
Abstract
Background and Objective
Sodium-glucose cotransporter 2 inhibitors (SGLT2i) have significant efficacy in reducing the risk of hospitalization for heart failure (hHF) or cardiovascular (CV) mortality in patients with type 2 diabetes mellitus (T2DM). However, there are differences in HF outcomes between the SGLT2i. Therefore, we compared the cost needed to achieve these outcomes between empagliflozin, canagliflozin, and dapagliflozin.
Methods
We calculated the cost needed to treat (CNT) in order to prevent one event of hHF or CV mortality, by multiplying the annualized number needed to treat (NNT) to prevent one event, by the annual cost of each therapy. Efficacy estimates were extracted from published randomized controlled trial (RCT) data. A sensitivity analysis was performed to mitigate differences between the RCT populations. Drug costs were extracted from the 2020 US National Average Drug Acquisition Cost listing.
Results
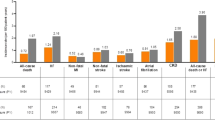
We figured empagliflozin’s CNT to be $664,464 (95% CI $499,872–$1,097,280), $1,535,387 (95% CI $886,074–$3,210,501) for canagliflozin, and $2,693,145 (95% CI $1,639,563–$11,092,206) for dapagliflozin. The sensitivity analysis confirmed the cost advantage of empagliflozin.
Conclusions
Our findings suggest that empagliflozin prescribed for preventing CV death or hHF in T2DM patients seems to be cost saving compared to treatment with canagliflozin, and dapagliflozin.
Similar content being viewed by others

Change history
06 June 2020
A Correction to this paper has been published: https://doi.org/10.1007/s40261-020-00932-4
References
Kosiborod M, Cavender MA, Fu AZ, Wilding JP, Khunti K, Holl RW, et al. Lower risk of heart failure and death in patients initiated on sodium-glucose cotransporter-2 inhibitors versus other glucose-lowering drugs. Circulation. 2017;136:249–59.
Fitchett D, Inzucchi SE, Cannon CP, et al. Empagliflozin reduced mortality and hospitalization for heart failure across the spectrum of cardiovascular risk in the EMPA-REG OUTCOME trial. Circulation. 2019;139(11):1384–95.
Rådholm K, Figtree G, Perkovic V, Solomon SD, Mahaffey KW, de Zeeuw D, et al. Canagliflozin and heart failure in type 2 diabetes mellitus. Circulation. 2018;138(5):458–68.
Kato ET, Silverman MG, Mosenzon O, Zelniker TA, Cahn A, Furtado RHM, et al. Effect of dapagliflozin on heart failure and mortality in type 2 diabetes mellitus. Circulation. 2019;139(22):2528–36.
Dunlay SM, Givertz MM, Aguilar D, Allen LA, Chan M, Desai AS, et al. Type 2 diabetes mellitus and heart failure: a scientific statement from the American Heart Association and the Heart Failure Society of America. Circulation. 2019;139:1–31.
American Diabetes Association. 9. Pharmacologic Approaches to Glycemic Treatment: Standards of Medical Care in Diabetes-2020. Diabetes Care. 2020;43(Suppl 1):S98–110. https://doi.org/10.2337/dc20-S009
Täger T, Atar D, Agewall S, Katus HA, Grundtvig M, Cleland JGF, et al. Comparative efficacy of sodium-glucose cotransporter-2 inhibitors (SGLT2i) for cardiovascular outcomes in type 2 diabetes: a systematic review and network meta-analysis of randomised controlled trials. Heart Fail Rev. 2020. https://doi.org/10.1007/s10741-020-09954-8.
Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med. 2015;373(22):2117–288.
Neal B, Perkovic V, Kenneth W, de Mahaffey ZD, Fulcher G, Erondu N, Shaw W, et al. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med. 2017;377(7):644–57.
Wiviott SD, Raz I, Bonaca MP, Mosenzon O, Kato ET, Cahn A, et al. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2019;380(4):347–57.
Mayne TJ, Whalen E, Vu A. Annualized was found better than absolute risk reduction in the calculation of number needed to treat in chronic conditions. J Clin Epidemiol. 2006;59:217–23.
Mendes D, Alves C, Batel-Marques F. Number needed to treat (NNT) in clinical literature: an appraisal. BMC Med. 2017;15(1):1–13.
Lehrke M, Marx N. Diabetes mellitus and heart failure. Am J Cardiol. 2017;120:S37–47.
Packer M. Heart failure: the most important, preventable, and treatable cardiovascular complication of type 2 diabetes. Diabetes Care. 2018;41:11–3.
Verma S, Jüni P, Mazer CD. Pump, pipes, and filter: do SGLT2 inhibitors cover it all? Lancet. 2019;393:3–5.
McMurray JJV, Solomon SD, Inzucchi SE, Køber L, Kosiborod MN, Martinez FA, et al. Dapagliflozin in patients with heart failure and reduced ejection fraction. N Engl J Med. 2019;381:1995–2008.
Zelniker TA, Wiviott SD, Raz I, Im K, Goodrich EL, Bonaca MP, et al. SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes: a systematic review and meta-analysis of cardiovascular outcome trials. Lancet. 2019;393:31–9.
Rahman W, Solinsky PJ, Munir KM, Lamos EM. Pharmacoeconomic evaluation of sodium-glucose transporter-2 (SGLT2) inhibitors for the treatment of type 2 diabetes. Expert Opin Pharmacother. 2019;20:151–61.
Kaku K, Haneda M, Sakamaki H, Yasui A, Murata T, Ustyugova A, et al. Cost-effectiveness analysis of empagliflozin in japan based on results from the Asian population in the EMPA-REG OUTCOME Trial. Clin Ther. 2019;41:2021–40.
Nguyen E, Coleman CI, Nair S, Weeda ER. Cost-utility of empagliflozin in patients with type 2 diabetes at high cardiovascular risk. J Diabetes Complicat. 2018;32:210–5.
Hou X, Wan X, Wu B. Cost-effectiveness of canagliflozin versus dapagliflozin added to metformin in patients with type 2 diabetes in China. Front Pharmacol. 2019;10:1–8.
Neslusan C, Teschemaker A, Willis M, Johansen P, Vo L. Cost-effectiveness analysis of canagliflozin 300 mg versus dapagliflozin 10 mg added to metformin in patients with type 2 diabetes in the United States. Diabetes Ther. 2018;9:565–81.
Moher D, Hopewell S, Schulz KF, et al. CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomized trials. BMJ. 2010;340:c869.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
No funding was received to conduct this study.
Conflict of interest
Author RA declares he has no conflict of interest. Author EA declares he has no conflict of interest. Author AH declares he has no conflict of interest. Author JA has received non-financial support from Janssen Pharmaceuticals, Speaker, and consulting honorarium from Pfizer and Novonordisk.
Authorship
Author RA initiated the study and wrote the initial draft. Author EA researched and analyzed the data and drafted the results section. Author AH contributed to the methods and discussion and edited the manuscript. Author JA reviewed the data analysis and the final draft of the manuscript.
Rights and permissions
About this article

Cite this article
Arbel, R., Aboalhasan, E., Hammerman, A. et al. Sodium-Glucose Cotransporter 2 Inhibitors for Prevention of Heart Failure Events in Patients with Type 2 Diabetes Mellitus: A Cost Per Outcome Analysis. Clin Drug Investig 40, 665–669 (2020). https://doi.org/10.1007/s40261-020-00929-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40261-020-00929-z