Comparison of the Clinical Results of Identically Designed Total Knee Prostheses with Different Surface Roughnesses


Department of Orthopaedic Surgery, School of Medicine, Inha University, Incheon 22332, Korea
*
Author to whom correspondence should be addressed.
Coatings 2020, 10(5), 486; https://doi.org/10.3390/coatings10050486
Submission received: 1 May 2020
/
Revised: 13 May 2020
/
Accepted: 14 May 2020
/
Published: 19 May 2020
(This article belongs to the Special Issue Surface Modification of Medical Implants)
Abstract
:The purpose of this study was to investigate the effects of the undersurface roughness of total knee prosthesis on clinical outcomes. We compared the clinical and radiological outcomes and prosthesis survivals in patients who underwent total knee arthroplasty using prosthesis with identical designs but different surface roughness (average surface roughnesses (Ra), 5.0 μm vs. 11.6 μm). The results showed that the knee prostheses with a more roughened undersurface (Ra = 11.6 μm) produced significantly better functional results and enhanced prosthesis survival. The difference in surface roughness was associated with incidence of osteolysis and loosening at the tibial baseplate, but not at the femoral component. Overall, our results provided significant evidence that the use of roughened undersurface of tibial baseplate would be a way to prevent aseptic loosening.
1. Introduction
Total knee arthroplasty (TKA) is the most effective surgical treatment for end-stage osteoarthritic knee disease when all non-operative methods have failed. TKA has shown good clinical outcomes since the introduction of cemented TKA in the 1960s, but aseptic loosening remains an unsolved problem [1]. Although the cause of loosening in cemented TKA is multifactorial, delayed instability of the prosthesis-cement interface is the leading cause of loosening [2,3,4].
The influence of prosthesis surface texture on the stability of the prosthesis-cement interface have been studied, and several mechanical studies have demonstrated that bonding strength between prosthesis and cement increase with increasing surface roughness of the prosthesis [5,6,7]. However, it is debatable whether roughened prostheses are clinically desirable [8,9]. In hip arthroplasty, rough surfaced femoral stems produced more wear debris caused by tension between cement and bone, resulting in more stem loosening through osteolysis than polished femoral stem [8,9,10,11]. But to our knowledge, no study has compared the clinical results of total knee prostheses with different undersurface roughness.
We examined the use of the prosthesis with an identical design and material but different undersurface roughness in primary TKA. The senior author has been using Buechel and Pappas (B-P) knee prostheses (L-F Knee System, Cellumed Co., Ltd., Seoul, Korea) for primary TKA since May 2009. The manufacturer increased the surface roughness of this prosthesis by changing the surface finish treatment in October 2013.
The purpose of the present study was to compare the clinical and radiological outcomes and prosthesis survivals in patients who underwent TKA using prosthesis with identical designs of different surface roughness. We hypothesized that increasing the surface roughness of total knee prosthesis would improve clinical and radiological outcomes and prosthesis survivals, and reduce aseptic loosening rates.
2. Materials and Methods
2.1. Surface Roughnesses of Prosthesis
The B-P knee prosthesis used in the present study had a mobile bearing design and was made of titanium alloy (TI6AL4V) coated with a golden-colored titanium nitride (TiN) hard coating, which confers higher scratch resistance, low friction characteristics and good wettability by synovial fluids [12,13]. Prior to October 2013, the undersurface of prosthesis was sandblasted for five minutes using 16-mesh sand before TiN coating (prosthesis A). However, due to the hardness of this coating, surface roughnesses of prosthesis A were lower than expected, and thus, the surface finishing process was changed in October 2013 (prosthesis B) by sandblasting using 16-mesh sand (the same used for prosthesis A) after TiN coating. Surface treatment processes are schematized in Figure 1.
Average surface roughnesses (Ra) of 10 unused samples of prostheses A and B determined using a portable roughness tester (Taylor Hobson Surtronic® S-116, AMETEK Inc., Berwyn, PA, USA) were 5.0 ± 0.39 and 11.6 ± 0.52 μm, respectively. Prosthesis B had a rougher undersurface than prosthesis A, as might be expected (Figure 2).
2.2. Patient Selection
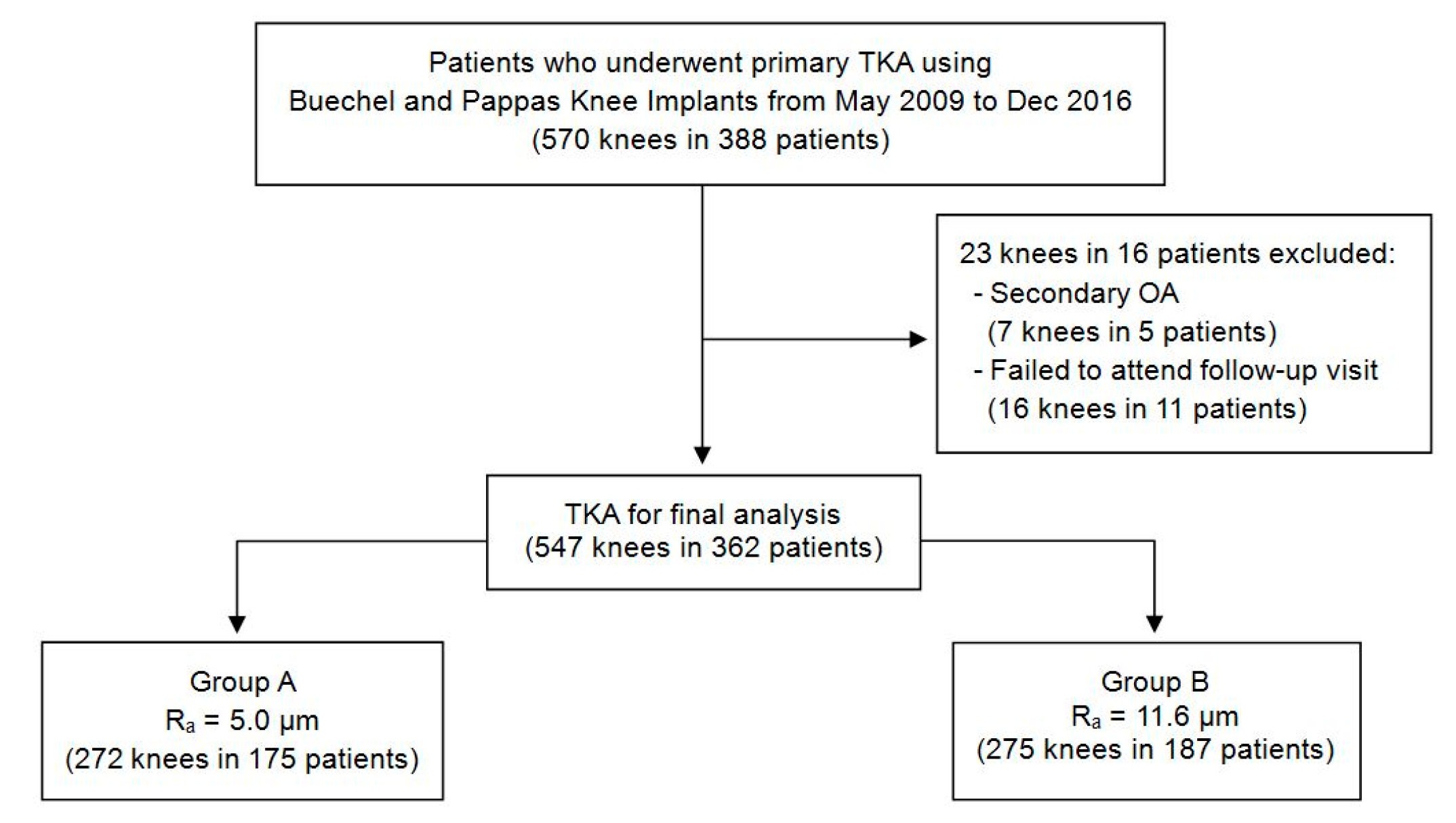
Of the 388 patients that underwent primary TKA using B-P knee prosthesis at our institute from May 2009 to December 2016, 570 consecutive knees were initially considered for this retrospective study. Patients of Kellgren-Lawrence classification grade III or IV that underwent primary TKA for primary osteoarthritis were included. However, patients with secondary osteoarthritis (e.g., rheumatoid arthritis, gouty arthritis, post-septic arthritis, or post-traumatic arthritis) and those followed for <3 years were excluded. In addition, patients with severe tibial bony defect were treated using a different knee prosthesis with a block or wedge, and/or stem extension was also excluded. After applying inclusion and exclusion criteria, 547 knees in 362 patients were enrolled in this study. Of 175 patients, 272 knees underwent TKA using prosthesis A (group A) and 275 knees in 187 patients underwent TKA using prosthesis B (group B) (Figure 3).
The study design and protocol were reviewed and approved by the institutional review board (IRB) of our institution (IRB No. INHAUH 2019-11-022), which waived informed consent due to the retrospective nature of the study.
2.3. Operative Procedure and Treatment after Surgery
All TKAs were performed by one senior orthopaedic surgeon using the standard mid-vastus approach and gap balancing technique in all cases. All components were fixed with DEPUY CMW3 Gentamicin BoneCement 40 g (Depuy Synthes, Raynham, MA, USA) using a modern cementing technique [14].
Routine perioperative antibiotics, prophylactic management of deep vein thrombosis (DVT) (antithrombotic stockings, intermittent pneumatic compression, and anticoagulation), pain management, and early postoperative rehabilitation protocols were similarly applied in all patients.
2.4. Clinical and Radiological Assessments
The clinical and functional performances of knee joints were evaluated using the American Knee Society Score (AKSS) scale (0–100, 100 being the best score) before surgery and annually after surgery [15]. Group AKSS scores at 3 years after surgery were compared. Surgical findings, postoperative ranges of motion (ROM), and complications or subsequent revision surgeries were recorded. Complications included major postoperative events such as revision surgery for any indication, aseptic loosening of any component, prosthetic joint infection, periprosthetic fracture, deep vein thrombosis (DVT), knee stiffness, and TKA-associated local tissue irritation. The presence of DVT was determined by doppler ultrasound before and 6 weeks after surgery. Prosthesis failure was defined as osteolysis and/or progressive radiolucency on serial radiographs, a prosthesis-related problem, or significant knee pain probably caused by inadequate prosthesis fixation [16]. Revision TKA was performed in cases of prosthesis failure.
Radiographic analysis was performed in anteroposterior and lateral views by one senior orthopedic surgeon who recorded the presence of any osteolytic lesion or radiolucent line > 2 mm located under the surface-cemented prosthesis on any postoperative radiograph [17,18]. Measurements were taken in millimeters using an INFINITT M6 Picture Archiving and Communication System (INFINITT Healthcare Co., Ltd, Seoul, Korea).
2.5. Statistical Analysis
The significance of differences between group A (Ra = 5.0) and group B (Ra = 11.6) were determined using the independent t-test or the nonparametric Mann-Whitney U-test when variables were non-normally distributed. Radiologic findings, complications, and revision rates were compared using Pearson’s chi-squared test or Fisher’s exact test. Times to failure (for any reason or aseptic loosening only) were subjected to Kaplan-Meier analysis. Cox proportional hazard regression analysis was used to identify factors associated with the risk of aseptic loosening. The analysis was conducted using IBM SPSS Statistics for Windows, version 19.0 (IBM Corp., Armonk, NY, USA). Results are presented as means ± standard deviation or as numbers and percentages, and statistical significance was set at p < 0.050.
3. Results
3.1. Patients Demographics
The demographic characteristics of the two groups are summarized in Table 1. In group A, the mean age at surgery was 68.2 years (range, 45–92 years), and the mean follow-up was 69.7 months (range, 36–125 months), and in group B, the mean age at surgery was 67.6 years (range, 47–93 years), and mean follow-up was 51.0 months (range, 36–73 months). The follow-up duration was significantly greater in group A (p = 0.001). No significant intergroup difference was found between patient demographics (e.g., age, gender, body mass index (BMI), surgical side, or bone mineral density (BMD)) (Table 1).
3.2. Clinical and Radiological Outcomes
In group A, clinical and functional AKSS scores significantly improved after surgery from 68.1 ± 8.5 and 65.7 ± 7.2 preoperatively to 95.2 ± 7.6 and 83.2 ± 20.5 at three years postoperatively, respectively (p < 0.001), and in group B from 67.1 ± 5.4 and 64.0 ± 11.5 preoperatively to 95.8 ± 7.3 and 88.8 ± 17.3 at three years postoperatively, respectively (p < 0.001). Clinical AKSS at three years postoperatively were similar in the two groups (p = 0.515), but functional AKSS at three years postoperatively were better in group B (p = 0.023). Mean flexion contractures and ROM at three years postoperatively were 0.37° ± 3.23° and 118.1° ± 14.0° in group A and 0.39° ± 1.82° and 120.1° ± 9.1° in group B, respectively, and these differences were not statistically significant (Flexion contracture, p = 0.950; ROM, p = 0.164) (Table 2).
There were no statistically significant differences between the two groups in prevalence of minor complications; superficial infection (p = 0.497), hypertrophic synovitis (p = 0.497), DVT (p > 0.999), and stiff knee (p = 0.800) (Table 2). One knee (0.4%) in group A experienced superficial infection four weeks following TKA and was treated with oral antibiotics. Hypertrophic synovitis occurred in one knee in group A (0.4%) and was treated with arthroscopic synovectomy. DVT checked by doppler ultrasound six weeks after surgery occurred in three knees in group A (1.1%) and in four knees in group B (1.5%). Eight knees in group A (2.9%) and seven knees in group B (2.5%) required manual manipulation following TKA because ROM was less than 90° at the 12 weeks follow-up visit.
During the three years after TKA, 21 knees in group A (7.7%) and five knees in group B (1.8%) developed tibial osteolysis, and 25 knees in group A (9.2%) and in seven knees in group B (2.5%) developed a tibial radiolucent line, and both represented a significant intergroup difference (both p = 0.001) (Table 2). On the other hand, femoral osteolysis and femoral radiolucent line development rates (p = 0.105 and 0.472, respectively) were not significantly different in the two groups (Table 2).
3.3. Prosthesis Survivorship
Thirteen knees (4.8%) in group A and five knees (1.8%) in the group B underwent revision for any reason, and these rates were not significantly different (p = 0.058). Nine cases of aseptic loosening occurred in group A (3.3%) at a mean time to failure of 38.7 months, but only two occurred in group B (0.7%) at a mean time to failure of 16.5 months. Revision rates due to aseptic loosening were significantly different between the two groups (p = 0.035). Revision rates due to prosthetic joint infection or periprosthetic fracture were not significantly different between the two groups (Table 2).
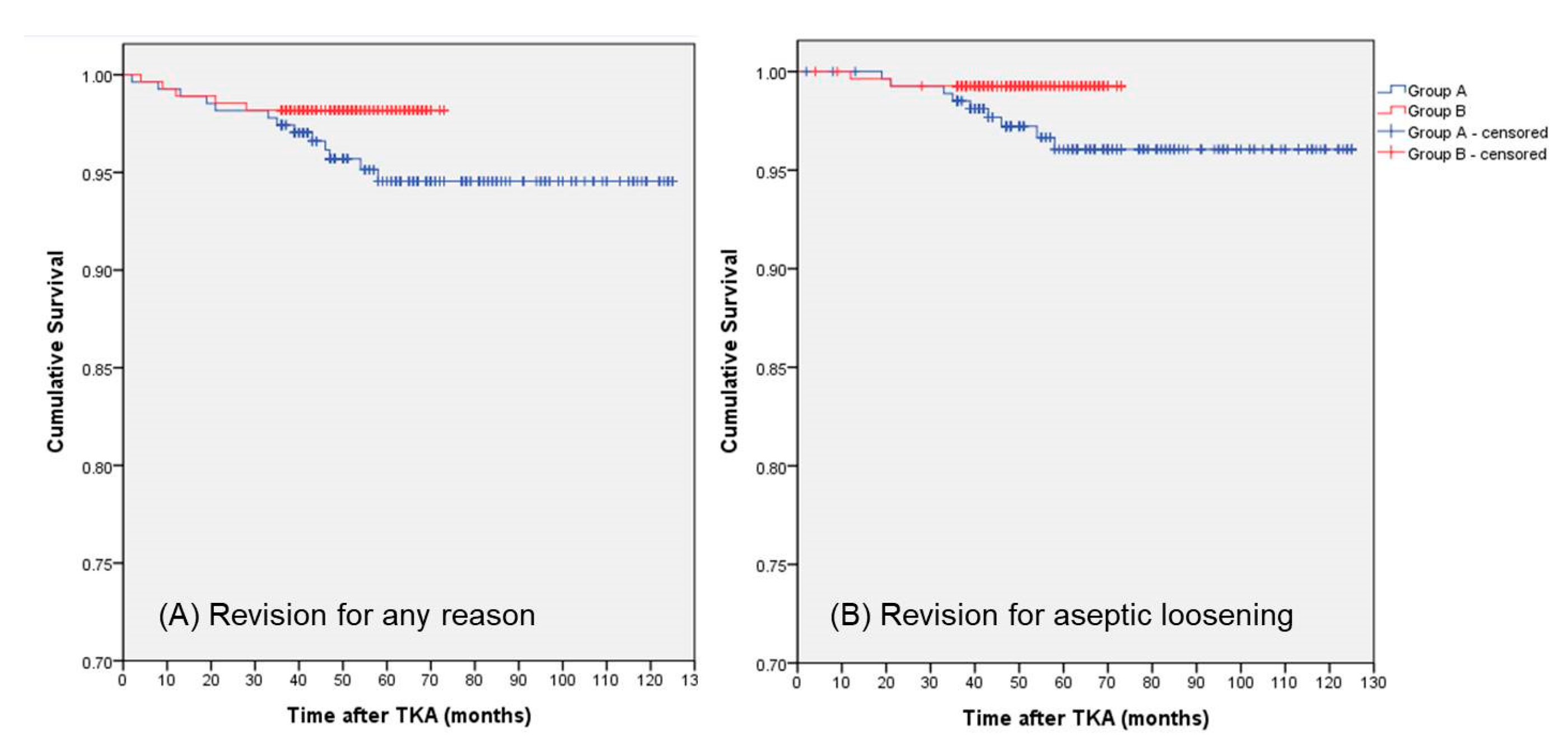
Prosthesis survival was greater in group B than in group A, as determined by Kaplan-Meier survival analysis. In group A, 3-, 5-, and 7-year survival rates using any reason as the endpoint were 97.4%, 94.5%, and 94.5%, respectively, and in group B corresponding 3- and 5-year survival rates were both 98.2% (Figure 4A). In group A, 3-, 5- and 7-year survival rates using aseptic loosening as the endpoint were 98.5%, 96.1%, and 96.1%, respectively, and in group B corresponding 3- and 5-year survival rates were both 99.3% (Figure 4B).
3.4. The Risk Factors of Aseptic Loosening in Multivariate Analysis
Cox proportional hazards regression analysis was used to identify risk factors of aseptic loosening. Notably, a prosthesis with an undersurface Ra value of 5.0 µm was found to be significantly more associated with aseptic loosening (odds ratio (OR) 4.69, 95% confidence interval (CI) 1.02–21.52, p = 0.047) than a prosthesis with a roughened undersurface Ra value of 11.6 μm. Age (OR 0.95, 95% CI 0.88–1.03, p = 0.226), sex (male rather than female, OR 1.67, 95% CI 0.33–8.36, p = 0.536), BMI (OR 0.99, 95% CI 0.84–1.16, p = 0.870), and BMD (OR 0.94, 95% CI 0.54–1.64, p = 0.831) were not found to be significantly associated with aseptic loosening.
4. Discussion
The present study was undertaken to investigate the effects of the undersurface roughness of total knee prosthesis on clinical outcomes, and the results showed that rough surfaced prostheses produced significantly better functional results and enhanced prosthesis survival.
The success of joint arthroplasty is directly related to prosthesis lifetime, aseptic loosening between cement and prosthesis and/or bone is one of the persistent problems of cemented arthroplasty [1,18,19]. Despite widespread awareness of the problems, the specific mechanisms of failure initiation and progression in prosthetic loosening have not been completely understood. Harris et al. [3,20] suggested that the early separation between prosthesis-cement resulted in an acceleration of the loosening process. This suggestion was based on experimental studies which showed that loose components were easily removed from cement and there were few fibrous membranes between cement and bone in revision arthroplasty [8,21,22,23]. Even in revision TKA for aseptic loosening, debonding between prosthesis-cement in surgical findings was reported by retrieval studies [24,25,26]. We also experienced the dissociation of prosthesis-cement in all cases of revision TKA for aseptic loosening. These results and observations suggested that increasing prosthesis-cement bond strength might effectively prevent early aseptic loosening.
Various surface treatments in orthopaedic prosthesis have been employed to enhance the ability of prostheses to bond with cement; polishing, porous coatings, and roughening of textures by sand-blasting [9]. Pittman et al. [5] reported a mechanical study about surface roughness of total knee prosthesis and demonstrated that prosthesis-cement bonding strength increased with increasing surface roughness. However, no study had been performed to determine whether increasing prosthesis surface roughness is clinically desirable or whether it affects rates of aseptic loosening after TKA. Kutzner et al. [26] reported, by a case-control study with retrieval analyses, that the comparatively low surface roughness made tibial baseplate more susceptible to mechanical loosening. However, they compared two different prosthesis designs, that is, Low-Contact Stress, Ra = 3.7 μm (DePuy Synthes, Warsaw, IN, USA) and Profix, Ra = 9.1 μm (Smith and Nephew, Memphis, TN, USA). In our present study, we compared prosthesis with identical designs but with different surface roughnesses (Ra, 5.0 μm vs. 11.6 μm) and observed that the rougher prosthesis (Ra = 11.6 μm) had a lower revision rate due to aseptic loosening and lower tibial osteolysis and/or radiolucent line development rates. Our results provide clinical support for the results of the mechanical study by Pittman et al. [5] that showed prosthesis-cement bonding strength increased as the surface roughness increased and suggests that using the roughened total knee prosthesis is useful for preventing aseptic loosening.
Our results for TKA were quite different from those previously reported for hip arthroplasty. In hip arthroplasty, earlier studies reported that rough surfaced femoral stems were shown to be clinically inferior to polished femoral stems because rough stems produced more wear debris caused by stresses between cement and bone than polished femoral stems, resulting in more stem loosening through osteolysis [6,8,10,11]. However, in the present study, roughened surfaced total knee prosthesis had less incidence of loosening and radiologic tibial osteolysis by wear debris. Kutzner et al. [26], similar to our results, reported that the low surface roughness makes the prosthesis more susceptible to loosening. We believe that these differences between hip and knee arthroplasties were probably due to differences in bone quality where cemented prosthesis is attached. In order to reduce loosening, the bond strength ratios at both interfaces (prosthesis-cement and cement-bone) should be considered [27]. Increasing the bond strength at prosthesis-cement would cause high stresses at the cement-bone interface [28]. Interfaces between cement and bone can be classified as cement to cancellous bone or cement to cortical bone interfaces, and cement-cancellous bone bond strengths are much higher than those of cement-cortical bone strengths [27]. In hip arthroplasty, the femoral stems are typically in contact with femoral cortical bone, whereas in knee arthroplasty, tibial components contact cancellous bone. We believe that this difference explains why smooth undersurfaces are advantageous for hip arthroplasty, whereas roughened undersurfaces are a better option for knee arthroplasty.
In the present study, a roughened surface was associated with osteolysis at the tibial baseplate, but not with osteolysis of the femoral component. We think that this difference was because the femur with a femoral component had a higher portion of cortical bone than tibia with tibial baseplate [9]. Therefore, our results indicate that strengthening bonding at the prosthesis-cement interface by increasing surface roughness is a better clinical option when a prosthesis is fixed in cancellous bone.
However, the surface roughness of prosthesis with exceeding a certain Ra value can lead to cement damage [9]. It is questionable whether prosthesis with Ra over 11.6 μm can produce better clinical results because we only compared prosthesis with two different surface roughnesses. In addition, optimal surface roughness depends on many factors such as prosthesis shape and geometry, loading modes, and the physical properties of bone and cement [9]. For these reasons, it is difficult to formulate quantitative specifications for prostheses surface roughness. Further research on this topic should be performed by comparing prosthesis with various surface roughnesses.
The present study contains several limitations. First, follow-up periods differed in the two groups. To account for this, we compared clinical and radiological outcomes and prosthesis survival rates in the two groups at the same time points. Second, the cementing technique, which could affect prosthesis-cement bonding strength, was not considered as a risk factor of aseptic loosening, and differences between cement compositions, timings, and curing temperatures may have affected the results. However, we tried to reduce these differences by using the same cementing technique (modern cementing technique) [14] and the same bone cement in all patients. Despite these limitations, our findings are meaningful as they provide evidence of the clinical effects on using prosthesis with identical designed but different surface roughness, and provide a rationale for how to treat undersurface of the total knee prosthesis to prevent aseptic loosening.
5. Conclusions
Differences in the undersurface roughness of total knee prosthesis were associated with clinical and radiological outcomes and revision rates for aseptic loosening. The more roughened undersurface (Ra = 11.6) resulted in better functional outcomes and the lower rate of revision for aseptic loosening. The roughened undersurface was a significant risk factor for aseptic loosening, but did not affect the osteolysis of femoral component. Therefore, the use of roughened undersurface of tibial baseplate would be a way to prevent aseptic loosening.
Author Contributions
Conceptualization, K.H.M.; Data curation, S.H.K.; Formal analysis, S.H.K.; Investigation, S.H.K.; Software, S.H.K.; Supervision, K.H.M.; Visualization, S.H.K.; Writing—original draft, S.H.K.; Writing—review and editing, S.H.K. and K.H.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Acknowledgments
This work was supported by an Inha University Research Grant.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Lachiewicz, P.F.; Soileau, E.S. The rates of osteolysis and loosening associated with a modular posterior stabilized knee replacement. Results at five to fourteen years. J. Bone Joint Surg Am. 2004, 86, 525–530. [Google Scholar] [CrossRef] [PubMed]
- Lombardi, A.V., Jr.; Berasi, C.C.; Berend, K.R. Evolution of tibial fixation in total knee arthroplasty. J. Arthroplast. 2007, 22, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Jasty, M.; Maloney, W.J.; Bragdon, C.R.; O’Connor, D.O.; Haire, T.; Harris, W.H. The initiation of failure in cemented femoral components of hip arthroplasties. J. Bone Jt. Surg. 1991, 73, 551–558. [Google Scholar] [CrossRef]
- Vanlommel, J.; Luyckx, J.P.; Labey, L.; Innocenti, B.; De Corte, R.; Bellemans, J. Cementing the tibial component in total knee arthroplasty: Which technique is the best? J. Arthroplast. 2011, 26, 492–496. [Google Scholar] [CrossRef] [PubMed]
- Pittman, G.T.; Peters, C.L.; Hines, J.L.; Bachus, K.N. Mechanical bond strength of the cement-tibial component interface in total knee arthroplasty. J. Arthroplast. 2006, 21, 883–888. [Google Scholar] [CrossRef] [PubMed]
- Shepard, M.F.; Kabo, J.M.; Lieberman, J.R. The Frank Stinchfield Award. Influence of cement technique on the interface strength of femoral components. Clin. Orthop. Relat. Res. 2000, 381, 26–35. [Google Scholar] [CrossRef]
- Zelle, J.; Janssen, D.; Peeters, S.; Brouwer, C.; Verdonschot, N. Mixed-mode failure strength of implant–cement interface specimens with varying surface roughness. J. Biomech. 2011, 44, 780–783. [Google Scholar] [CrossRef] [Green Version]
- Cho, W.S. Knee Joint Arthroplasty; Springer: Berlin/Heidelberg, Germany, 2014. [Google Scholar]
- Hung, J.P.; Bai, Y.W.; Hung, C.Q.; Lee, T.E. Biomechanical performance of the cemented hip stem with different surface finish. Appl. Sci. 2019, 9, 4082. [Google Scholar] [CrossRef] [Green Version]
- Mohler, C.G.; Callaghan, J.J.; Collis, D.K.; Johnston, R.C. Early loosening of the femoral component at the cement prosthesis interface after total hip replacement. J. Bone Jt. Surg. 1995, 77, 1315–1322. [Google Scholar] [CrossRef]
- Manley, M.T.; Stern, L.S.; Gurtowski, J. The load carrying and fatigue properites of the stem cement interface with smooth and porous coated femoral components. J. Biomed. Mater. Res. 1985, 19, 563–575. [Google Scholar] [CrossRef]
- Moon, K.H.; Hong, S.H.; Hong, T.H. Total knee replacement arthroplasty with Buechel and Pappas knee: Minimum 2-year follow-up. Clin. Orthop. Surg. 2015, 7, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Gotman, I.; Gutmanas, E.Y. Titanium nitride-based coatings on implantable medical devices. Adv. Biomater. Devices Med. 2014, 1, 53–73. [Google Scholar]
- Zimmer Biomet. Modern Cementing Technique. Available online: https://www.zimmerbiomet.com/content/dam/zimmer-biomet/medical-professionals/common/cement/modern-cementing-technique-brochure.pdf (accessed on 1 May 2020).
- Insall, J.N.; Dorr, L.D.; Scott, R.D.; Scott, W.N. Rationale of the Knee Society clinical rating system. Clin. Orthop. Relat. Res. 1989, 248, 13–14. [Google Scholar] [CrossRef]
- Gioe, T.J.; Killeen, K.K.; Grimm, K.; Mehle, S.; Scheltema, K. Why are total knee replacements revised? Analysis of early revision in a community knee implant registry. Clin. Orthop. Relat. Res. 2004, 428, 100–106. [Google Scholar] [CrossRef]
- Guha, A.R.; Debnath, U.K.; Graham, N.M. Radiolucent lines below the tibial component of a total knee replacement (TKR)—A comparison between single-and two-stage cementation techniques. Int. Orthop. 2008, 32, 453–457. [Google Scholar] [CrossRef] [Green Version]
- Durig, N.; Pace, T.; Broome, B.; Osuji, O.; Harman, M.K. Clinical outcomes of tibial components with modular stems used in primary TKA. Adv. Orthop. 2014, 2014, 651279. [Google Scholar] [CrossRef] [Green Version]
- Lum, Z.C.; Shieh, A.K.; Dorr, L.D. Why total knees fail—A modern perspective review. World J. Orthop. 2018, 18, 60–64. [Google Scholar] [CrossRef]
- Harris, W.H. Is it advantageous to strengthen the cement–metal interface and use a collar for cemented femoral components of total hip replacement? Clin. Orthop. 1992, 285, 67–72. [Google Scholar] [CrossRef]
- Maloney, W.J.; Jasty, M.; Burke, D.W.; O’Connor, D.O.; Zalenski, E.B.; Bragdon, C.; Harris, W.H. Biomechanical and histologic investigation of emented total hip arthroplasties. A study of autopsy-retrieved femurs after in vivo cycling. Clin. Orthop. Relat. Res. 1989, 249, 129–140. [Google Scholar]
- Stauffer, R.N. Ten-year follow-up study of total hip replacement. J. Bone Joint Surg. Am. 1982, 64, 983–990. [Google Scholar] [CrossRef]
- Fornasier, V.L.; Cameron, H.U. The femoral stem/cement interface in total hip replacement. Clin. Orthop. Relat. Res. 1976, 116, 248–252. [Google Scholar] [CrossRef]
- Mikulak, S.A.; Mahoney, O.M.; dela Rosa, M.A.; Schmalzried, T.P. Loosening and osteolysis with the press-fit condylar posterior-cruciate-substituting total knee replacement. J. Bone Joint Surg. Am. 2001, 83, 398–403. [Google Scholar] [CrossRef] [PubMed]
- Han, H.S.; Kang, S.B.; Yoon, K.S. High incidence of loosening of the femoral component in legacy posterior stabilised-flex total knee replacement. J. Bone Joint Surg. Br. 2007, 89, 1457–1461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kutzner, I.; Hallan, G.; Høl, P.J.; Furnes, O.; Gøthesen, Ø.; Figved, W.; Ellison, P. Early aseptic loosening of a mobile-bearing total knee replacement. Acta Orthop. 2018, 89, 77–83. [Google Scholar] [CrossRef] [Green Version]
- Van de Groes, S.; de Waal-Malefijt, M.; Verdonschot, N. Probability of mechanical loosening of the femoral component in high flexion total knee arthroplasty can be reduced by rather simple surgical techniques. Knee 2014, 21, 209–215. [Google Scholar] [CrossRef] [Green Version]
- Arola, D.; Stoffel, K.A.; Yang, D.T. Fatigue of the cement/bone interface: The surface texture of bone and loosening. J. Biomed. Mater. Res. B Appl. Biomater. 2006, 76, 287–297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Figure 1.
The schematized surface treatment process of Buechel and Pappas knee prosthesis (L-F Knee System, Cellumed Co., Ltd., Seoul, Korea) used in this study. The undersurface treatment process of the prosthesis was changed from (A) to (B) in late 2013.
Figure 1.
The schematized surface treatment process of Buechel and Pappas knee prosthesis (L-F Knee System, Cellumed Co., Ltd., Seoul, Korea) used in this study. The undersurface treatment process of the prosthesis was changed from (A) to (B) in late 2013.

Figure 2.
Photograph of Buechel and Pappas knee prosthesis (L-F Knee System, Cellumed Co., Ltd., Seoul, Korea) used in this study. The undersurface of the prosthesis was changed from (A) to (B) in late 2013.
Figure 2.
Photograph of Buechel and Pappas knee prosthesis (L-F Knee System, Cellumed Co., Ltd., Seoul, Korea) used in this study. The undersurface of the prosthesis was changed from (A) to (B) in late 2013.

Figure 3.
A flowchart of patient selection for this study (total knee arthroplasty (TKA), osteoarthritis (OA)).
Figure 3.
A flowchart of patient selection for this study (total knee arthroplasty (TKA), osteoarthritis (OA)).

Figure 4.
The Kaplan-Meier survival curve with revision (A) for any reason or (B) for aseptic loosening as endpoint. Patients were categorized into two groups according to the undersurface roughness (Ra) of the prosthesis used in total knee arthroplasty: Ra = 5.0 μm (Group A) and Ra = 11.6 μm (Group B).
Figure 4.
The Kaplan-Meier survival curve with revision (A) for any reason or (B) for aseptic loosening as endpoint. Patients were categorized into two groups according to the undersurface roughness (Ra) of the prosthesis used in total knee arthroplasty: Ra = 5.0 μm (Group A) and Ra = 11.6 μm (Group B).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Patient demographic characteristics.
| Variable | Group A Ra = 5.0 μm (272 Knees in 175 Patients) | Group B Ra = 11.6 μm (275 Knees in 187 Patients) | p Value |
|---|---|---|---|
| Mean age at surgery (years, range) a | 68.2 ± 8.0 (45–92) | 67.6 ± 7.6 (47–93) | 0.481 |
| Gender (n, %) b | – | – | 0.494 |
| Male | 21 (12.0%) | 27 (14.4%) | |
| Female | 154 (88.0%) | 160 (85.6%) | |
| Duration of follow-up (months, range) a | 69.7 ± 25.6 (36–125) | 51.0 ± 10.6 (36–73) | 0.001 * |
| Body Mass Index (kg/m2) a | 26.1 ± 3.7 | 26.5 ± 3.9 | 0.296 |
| Bone Mineral Density (T-score) a | −1.83 ± 1.16 | −1.88 ± 1.11 | 0.768 |
| Knees (n, %) b | – | – | – |
| Bilateral | 97 (55.4%) | 88 (47.1%) | 0.111 |
| Unilateral | 78 (44.6%) | 99 (52.9%) | |
| Right | 42 (53.8%) | 53 (53.5%) | 0.967 |
| Left | 36 (46.2%) | 46 (46.5%) |
a Data presented as mean ± standard deviation. Statistical significance was determined by independent t-test; b Data presented as number (%). Statistical significance was determined by Pearson’s chi-squared test; * p < 0.05. Statistical significance was defined as p < 0.05; Ra, Average roughness.
Table 2.
Clinical and radiological outcomes.
| Variable | Group A Ra = 5.0 μm (272 Knees in 175 Patients) | Group B Ra = 11.6 μm (275 Knees in 187 Patients) | p Value |
|---|---|---|---|
| Range of motion a | – | – | – |
| Preoperative flexion contracture (°) | 2.3 ± 5.0 | 2.0 ± 4.9 | 0.399 |
| Postoperative flexion contracture (°) | 0.37 ± 3.23 | 0.39 ± 1.82 | 0.950 |
| Preoperative range of motion (°) | 121.5 ± 13.0 | 119.7 ± 9.8 | 0.154 |
| Postoperative range of motion (°) | 118.1 ± 14.0 | 120.1 ± 9.1 | 0.164 |
| Outcome scores a | – | – | – |
| Preoperative clinical AKSS | 68.1 ± 8.5 | 67.1 ± 5.4 | 0.276 |
| Postoperative clinical AKSS | 95.2 ± 7.6 | 95.8 ± 7.3 | 0.515 |
| Preoperative functional AKSS | 65.7 ± 7.2 | 64.0 ± 11.5 | 0.279 |
| Postoperative functional AKSS | 83.2 ± 20.5 | 88.8 ± 17.3 | 0.023 * |
| Complications b | – | – | – |
| Superficial infection | 1 (0.4%) | 0 (0%) | 0.497 |
| Hypertrophic synovitis | 1 (0.4%) | 0 (0%) | 0.497 |
| Deep vein thrombosis | 3 (1.1%) | 4 (1.5%) | >0.999 |
| Stiffness after TKA | 8 (2.9%) | 7 (2.5%) | 0.800 |
| Revision surgery b | – | – | – |
| Any reason | 13 (4.8%) | 5 (1.8%) | 0.058 |
| Aseptic loosening | 9 (3.3%) | 2 (0.7%) | 0.035 * |
| Prosthetic joint infection | 4 (1.5%) | 2 (0.7%) | 0.448 |
| Periprosthetic fracture | 0 (0%) | 1 (0.4%) | >0.999 |
| Radiologic findings b | – | – | – |
| Femoral osteolysis | 7 (2.6%) | 2 (0.7%) | 0.105 |
| Femoral radiolucencies | 10 (5.7%) | 7 (2.5%) | 0.472 |
| Tibial osteolysis | 21 (7.7%) | 5 (1.8%) | 0.001 * |
| Tibial radiolucencies | 25 (9.2%) | 7 (2.5%) | 0.001 * |
a Data presented as mean ± standard deviation. Statistical significance was determined by independent t-test or Mann-Whitney U-test; b Data presented as number (%). Statistical significance was determined by Fisher exact test; * p < 0.05. Statistical significance was defined as p < 0.05; Ra, Average roughness; AKSS, American Knee Society score; TKA, total knee arthroplasty.
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Ko, S.H.; Moon, K.H. Comparison of the Clinical Results of Identically Designed Total Knee Prostheses with Different Surface Roughnesses. Coatings 2020, 10, 486. https://doi.org/10.3390/coatings10050486
AMA Style
Ko SH, Moon KH. Comparison of the Clinical Results of Identically Designed Total Knee Prostheses with Different Surface Roughnesses. Coatings. 2020; 10(5):486. https://doi.org/10.3390/coatings10050486
Chicago/Turabian StyleKo, Sang Hyun, and Kyoung Ho Moon. 2020. "Comparison of the Clinical Results of Identically Designed Total Knee Prostheses with Different Surface Roughnesses" Coatings 10, no. 5: 486. https://doi.org/10.3390/coatings10050486
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.