |
| Number of Health-Risk Behaviours (Smoking, Drinking Alcohol and Gambling) | Injuries Requiring Medical Attention | Injuries Requiring Hospital Admission | Injuries from Road Traffic Accidents Requiring Medical Attention |
|---|---|---|---|
| aOR (95% CI), p-Value | aOR (95% CI), p-Value | aOR (95% CI), p-Value | |
| 0 | Reference | Reference | Reference |
| 1 | 1.43 (0.49 to 4.16), p = 0.513 | 1.69 (0.47 to 6.14), p= 0.422 | 2.16 (0.65 to 7.20), p =0.209 |
| 2 | 3.81 (1.33 to 10.90), p = 0.013 | 2.02 (0.50 to 8.11), p = 0.322 | 4.19 (1.39 to 12.60), p = 0.011 |
| 3 | 13.8 (4.24 to 45.10), p < 0.001 | 8.02 (1.94 to 33.30), p = 0.004 | 8.20 (2.27 to 29.50), p = 0.001 |
| p-value * | <0.001 | 0.037 | 0.008 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wattanapisit, A.; Jiraporncharoen, W.; Pinyopornpanish, K.; Jiraniramai, S.; Thaikla, K.; Angkurawaranon, C. Health-Risk Behaviours and Injuries among Youth and Young Adults in Chiang Mai, Thailand: A Population-Based Survey. Int. J. Environ. Res. Public Health 2020, 17, 3696. https://doi.org/10.3390/ijerph17103696
Wattanapisit A, Jiraporncharoen W, Pinyopornpanish K, Jiraniramai S, Thaikla K, Angkurawaranon C. Health-Risk Behaviours and Injuries among Youth and Young Adults in Chiang Mai, Thailand: A Population-Based Survey. International Journal of Environmental Research and Public Health. 2020; 17(10):3696. https://doi.org/10.3390/ijerph17103696
Chicago/Turabian StyleWattanapisit, Apichai, Wichuda Jiraporncharoen, Kanokporn Pinyopornpanish, Surin Jiraniramai, Kanittha Thaikla, and Chaisiri Angkurawaranon. 2020. "Health-Risk Behaviours and Injuries among Youth and Young Adults in Chiang Mai, Thailand: A Population-Based Survey" International Journal of Environmental Research and Public Health 17, no. 10: 3696. https://doi.org/10.3390/ijerph17103696