
Abstract
Previous studies have reported superiority of mechanistic target-of-rapamycin (mTOR) antagonists (mTA) over calcineurin inhibitors (CNI) as part of maintenance immunosuppression (IS) in mitigating cardiac allograft vasculopathy (CAV) after heart transplantation (HT). MEDLINE and EMBASE were searched through October 2019 for studies comparing maintenance IS with mTA + antimetabolites (AM), CNI + mTA or CNI + AM post HT. The main outcomes were all-cause mortality, CAV, acute rejection, CMV infections, and change in eGFR. To compare different IS antagonists, a random-effects network meta-analysis was performed. We used p-scores to rank best treatments per outcome. Our search identified fifteen eligible studies (5 studies comparing mTA + AM vs. CNI + AM, 9 comparing CNI + mTA vs. CNI + AM, 1 comparing mTA + AM vs. CNI + mTA, 8 using everolimus and 7 sirolimus as mTA) reporting the selected outcomes. We did not identify any statistical difference in all-cause mortality among the three IS regimens without heterogeneity among studies. CAV rates were significantly lower with CNI + mTA (odds ratio [OR] 0.53, 95% confidence interval [CI] 0.3–0.92). Acute rejection rates were significantly lower with CNI + AM (OR 0.26, 95% CI 0.12–0.56) and with CNI + mTA (OR 0.16, 95% CI 0.07–0.33) compared with mTA + AM without significant heterogeneity (I2 = 43%, p = 0.9). CMV infections were significantly lower with mTA + AM (OR 0.13, 95% CI 0.03–0.46) and with CNI + mTA (OR 0.27, 95% CI 0.2–0.38) compared with CNI + AM without heterogeneity. mTA + AM led to higher eGFR compared with CNI + AM (9.06 ml/min/1.73 m2, 95% CI 3.15–14.97) and CNI + Mta (9.64 ml/min/1.73 m2, 95% CI 0.91–18.36), but the heterogeneity among studies was significant. CNI + mTA ranked better for CAV (p = 0.78), and acute rejection (p = 0.99) while mTA + AM for CMV infection (p = 0.94) and improvement in renal function (p = 0.93) than other regimens. Different IS regimens have similar effects on survival post HT, but CNI + mTA was associated with lower CAV rates, and acute rejection, while mTA + AM with less CMV infection post HT.







Similar content being viewed by others

References
Lund LH, Edwards LB, Kucheryavaya AY, Benden C, Dipchand AI, Goldfarb S, Levvey BJ, Meiser B, Rossano JW, Yusen RD, Stehlik J (2015) The registry of the International Society for Heart and Lung Transplantation: thirty-second official adult heart transplantation report--2015; focus theme: early graft failure. J Heart Lung Transplant 34(10):1244–1254
Topilsky Y, Hasin T, Raichlin E, Boilson BA, Schirger JA, Pereira NL, Edwards BS, Clavell AL, Rodeheffer RJ, Frantz RP, Maltais S, Park SJ, Daly RC, Lerman A, Kushwaha SS (2012) Sirolimus as primary immunosuppression attenuates allograft vasculopathy with improved late survival and decreased cardiac events after cardiac transplantation. Circulation. 125(5):708–720
Asleh R, Briasoulis A, Kremers WK, Adigun R, Boilson BA, Pereira NL, Edwards BS, Clavell AL, Schirger JA, Rodeheffer RJ, Frantz RP, Joyce LD, Maltais S, Stulak JM, Daly RC, Tilford J, Choi WG, Lerman A, Kushwaha SS (2018) Long-term sirolimus for primary immunosuppression in heart transplant recipients. J Am Coll Cardiol 71(6):636–650
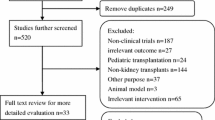
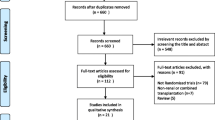
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC, Ioannidis JP, Clarke M, Devereaux PJ, Kleijnen J, Moher D (2009) The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol 62:e1–e34
Higgins JP, Altman DG, Gotzsche PC, Juni P, Moher D, Oxman AD, Savovic J, Schulz KF, Weeks L, Sterne JA (2011) The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. Bmj 343:d5928
Neupane B, Richer D, Bonner AJ, Kibret T, Beyene J (2014) Network meta-analysis using R: a review of currently available automated packages. PLoS One 9:e115065
Higgins JP, Thompson SG, Deeks JJ, Altman DG (2003) Measuring inconsistency in meta-analyses. Bmj 327:557–560
Rucker G, Schwarzer G (2015) Ranking treatments in frequentist network meta-analysis works without resampling methods. BMC Med Res Methodol 15:58
Andreassen AK, Andersson B, Gustafsson F, Eiskjaer H, Radegran G, Gude E, Jansson K, Solbu D, Karason K, Arora S, Dellgren G, Gullestad L (2016) Everolimus initiation with early calcineurin inhibitor withdrawal in de novo heart transplant recipients: three-year results from the randomized SCHEDULE study. Am J Transplant 16:1238–1247
Arora S, Ueland T, Wennerblom B, Sigurdadottir V, Eiskjaer H, Botker HE, Ekmehag B, Jansson K, Mortensen SA, Saunamaki K, Simonsen S, Gude E, Bendz B, Solbu D, Aukrust P, Gullestad L (2011) Effect of everolimus introduction on cardiac allograft vasculopathy--results of a randomized, multicenter trial. Transplantation 92:235–243
Bara C, Dengler T, Hack MA, Ladenburger S, Lehmkuhl HB (2013) A 1-year randomized controlled study of everolimus versus mycophenolate mofetil with reduced-dose cyclosporine in maintenance heart transplant recipients. Transplant Proc 45:2387–2392
Eisen HJ, Kobashigawa J, Starling RC, Pauly DF, Kfoury A, Ross H, Wang SS, Cantin B, Van Bakel A, Ewald G, Hirt S, Lehmkuhl H, Keogh A, Rinaldi M, Potena L, Zuckermann A, Dong G, Cornu-Artis C, Lopez P (2013) Everolimus versus mycophenolate mofetil in heart transplantation: a randomized, multicenter trial. Am J Transplant 13:1203–1216
Gleissner CA, Doesch A, Ehlermann P, Koch A, Sack FU, Katus HA, Dengler TJ (2006) Cyclosporine withdrawal improves renal function in heart transplant patients on reduced-dose cyclosporine therapy. Am J Transplant 6:2750–2758
Groetzner J, Kaczmarek I, Schulz U, Stegemann E, Kaiser K, Wittwer T, Schirmer J, Voss M, Strauch J, Wahlers T, Sohn HY, Wagner F, Tenderich G, Stempfle HU, Mueller-Ehmsen J, Schmid C, Vogeser M, Koch KC, Reichenspurner H, Daebritz S, Meiser B, Reichart B (2009) Mycophenolate and sirolimus as calcineurin inhibitor-free immunosuppression improves renal function better than calcineurin inhibitor-reduction in late cardiac transplant recipients with chronic renal failure. Transplantation 87:726–733
Guethoff S, Stroeh K, Grinninger C, Koenig MA, Kleinert EC, Rieger A, Mayr T, von Ziegler F, Reichart B, Hagl C, Schramm R, Kaczmarek I, Meiser BM (2015) De novo sirolimus with low-dose tacrolimus versus full-dose tacrolimus with mycophenolate mofetil after heart transplantation--8-year results. J Heart Lung Transplant 34:634–642
Gullestad L, Mortensen SA, Eiskjaer H, Riise GC, Mared L, Bjortuft O, Ekmehag B, Jansson K, Simonsen S, Gude E, Rundqvist B, Fagertun HE, Solbu D, Iversen M (2010) Two-year outcomes in thoracic transplant recipients after conversion to everolimus with reduced calcineurin inhibitor within a multicenter, open-label, randomized trial. Transplantation 90:1581–1589
Keogh A, Richardson M, Ruygrok P, Spratt P, Galbraith A, O'Driscoll G, Macdonald P, Esmore D, Muller D, Faddy S (2004) Sirolimus in de novo heart transplant recipients reduces acute rejection and prevents coronary artery disease at 2 years: a randomized clinical trial. Circulation 110:2694–2700
Lehmkuhl HB, Arizon J, Vigano M, Almenar L, Gerosa G, Maccherini M, Varnous S, Musumeci F, Hexham JM, Mange KC, Livi U (2009) Everolimus with reduced cyclosporine versus MMF with standard cyclosporine in de novo heart transplant recipients. Transplantation 88:115–122
Mancini D, Pinney S, Burkhoff D, LaManca J, Itescu S, Burke E, Edwards N, Oz M, Marks AR (2003) Use of rapamycin slows progression of cardiac transplantation vasculopathy. Circulation 108:48–53
Vigano M, Tuzcu M, Benza R, Boissonnat P, Haverich A, Hill J, Laufer G, Love R, Parameshwar J, Pulpon LA, Renlund D, Abeywickrama K, Cretin N, Starling RC, Eisen HJ (2007) Prevention of acute rejection and allograft vasculopathy by everolimus in cardiac transplants recipients: a 24-month analysis. J Heart Lung Transplant 26:584–592
White M, Boucher A, Dandavino R, Fortier A, Pelletier GB, Racine N, Ducharme A, de Denus S, Carrier M, Collette S (2014) Sirolimus immunoprophylaxis and renal histological changes in long-term cardiac transplant recipients: a pilot study. Ann Pharmacother 48:837–846
Zuckermann A, Keogh A, Crespo-Leiro MG, Mancini D, Vilchez FG, Almenar L, Brozena S, Eisen H, Tai SS, Kushwaha S (2012) Randomized controlled trial of sirolimus conversion in cardiac transplant recipients with renal insufficiency. Am J Transplant 12:2487–2497
Barten MJ, Hirt SW, Garbade J, Bara C, Doesch AO, Knosalla C, Grinninger C, Stypmann J, Sieder C, Lehmkuhl HB, Porstner M, Schulz U (2019) Comparing everolimus-based immunosuppression with reduction or withdrawal of calcineurin inhibitor reduction from six months after heart transplantation: the randomized MANDELA study. Am J Transplant 18. https://doi.org/10.1111/ajt.15361
König S, Browne S, Doleschal B, Schernthaner M, Poteser M, Mächler H, Wittchow E, Braune M, Muik M, Romanin C, Groschner K (2013) Inhibition of orai1-mediated Ca(2+) entry is a key mechanism of the antiproliferative action of sirolimus in human arterial smooth muscle. Am J Physiol Heart Circ Physiol 305(11):H1646–H1657
Kaczmarek I, Zaruba MM, Beiras-Fernandez A, Reimann R, Nickel T, Grinninger C, Sadoni S, Hagl C, Meiser B (2013) Tacrolimus with mycophenolate mofetil or sirolimus compared with calcineurin inhibitor-free immunosuppression (sirolimus/mycophenolate mofetil) after heart transplantation: 5-year results. J Heart Lung Transplant 32(3):277–284
Zakliczynski M, Nozynski J, Kocher A, Lizak MK, Zakliczynska H, Przybylski R, Wojarski J, Zembala M (2007) Surgical wound-healing complications in heart transplant recipients treated with rapamycin. Wound Repair Regen 15(3):316–321
Delgado JF, Torres J, JoséRuiz-Cano M, Sánchez V, Escribano P, Borruel S, María Cortina J, de la Calzada CS (2006) Sirolimus-associated interstitial pneumonitis in 3 heart transplant recipients. J Heart Lung Transplant 25(9):1171–1174
Asleh R, Briasoulis A, Pereira NL, Edwards BS, Frantz RP, Daly RC, Lerman A, Kushwaha SS (2018) Hypercholesterolemia after conversion to sirolimus as primary immunosuppression and cardiac allograft vasculopathy in heart transplant recipients. J Heart Lung Transplant 37(11):1372–1380
Asleh R, Clavell AL, Pereira NL, Smith B, Briasoulis A, Alnsasra H, Kremers WK, Habermann TM, Otley CC, Li X, Edwards BS, Stulak JM, Daly RC, Kushwaha SS (2019) Incidence of malignancies in patients treated with sirolimus following heart transplantation. J Am Coll Cardiol 73(21):2676–2688
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
Funnel plot for assessment of publication bias. (JPG 93 kb).
Rights and permissions
About this article

{kind=link}
Cite this article
Ueyama, H., Kuno, T., Takagi, H. et al. Maintenance immunosuppression in heart transplantation: insights from network meta-analysis of various immunosuppression regimens. Heart Fail Rev 27, 869–877 (2022). https://doi.org/10.1007/s10741-020-09967-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10741-020-09967-3