Impact of Gender Inequalities in the Causes of Mortality on the Competitiveness of OECD Countries


Abstract
:1. Introduction
2. Theoretical Background
3. Materials and Methods
4. Results
4.1. Descriptive Analysis
4.2. Analysis of Effects—Regression Analysis and Correlation Analysis
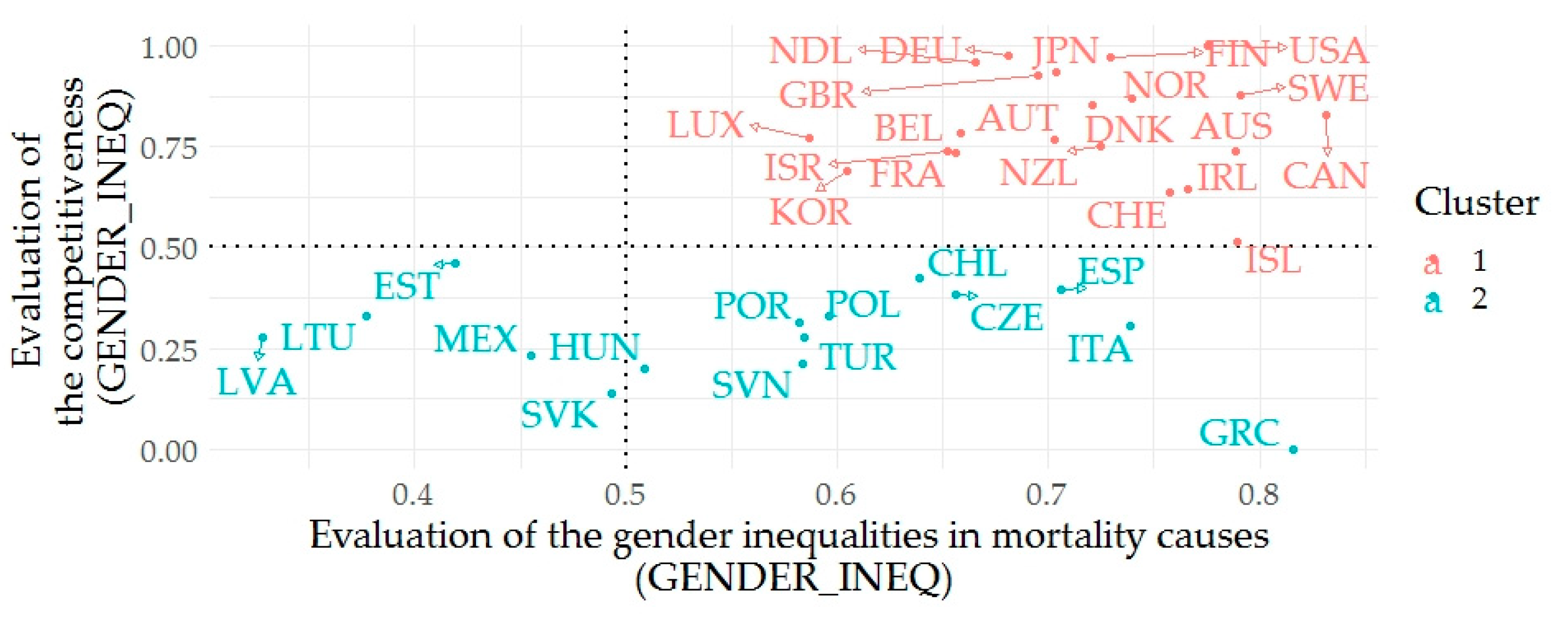
4.3. Cluster Analysis
5. Discussion
5.1. Descriptive and Difference Analysis Output—Gender Health Inequalities
5.2. Regression and Correlation Analysis Output—Relation between Health and Economic Output
5.3. Cluster Analysis Output—Relation between Health and Economic Output
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AUS | Australia |
| AUT | Austria |
| BEL | Belgium |
| CAN | Canada |
| COPD | chronic obstructive pulmonary disease |
| CZE | Czech Republic |
| DNK | Denmark |
| ESP | Spain |
| EST | Estonia |
| FIN | Finland |
| FRA | France |
| DEU | Germany |
| QALY | quality adjusted life year |
| GBR | United Kingdom |
| GCI | Global Competitiveness Index |
| GICM | gender inequalities in cause of mortality |
| GRC | Greece |
| HDI | Human Development Index |
| HIV/AIDS | human immunodeficiency virus/acquired immunodeficiency syndrome |
| HUN | Hungary |
| CHL | Chile |
| CHE | Switzerland |
| ISL | Iceland |
| IRL | Ireland |
| ISR | Israel |
| ITA | Italy |
| JPN | Japan |
| KOR | Korea |
| LVA | Latvia |
| LTU | Lithuania |
| LUX | Luxembourg |
| MEX | Mexico |
| NCD | non−communicable diseases |
| NDL | Netherlands |
| NZL | New Zealand |
| NOR | Norway |
| OLS | ordinary least squares |
| POL | Poland |
| POR | Portugal |
| PYLL | potential years of life lost |
| SD | standard deviation |
| SVK | Slovak Republic |
| SVN | Slovenia |
| SWE | Sweden |
| TUR | Turkey |
| USA | United States |
| VIF | variance inflation factor |
| WHO | World Health Organization |
Appendix A

{kind=link}
| ID | INFC | CNCR | BLOD | MTBL | MNTL | NRVS | CRCL | RSPT | DGST | SKIN | MSCL | GNTR | PRNT | GCI |
| AUS | 23.2 | 404.3 | 4.3 | 55.6 | 72.9 | 67.6 | 388.2 | 121.2 | 47.4 | 4.0 | 10.3 | 30.3 | 4.6 | 5.1 |
| AUT | 14.7 | 424.3 | 3.9 | 76.9 | 29.4 | 52.9 | 633.0 | 82.7 | 57.7 | 1.1 | 4.9 | 28.5 | 4.2 | 5.2 |
| BEL | 36.0 | 444.4 | 5.5 | 39.0 | 65.0 | 75.8 | 442.1 | 167.0 | 69.5 | 3.7 | 7.9 | 37.8 | 4.3 | 5.2 |
| CAN | 28.9 | 428.4 | 5.0 | 54.1 | 89.3 | 70.2 | 378.7 | 132.1 | 56.2 | 2.7 | 8.9 | 28.5 | 7.3 | 5.3 |
| CZE | 31.6 | 490.8 | 3.6 | 68.9 | 22.7 | 49.9 | 959.4 | 125.9 | 79.9 | 3.0 | 3.4 | 25.2 | 3.7 | 4.6 |
| DEU | 32.5 | 433.0 | 5.3 | 53.9 | 63.6 | 48.2 | 609.5 | 116.9 | 73.4 | 2.3 | 6.0 | 39.7 | 4.6 | 5.5 |
| DNK | 28.9 | 502.5 | 8.2 | 54.4 | 99.6 | 64.5 | 414.1 | 190.7 | 70.5 | 1.8 | 10.9 | 26.9 | 4.9 | 5.3 |
| ESP | 23.1 | 414.2 | 5.8 | 42.1 | 54.8 | 73.3 | 392.4 | 158.6 | 68.2 | 4.1 | 11.6 | 38.2 | 4.3 | 4.6 |
| EST | 17.9 | 542.0 | 2.6 | 22.4 | 16.4 | 40.3 | 1082.2 | 79.3 | 80.7 | 1.7 | 5.4 | 17.8 | 2.8 | 4.7 |
| FIN | 9.7 | 377.1 | 2.1 | 20.4 | 65.1 | 213.5 | 595.3 | 64.1 | 73.1 | 0.8 | 6.3 | 10.3 | 2.2 | 5.5 |
| FRA | 27.2 | 437.6 | 5.0 | 46.8 | 50.3 | 80.9 | 332.1 | 91.7 | 58.2 | 2.6 | 9.2 | 21.7 | 4.6 | 5.1 |
| GBR | 17.1 | 465.7 | 3.1 | 22.9 | 111.9 | 73.5 | 423.1 | 215.6 | 77.4 | 5.0 | 11.6 | 28.4 | 5.5 | 5.4 |
| GRC | 30.7 | 414.5 | 4.7 | 24.5 | 7.4 | 31.8 | 612.7 | 160.9 | 43.0 | 0.5 | 5.0 | 32.8 | 4.5 | 4.0 |
| HUN | 15.0 | 620.8 | 3.7 | 55.1 | 59.3 | 35.2 | 1209.5 | 141.9 | 121.8 | 2.1 | 7.4 | 18.0 | 6.9 | 4.3 |
| CHE | 16.1 | 379.5 | 3.7 | 34.3 | 94.0 | 69.9 | 431.2 | 86.7 | 51.5 | 1.9 | 11.6 | 21.6 | 5.2 | 5.0 |
| CHL | 37.2 | 442.0 | 8.4 | 94.0 | 39.6 | 64.1 | 505.1 | 194.4 | 118.9 | 6.0 | 9.1 | 57.9 | 8.3 | 4.6 |
| IRL | 14.6 | 481.7 | 4.8 | 39.2 | 65.6 | 74.3 | 519.5 | 206.3 | 55.8 | 2.8 | 11.2 | 37.9 | 3.8 | 5.0 |
| ISL | 13.6 | 422.8 | 4.3 | 25.3 | 46.0 | 138.3 | 479.9 | 114.0 | 41.4 | 2.1 | 7.9 | 22.1 | 1.8 | 4.8 |
| ISR | 77.4 | 374.1 | 9.5 | 103.7 | 45.3 | 49.8 | 346.8 | 115.9 | 49.3 | 15.3 | 10.6 | 73.2 | 3.7 | 5.1 |
| ITA | 30.7 | 441.3 | 6.7 | 61.0 | 36.5 | 56.0 | 499.8 | 101.6 | 53.7 | 2.2 | 6.8 | 27.4 | 4.7 | 4.4 |
| JPN | 24.8 | 388.3 | 4.1 | 20.6 | 9.8 | 26.1 | 319.8 | 196.7 | 47.0 | 1.4 | 5.6 | 32.8 | 1.4 | 5.4 |
| KOR | 40.7 | 395.2 | 3.6 | 63.2 | 32.6 | 54.8 | 335.6 | 167.8 | 55.3 | 2.8 | 9.1 | 34.0 | 4.1 | 5.1 |
| LTU | 42.3 | 520.6 | 2.0 | 19.7 | 6.6 | 35.4 | 1367.2 | 90.2 | 131.0 | 2.4 | 5.1 | 20.3 | 4.0 | 4.5 |
| LUX | 27.9 | 420.5 | 7.3 | 39.7 | 66.5 | 63.8 | 456.0 | 113.0 | 63.4 | 1.2 | 6.2 | 26.0 | 3.2 | 5.2 |
| LVA | 28.6 | 557.2 | 2.6 | 41.5 | 29.4 | 27.9 | 1414.8 | 74.8 | 90.5 | 4.2 | 6.7 | 33.8 | 7.0 | 4.4 |
| MEX | 43.8 | 258.2 | 15.1 | 360.9 | 14.4 | 29.7 | 568.8 | 194.0 | 188.4 | 7.7 | 15.3 | 70.1 | 15.2 | 4.3 |
| NDL | 31.4 | 491.7 | 5.4 | 38.6 | 104.5 | 72.4 | 420.8 | 144.2 | 51.0 | 3.2 | 10.4 | 37.1 | 5.1 | 5.5 |
| NOR | 34.1 | 422.4 | 5.0 | 35.7 | 79.2 | 66.8 | 430.4 | 152.6 | 45.2 | 3.7 | 9.4 | 30.0 | 3.1 | 5.3 |
| NZL | 15.2 | 443.7 | 3.1 | 50.7 | 64.8 | 62.7 | 501.3 | 139.4 | 45.4 | 4.9 | 11.1 | 22.1 | 6.6 | 5.1 |
| POL | 11.8 | 536.7 | 1.4 | 40.4 | 10.1 | 29.0 | 942.3 | 127.1 | 82.3 | 1.0 | 2.6 | 22.6 | 5.9 | 4.5 |
| POR | 34.7 | 424.5 | 6.7 | 81.9 | 28.4 | 52.2 | 469.9 | 197.5 | 71.5 | 1.7 | 5.9 | 44.5 | 4.7 | 4.5 |
| SVK | 12.4 | 562.3 | 2.3 | 42.2 | 40.9 | 51.1 | 1071.3 | 142.1 | 119.4 | 7.0 | 2.8 | 34.1 | 6.1 | 4.2 |
| SVN | 10.1 | 528.8 | 2.2 | 31.3 | 16.8 | 31.7 | 650.5 | 122.2 | 88.5 | 2.5 | 6.1 | 27.0 | 3.2 | 4.3 |
| SWE | 35.3 | 398.5 | 4.8 | 40.7 | 88.7 | 67.5 | 531.6 | 99.4 | 46.4 | 2.7 | 7.3 | 19.1 | 3.0 | 5.3 |
| TUR | 32.2 | 345.9 | 5.7 | 99.5 | 3.1 | 88.4 | 787.5 | 219.4 | 46.8 | 1.3 | 5.9 | 66.2 | 14.3 | 4.4 |
| USA | 45.1 | 398.3 | 6.7 | 72.8 | 88.3 | 106.0 | 524.8 | 171.5 | 63.5 | 2.9 | 8.5 | 43.2 | 7.5 | 5.5 |
References
- WHO. Health 2020: A European Policy Framework Supporting Action across Government and Society for Health and Well-Being; WHO Regional Office for Europe: Copenhagen, Denmark, 2013; Available online: http://www.euro.who.int/__data/assets/pdf_file/0006/199536/Health2020-Short.pdf?ua=1 (accessed on 28 April 2020).
- Beckfield, J.; Olafsdottir, S.; Bakhtiari, E. Health Inequalities in Global Context. Am. Behav. Sci. 2013, 57, 1014–1039. [Google Scholar] [CrossRef] [Green Version]
- Woodward, A. Why reduce health inequalities? J. Epidemiol. Community Health 2000, 54, 923–929. [Google Scholar] [CrossRef]
- Marmot, M.; Friel, S.; Bell, R.; Houweling, T.A.J.; Taylor, S. Closing the gap in a generation: Health equity through action on the social determinants of health. Lancet 2008, 372, 1661–1669. [Google Scholar] [CrossRef]
- McMichael, A.J.; McKee, M.; Shkolnikov, V.; Valkonen, T. Mortality trends and setbacks: Global convergence or divergence? Lancet 2014, 363, 1155–1159. [Google Scholar] [CrossRef]
- Houweling, T.A.J.; Kunst, A.E. Socio-economic inequalities in childhood mortality in low- and middle-income countries: A review of the international evidence. Br. Med. Bull. 2010, 93, 7–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mackenbach, J.P.; Meerding, W.J.; Kunst, A.E. Economic costs of health inequalities in the European Union. J. Epidemiol. Community Health 2011, 65, 412–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nanney, M.S.; Myers, S.L.; Xu, M.; Kent, K.; Durfee, T.; Allen, M.L. The Economic Benefits of Reducing Racial Disparities in Health: The Case of Minnesota. Int. J. Environ. Res. Public Health 2019, 16, 742. [Google Scholar] [CrossRef] [Green Version]
- Politzer, E.; Shmueli, A.; Avni, S. The economic burden of health disparities related to socioeconomic status in Israel. Isr. J. Health Policy Res. 2019, 8, 46. [Google Scholar] [CrossRef]
- Mackenbach, J.P.; Stirbu, I.; Roskam, A.J.R.; Schaap, M.M.; Menvielle, G.; Leinsalu, M.; Kunst, A.E. Socioeconomic inequalities in health in 22 European countries. N. Engl. J. Med. 2008, 358, 2468–2481. [Google Scholar] [CrossRef] [Green Version]
- Currie, J.; Schwandt, H.; Thuilliez, J. Pauvrete, Egalite, Mortalite: Mortality (in)equality in France and the United States. J. Popul. Econ. 2020, 33, 197–231. [Google Scholar] [CrossRef]
- Laliotis, I.; Ioannidis, J.P.A.; Stavropoulou, C. Total and cause-specific mortality before and after the onset of the Greek economic crisis: An interrupted time-series analysis. Lancet Public Health 2016, 1, E56–E65. [Google Scholar] [CrossRef] [Green Version]
- Bosworth, B. Increasing Disparities in Mortality by Socioeconomic Status. Annu. Rev. Public Health 2018, 39, 237–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker, M.; Currie, J.; Schwandt, H. Mortality Inequality in Canada and the United States: Divergent or Convergent Trends? J. Labor Econ. 2019, 37, S325–S353. [Google Scholar] [CrossRef]
- De Gelder, R.; Menvielle, G.; Costa, G.; Kovacs, K.; Martikainen, P.; Strand, B.H.; Mackenbach, J.P. Long-term trends of inequalities in mortality in 6 European countries. Int. J. Public Health 2017, 62, 127–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, D.; Allik, M.; Dundas, R.; Leyland, A.H. All-cause and cause-specific mortality in Scotland 1981–2011 by age, sex and deprivation: A population-based study. Eur. J. Public Health 2019, 29, 647–655. [Google Scholar] [CrossRef] [PubMed]
- Mustard, C.A.; Etches, J. Gender differences in socioeconomic inequality in mortality. J. Epidemiol. Community Health 2003, 57, 974–980. [Google Scholar] [CrossRef] [Green Version]
- Di Girolamo, C.; Nusselder, W.J.; Bopp, M.; Bronnum-Hansen, H.; Costa, G.; Kovacs, K.; Leinsalu, M.; Martikainen, P.; Pacelli, B.; Valverde, J.R.; et al. Progress in reducing inequalities in cardiovascular disease mortality in Europe. Heart 2020, 106, 40–49. [Google Scholar] [CrossRef] [Green Version]
- Pappas, G.; Queen, S.; Hadden, W.; Fisher, G. The Increasing Disparity in Mortality Between Socioeconomic Groups in the United-States; 1960 and 1986. N. Engl. J. Med. 1993, 329, 103–109. [Google Scholar] [CrossRef]
- Lewer, D.; Jayatunga, W.; Aldridge, R.W.; Edge, C.; Marmot, M.; Story, A.; Hayward, A. Premature mortality attributable to socioeconomic inequality in England between 2003 and 2018: An observational study. Lancet Public Health 2020, 5, e33–e41. [Google Scholar] [CrossRef] [Green Version]
- Cha, S.; Jin, Y. Have inequalities in all-cause and cause-specific child mortality between countries declined across the world? Int. J. Equity Health 2020, 19, 1. [Google Scholar] [CrossRef]
- Deaton, A. Health, inequality, and economic development. J. Econ. Lit. 2003, 41, 113–158. [Google Scholar] [CrossRef]
- Goldman, D.; Smith, J.P. The increasing value of education to health. Soc. Sci. Med. 2011, 72, 1728–1737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strand, B.H.; Groholt, E.K.; Steingrimsdottir, O.A.; Biakely, T.; Graff-Iversen, S.; Naess, O. Educational inequalities in mortality over four decades in Norway: Prospective study of middle aged men and women followed for cause specific mortality; 1960–2000. Br. Med. J. 2010, 340, c654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allik, M.; Brown, D.; Dundas, R.; Leyland, A.H. Differences in ill health and in socioeconomic inequalities in health by ethnic groups: A cross-sectional study using 2011 Scottish census. Ethn. Health 2019, 1–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrelli, A.; Di Napoli, A.; Sebastiani, G.; Rossi, A.; Rossi, P.G.; Demuru, E.; Costa, G.; Zengarini, N.; Alicandro, G.; Marchetti, S.; et al. Italian Atlas of Mortality Inequalities by Education Level. Epidemiol. Prev. 2019, 43, 1–120. [Google Scholar] [PubMed]
- Bertuccio, P.; Alicandro, G.; Sebastiani, G.; Zengarini, N.; Costa, G.; La Vecchia, C.; Frova, L. Mortality by occupation-based social class in Italy from 2012 to 2014. Int. J. Public Health 2018, 63, 865–874. [Google Scholar] [CrossRef] [PubMed]
- Doyal, L. Gender equity in health: Debates and dilemmas. Soc. Sci. Med. 2002, 51, 931–939. [Google Scholar] [CrossRef]
- Owens, I.P.F. Sex differences in mortality rate. Science 2002, 297, 2008–2009. [Google Scholar] [CrossRef]
- Singh-Manoux, A.; Gueguen, A.; Ferrie, J.; Shipley, M.; Martikainen, P.; Bonenfant, S.; Goldberg, M.; Marmot, M. Gender Differences in the Association between Morbidity and Mortality among Middle-Aged Men and Women. Am. J. Public Health 2008, 98, 2251–2257. [Google Scholar] [CrossRef]
- Marshall-Catlin, E.; Bushnik, T.; Tjepkema, M. Trends in mortality inequalities among the adult household population. Health Rep. 2019, 30, 11–17. [Google Scholar]
- De Torres, J.P.; Cote, C.G.; Lopez, M.V.; Casanova, C.; Diaz, O.; Marin, J.M.; Pinto-Plata, V.; de Oca, M.M.; Nekach, H.; Dordelly, L.J.; et al. Sex differences in mortality in patients with COPD. Eur. Respir. J. 2009, 33, 528–535. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, A.V.; Suissa, S.; Ernst, P. Gender differences in survival following hospitalisation for COPD. Thorax 2011, 66, 38–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ellison, L.F. Differences in cancer survival in Canada by sex. Health Rep. 2016, 27, 19–27. [Google Scholar] [PubMed]
- Fernandez, E.; Bosetti, C.; La Vecchia, C.; Levi, F.; Fioretti, F.; Negri, E. Sex differences in colorectal cancer mortality in Europe; 1955–1996. Eur. J. Cancer Prev. 2000, 9, 99–104. [Google Scholar] [CrossRef]
- Pampel, F.C. Declining sex differences in mortality from lung cancer in high-income nations. Demography 2003, 40, 45–65. [Google Scholar] [CrossRef]
- Kazerouni, N.; Alverson, C.J.; Redd, S.C.; Mott, J.A.; Mannino, D.M. Sex differences in COPD and lung cancer mortality trends—United States; 1968–1999. J. Womens Health 2004, 13, 17–23. [Google Scholar] [CrossRef] [Green Version]
- Kriksic, V.; Stevanovic, R.; Knezevic, T.; Krtalic, B.; Vrkic, T.Z.; Kos, J.; Gellineo, L.; Dapic, K.; Domislovic, V.; Cuti, E.C.; et al. Gender differences in cardiovascular mortality—Results from the epidemiology of hypertension in Croatia (EHUH study)—Mortality data after 17 years of follow-up. J. Hypertens. 2019, 37, E45. [Google Scholar] [CrossRef]
- Roche, M.M.; Wang, P.P. Sex Differences in All-Cause and Cardiovascular Mortality; Hospitalization for Individuals with and without Diabetes; and Patients with Diabetes Diagnosed Early and Late. Diabetes Care 2013, 36, 2582–2590. [Google Scholar] [CrossRef] [Green Version]
- Xu, G.; You, D.; Wong, L.; Duan, D.; Kong, F.; Zhang, X.; Zhao, J.; Xing, W.; Han, L.; Li, L. Risk of all-cause and CHD mortality in women versus men with type 2 diabetes: A systematic review and meta-analysis. Eur. J. Endocrinol. 2019, 180, 243–255. [Google Scholar] [CrossRef]
- Meirhaeghe, A.; Cottel, D.; Cousin, B.; Dumont, M.P.; Marecaux, N.; Amouyel, P.; Dallongeville, J. Sex Differences in Stroke Attack; Incidence; and Mortality Rates in Northern France. J. Stroke Cerebrovasc. Dis. 2018, 27, 1368–1374. [Google Scholar] [CrossRef]
- Roy-O’Reilly, M.; McCullough, L.D. Sex differences in stroke: The contribution of coagulation. Exp. Neurol. 2014, 259, 16–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ayala, C.; Croft, J.B.; Greenlund, K.J.; Keenan, N.L.; Donehoo, R.S.; Malarcher, A.M.; Mensah, G.A. Sex differences in US mortality rates for stroke and stroke subtypes by race/ethnicity and age; 1995–1998. Stroke 2002, 33, 1197–1201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, C.T.; Wu, B.Y.; Hu, W.L.; Hung, Y.C. Gender-based differences in mortality and complementary therapies for patients with stroke in Taiwan. Complement. Ther. Med. 2017, 30, 113–117. [Google Scholar] [CrossRef] [PubMed]
- Short, S.E.; Yang, Y.C.; Jenkins, T.M. Sex, Gender, Genetics, and Health. Am. J. Public Health 2013, 103, 93–101. [Google Scholar] [CrossRef]
- Boisclair, D.; Decarie, Y.; Laliberte-Auger, F.; Michaud, P.C.; Vincent, C. The economic benefits of reducing cardiovascular disease mortality in Quebec; Canada. PLoS ONE 2018, 13, e0190538. [Google Scholar] [CrossRef] [Green Version]
- Kozlova, O.A.; Nifantova, R.V.; Makarova, M.N. Methods of the Assessment of Economic Losses Caused by the Mortality of the Population Employed in Regional Economy. Econ. Reg. 2017, 13, 511–523. [Google Scholar] [CrossRef]
- Kalemli-Ozcan, S.; Ryder, H.E.; Weil, D.N. Mortality decline, human capital investment, and economic growth. J. Dev. Econ. 2000, 62, 1–23. [Google Scholar] [CrossRef]
- Herzer, D.; Nagel, K. The impact of adult and non-adult mortality on development: Two centuries evidence from a panel of industrial countries. J. Policy Model. 2019, 41, 352–371. [Google Scholar] [CrossRef]
- Herzer, D. How does mortality affect innovative activity in the long run? World Dev. 2020, 125, 104688. [Google Scholar] [CrossRef]
- Bar, M.; Leukhina, O. The role of mortality in the transmission of knowledge. J. Econ. Growth 2010, 15, 291–321. [Google Scholar] [CrossRef] [Green Version]
- Kordalska, A.; Olczyk, M. Global Competitiveness and Economic Growth: A One-Way or Two-Way Relationship? Equilib. Q. J. Econ. Econ. Policy 2016, 11, 121–142. [Google Scholar] [CrossRef] [Green Version]
- Perez-Moreno, S.; Rodriguez, B.; Luque, M. Assessing global competitiveness under multi-criteria perspective. Econ. Model. 2016, 53, 398–408. [Google Scholar] [CrossRef]
- Kiselakova, D.; Sofrankova, B.; Cabinova, V.; Onuferova, E. The Impact of R&D Expenditure on the Development of Global Competitiveness within the CEE EU Countries. J. Compet. 2018, 10, 34–50. [Google Scholar]
- Fyliuk, H.; Honchar, I.; Kolosha, V. The Interrelation between Economic Growth and National Economic Competitiveness: The Case of Ukraine. J. Compet. 2019, 11, 53–69. [Google Scholar] [CrossRef]
- Lall, S. Competitiveness indices and developing countries: An economic evaluation of the global competitiveness report. World Dev. 2001, 29, 1501–1525. [Google Scholar] [CrossRef]
- Sofrankova, B.; Kiselakova, D.; Cabinova, V. Innovation as a source of country’s global competitiveness growth. Innov. Econ. Symp. 2017, 39, 01026. [Google Scholar] [CrossRef] [Green Version]
- Ivanova, E.; Cepel, M. The Impact of Innovation Performance on the Competitiveness of the Visegrad 4 Countries. J. Compet. 2018, 10, 54–72. [Google Scholar] [CrossRef] [Green Version]
- WEF. The Global Competitiveness Report 2019. Available online: http://www3.weforum.org/docs/WEF_TheGlobalCompetitivenessReport2019.pdf (accessed on 28 April 2020).
- Overby, J. HIV/AIDS: A present and future threat to human capacity and global competitiveness. Compet. Rev. 2006, 16, 67–74. [Google Scholar] [CrossRef]
- Bucher, S. The Global Competitiveness Index as an Indicator of Sustainable Development. Her. Russ. Acad. Sci. 2018, 88, 44–57. [Google Scholar] [CrossRef]
- OECD. OECD. Stat. 2020. Available online: https://stats.oecd.org/# (accessed on 1 January 2020).
- OECD. Causes of Mortality. 2020. Available online: Stats.oecd.org/wbos/fileview2.aspx?IDFile=638c2ac2-5f0f-41ef-b2d9-2cfa1fd56429 (accessed on 1 January 2020).
- Fox, J.; Weisberg, S. An R Companion to Applied Regression, 3rd ed.; SAGE Publishing: Thousand Oaks, CA, USA, 2018; p. 607. [Google Scholar]
- White, H.A. Heteroskedasticity-Consistent Covariance-Matrix Estimator and a Direct Test for Heteroskedasticity. Econometrica 1980, 48, 817–838. [Google Scholar] [CrossRef]
- Ahmed, S.; Hasan, M.Z.; MacLennan, M.; Dorin, F.; Ahmed, M.W.; Hasan, M.M.; Hasan, S.M.; Islam, M.T.; Khan, J.A.M. Measuring the efficiency of health systems in Asia: A data envelopment analysis. BMJ Open 2019, 9, e022155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dagenais, G.R.; Leong, D.P.; Rangarajan, S.; Lanas, F.; Lopez-Jaramillo, P.; Gupta, R.; Diaz, R.; Avezum, A.; Oliveira, G.B.F.; Wielgosz, A.; et al. Variations in common diseases, hospital admissions, and deaths in middle-aged adults in 21 countries from five continents (PURE): A prospective cohort study. Lancet 2020, 395, 785–794. [Google Scholar] [CrossRef]
- WHO. The Top 10 Causes of Death. 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death?fbclid=IwAR0YjwTN7XSalNlUxxXzoXJHOHeJkSqbt934wZ7MZxMPhnf3dLHiStEPT_Q (accessed on 28 April 2020).
- Kubak, M.; Stefko, R.; Bartak, M.; Majernik, J.; Vagasova, T.; Fedelesova, M. Risk of dying from cancer by socio-demographic indicators in the Slovak republic. Cent. Eur. J. Public Health 2017, 25, S37–S43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schoeni, R.F.; Dow, W.H.; Miller, W.D.; Pamuk, E.R. The Economic Value of Improving the Health of Disadvantaged Americans. Am. J. Prev. Med. 2011, 40, S67–S72. [Google Scholar] [CrossRef]

| INFC | CNCR | BLOD | MTBL | MNTL | NRVS | CRCL | RSPT | DGST | SKIN | MSCL | GNTR | PRNT | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| F | Mean | 11.4465 | 164.7535 | 2.3030 | 26.2900 | 24.5420 | 29.0495 | 249.7840 | 50.6580 | 26.9905 | 1.6475 | 4.5190 | 13.7245 | 2.3240 |
| SD | 5.9057 | 26.4960 | 1.2777 | 28.0870 | 17.6477 | 17.6200 | 113.6978 | 20.4510 | 10.1736 | 1.3668 | 1.7802 | 6.4830 | 1.3221 | |
| CI 95% | 10.6230 | 161.0589 | 2.1248 | 22.3736 | 22.0812 | 26.5926 | 233.9302 | 47.8064 | 25.5719 | 1.4569 | 4.2708 | 12.8205 | 2.1397 | |
| 12.2700 | 168.4481 | 2.4812 | 30.2064 | 27.0028 | 31.5064 | 265.6378 | 53.5096 | 28.4091 | 1.8381 | 4.7672 | 14.6285 | 2.5083 | ||
| M | Mean | 16.8945 | 278.1220 | 2.6580 | 32.4805 | 25.6770 | 34.2785 | 360.1790 | 89.4960 | 44.9180 | 1.5710 | 3.4065 | 19.7090 | 2.8765 |
| SD | 8.2881 | 52.8338 | 1.4246 | 30.0712 | 14.8262 | 17.3646 | 179.6917 | 27.0570 | 21.4373 | 1.4238 | 1.3129 | 8.6967 | 1.6601 | |
| CI 95% | 15.7388 | 270.7549 | 2.4594 | 28.2874 | 23.6097 | 31.8572 | 335.1231 | 85.7232 | 41.9288 | 1.3725 | 3.2234 | 18.4963 | 2.6450 | |
| 18.0502 | 285.4891 | 2.8566 | 36.6736 | 27.7443 | 36.6998 | 385.2349 | 93.2688 | 47.9072 | 1.7695 | 3.5896 | 20.9217 | 3.1080 | ||
| ABS F-M | Mean | 5.5147 | 112.6588 | 0.5078 | 6.4348 | 4.3676 | 5.4348 | 110.0044 | 38.5426 | 17.7779 | 0.3050 | 1.2250 | 5.9495 | 0.6251 |
| SD | 3.7728 | 44.6773 | 0.4167 | 3.6089 | 3.1358 | 2.6032 | 70.1434 | 17.1292 | 12.5011 | 0.2853 | 0.9524 | 3.0609 | 0.4512 | |
| CI 95% | 15.7820 | 273.1206 | 2.4889 | 28.7128 | 23.2596 | 31.4754 | 341.5075 | 86.1079 | 42.5928 | 1.3872 | 3.2472 | 18.7783 | 2.6880 | |
| 17.8847 | 286.8187 | 2.8581 | 36.4633 | 27.0438 | 35.8519 | 388.5404 | 93.0434 | 48.1841 | 1.7479 | 3.5878 | 21.0132 | 3.1129 | ||
| Dif test | S-W (F) | 0.9329 † | 0.9433 † | 0.8735 † | 0.5198 † | 0.9749 ** | 0.7540 † | 0.7825 † | 0.9692 † | 0.8154 † | 0.6618 † | 0.9858 * | 0.8630 † | 0.7902 † |
| S-W(M) | 0.8791 † | 0.9851 * | 0.8520 † | 0.4961 † | 0.9473 † | 0.7678 † | 0.8358 † | 0.9828 * | 0.7858 † | 0.7383 † | 0.9721 † | 0.9116 † | 0.8033 † | |
| W | 32972.00 | 21953.50 | 37892.50 | 35900.00 | 40496.50 | 36034.00 | 31227.50 | 26270.00 | 27795.00 | 40052.50 | 34346.50 | 31846.00 | 35295.00 | |
| p-value | <0.001 | <0.001 | 0.001 | <0.001 | 0.305 | <0.001 | <0.001 | <0.001 | <0.001 | 0.524 | <0.001 | <0.001 | <0.001 | |
| Ordinary Least Squares (OLS) | Model Female | Model Male | Model Gender Inequalities | |||
|---|---|---|---|---|---|---|
| HC3 | HC3 | HC3 | ||||
| F = 28.62 (p < 0.001) | F = 32.53 (p < 0.001) | F = 25.46 (p < 0.001) | ||||
| R2 = 0.67; R2 adj. = 0.64 | R2 = 0.70; R2 adj. = 0.68 | R2 = 0.64; R2 adj. = 0.62 | ||||
| Estimate | Pr (>|t|) | Estimate | Pr (>|t|) | Estimate | Pr (>|t|) | |
| Intercept | 5.3685 | <0.001 | 5.9336 | <0.001 | 5.8748 | <0.001 |
| INFC | 0.0064 | 0.430 | 0.0101 | 0.008 | 0.0316 | <0.001 |
| CNCR | −0.0005 | 0.725 | −0.0048 | <0.001 | −0.0095 | <0.001 |
| BLOD | −0.0592 | 0.296 | −0.1078 | 0.004 | −0.0464 | 0.430 |
| MTBL | 0.0021 | 0.329 | −0.0015 | 0.446 | −0.0031 | 0.708 |
| MNTL | 0.0189 | <0.001 | 0.0200 | <0.001 | 0.0381 | <0.001 |
| NRVS | 0.0011 | 0.341 | −0.0010 | 0.524 | 0.0385 | 0.002 |
| CRCL | −0.0018 | <0.001 | 0.0000 | 0.935 | 0.0006 | 0.329 |
| RSPT | −0.0071 | <0.001 | 0.0002 | 0.884 | 0.0079 | 0.001 |
| DGST | 0.0038 | 0.212 | 0.0013 | 0.297 | −0.0145 | <0.001 |
| SKIN | −0.0444 | 0.156 | −0.0667 | 0.002 | −0.1765 | 0.018 |
| MSCL | −0.0322 | 0.153 | 0.0240 | 0.333 | −0.0676 | 0.065 |
| GNTR | 0.0112 | 0.141 | 0.0101 | 0.090 | −0.0314 | <0.001 |
| PRNT | −0.0346 | 0.156 | −0.0844 | <0.001 | −0.2920 | <0.001 |
| Spearman ρ | Female | Male | Gender Inequalities | |||
|---|---|---|---|---|---|---|
| ρ | Pr(>|t|) | ρ | Pr(>|t|) | ρ | Pr(>|t|) | |
| INFC | 0.1630 | 0.020 | 0.0318 | 0.652 | −0.0650 | 0.356 |
| CNCR | 0.0456 | 0.518 | −0.4105 | <0.001 | −0.5074 | <0.001 |
| BLOD | 0.0983 | 0.162 | 0.1253 | 0.074 | 0.0334 | 0.635 |
| MTBL | −0.1849 | 0.008 | −0.1222 | 0.082 | 0.1155 | 0.100 |
| MNTL | 0.6665 | <0.001 | 0.6434 | <0.001 | 0.0963 | 0.170 |
| NRVS | 0.4546 | <0.001 | 0.4739 | <0.001 | −0.0557 | 0.429 |
| CRCL | −0.5215 | <0.001 | −0.4623 | <0.001 | −0.1989 | 0.004 |
| RSPT | 0.0578 | 0.412 | −0.1624 | 0.020 | −0.4133 | <0.001 |
| DGST | −0.2348 | <0.001 | −0.3685 | <0.001 | −0.4700 | <0.001 |
| SKIN | 0.0667 | 0.344 | 0.0371 | 0.601 | −0.1063 | 0.133 |
| MSCL | 0.261 | <0.001 | 0.2725 | <0.001 | 0.0129 | 0.855 |
| GNTR | −0.043 | 0.541 | −0.0498 | 0.479 | −0.1085 | 0.122 |
| PRNT | −0.2095 | 0.003 | −0.2548 | <0.001 | −0.2994 | <0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gavurova, B.; Ivankova, V.; Rigelsky, M.; Suhanyi, L. Impact of Gender Inequalities in the Causes of Mortality on the Competitiveness of OECD Countries. Int. J. Environ. Res. Public Health 2020, 17, 3698. https://doi.org/10.3390/ijerph17103698
Gavurova B, Ivankova V, Rigelsky M, Suhanyi L. Impact of Gender Inequalities in the Causes of Mortality on the Competitiveness of OECD Countries. International Journal of Environmental Research and Public Health. 2020; 17(10):3698. https://doi.org/10.3390/ijerph17103698
Chicago/Turabian StyleGavurova, Beata, Viera Ivankova, Martin Rigelsky, and Ladislav Suhanyi. 2020. "Impact of Gender Inequalities in the Causes of Mortality on the Competitiveness of OECD Countries" International Journal of Environmental Research and Public Health 17, no. 10: 3698. https://doi.org/10.3390/ijerph17103698