
Abstract
Background
Children are at high risk of suffering health consequences of air pollution and childhood exposure can increase the risk of developing chronic diseases in adulthood. This study, part of the MAPEC_LIFE project (LIFE12 ENV/IT/000614), aimed to investigate the associations between exposure to urban air pollutants and micronucleus (MN) frequency, as a biomarker of chromosomal damage, in buccal cells of children for supporting implementation and updating of environmental policy and legislation.
Methods
This prospective epidemiological cohort study was carried out on 6- to 8-year-old children living in five Italian towns with different levels and features of air pollution. Exfoliated buccal cells of the children were sampled twice, in winter and spring, obtaining 2139 biological samples for genotoxicological investigation. Micronucleus (MN) frequency was investigated in buccal cells of children and its association with air pollution exposure was assessed applying multiple Poisson regression mixed models, including socio-demographic and lifestyle factors as confounders. We also dichotomize air pollutants’ concentration according to the EU Ambient Air Quality Directives and WHO Air Quality Guidelines in all Poisson regression models to assess their risk predictive capacity.
Results
Positive and statistically significant associations were found between MN frequency and PM10, PM2.5, benzene, SO2 and ozone. The increment of the risk of having MN in buccal cells for each μg/m3 increase of pollutant concentration was maximum for benzene (18.9%, 95% CIs 2.2–38.4%) and modest for the other pollutants (between 0.2 and 1.4%). An increased risk (between 17.9% and 59.8%) was found also for exposure to PM10, benzene and benzo(a)pyrene levels higher than the threshold limits.
Conclusions
Some air pollutants are able to induce chromosomal damage in buccal cells of children even at concentrations below present EU/WHO limits. This type of biological effects may be indicative of the environmental pressure which populations are exposed to in urban areas.
Similar content being viewed by others

Background
According to the 2018 Environmental Performance Index [1], poor air quality is the greatest environmental threat to public health. In 2017, more than 90% of people worldwide live in areas that exceed the World Health Organization (WHO) Guidelines for healthy air. Air pollution contributed to almost 5 million deaths (nearly 1 in every 10) and 147 million years of healthy life lost, globally, and it reduces life expectancy on average by 1 year and 8 months [2]. Air pollution exposure has been linked to a wide range of diseases [3,4,5], among which heart disease and stroke are the most common, followed by lung diseases and lung cancer [6]. More recently, maternal exposure to outdoor air pollution has been associated with adverse impacts on fertility, pregnancy, newborns and children, and some evidence emerged on the association between exposure to air pollution and new onset type 2 diabetes in adults and with obesity, systemic inflammation, aging, Alzheimer’s disease, dementia [6] and autoimmune diseases [7]. In 2013, the International Agency for Research on Cancer (IARC) classified outdoor air pollution and particulate matter as carcinogenic to humans (Group 1), specifically via genotoxic pathways [8]. In particular, the IARC reported that human exposure to outdoor air pollution or particulate matter is associated with increases in genetic damage that have been shown to be predictive of cancer in humans [8].
Compared to adults, children are at higher risk of suffering health consequences of airborne chemicals for their higher exposure and susceptibility [9]. Even low-dose exposure to air pollutants during windows of vulnerability in utero and in early infancy can result in disease, disability, and death in childhood and across lifespan [10]. Really, some data suggest that genetic damage occurring early in life may affect the risk of developing chronic diseases, including cancer, in adulthood more than later damage events [11, 12].
In the last decades, studies on the health effects of air pollution have increasingly used a molecular epidemiological approach, investigating biological and genotoxic effects in cells of exposed subjects [13]. The use of biomarkers in the investigation of health effects of air pollution, as well as other exposures, could improve exposure assessment, increase the understanding of mechanisms and allow the investigation of individual susceptibility [14]. Measuring biomarkers of early effects, detectable a long time before clinical disease develops, allows a prompt detection of the biological consequences of a specific situation, such as the exposure to air pollutants. Moreover, some biomarkers of early effect, such as micronuclei, are predictive of cancer risk [15]. Furthermore, in contrast to disease monitoring, biomarkers of early effects are measurable in a wide number of individuals, providing a global pattern of the possible effects of total environmental exposures in a population. Today, almost all air pollution studies investigating human health effects employ some sort of biomarker [16] and the attention is more and more focused on the effects of early exposure, occurring during prenatal and childhood periods [17]. Despite this growth of molecular epidemiological studies on air pollution effects, the studies investigating the impact of this exposure on children are still few, with small sample size and poor evaluation of potential confounding factors.
This research is part of the MAPEC_LIFE project (Monitoring air pollution effects in children for supporting public health policy, http://www.mapec-life.eu), a prospective epidemiological cohort study funded by the EU Life + Programme (LIFE12 ENV/IT/000614). The aim was to investigate the associations between exposure to urban air pollutants and micronucleus frequency, as a biomarker of chromosomal damage, in exfoliated buccal cells of children, taking into account socio-demographic and lifestyle factors as confounders. The results of this investigation could contribute to a better understanding of the impact of this major environmental issue on children health, providing a concrete contribution to the implementation and updating of environmental policy and legislation.
Results
The project was started in November 2014 and involved 26 schools in five towns. Among the 3144 candidate children, 1767 (56.2%) agreed to participate and 1356 of them were eligible for the research (Fig. 1). Of these, 1317 children were included in the study, providing buccal cell samples in winter, and 1149 of them provided again their buccal cells in spring. Therefore, 1149 of 1317 initial participants (87%) provided a double biological sample. After excluding samples unsuitable for laboratory analysis, 2139 biological samples were analyzed, 1093 of which collected in winter and 1046 in spring. The majority of cell samples showed no micronucleus (MN) (55.5%) or MN frequency between 0.5 and 2 MN/1000 cells (43.8%), while only 0.7% of the samples showed an MN frequency higher than 2 MN/1000 cells (Fig. 2).

Flow diagram describing subjects’ selection and inclusion in the study

MN frequency (MN/1000 cells) in buccal cells of children
The levels of air pollutants monitored by the Regional Agencies of Environmental Protection (ARPAs) (PM10, PM2.5, benzene, NO2, SO2, O3) in the 3 weeks preceding the biological samplings in winter and spring are shown in Additional file 1: Table S1. As expected, the mean levels of the pollutants were higher in winter than in spring, except for ozone, which showed higher concentration in spring than in winter. However, almost no children were exposed to benzene levels higher than the EU limit and no one was exposed to SO2 and O3 levels over both the EU and WHO thresholds.
The application of the univariate mixed Poisson regression models showed associations between MN frequency and town of residence and temperature (Table 1). All the towns showed lower Incidence Rate Ratios (IRRs) for MN frequency than Brescia, considered as the reference. MN frequency showed a negative association with temperature. Also sampling season was associated with MN frequency (data not shown), but, since season and temperature were collinear, only the latter was retained in the models because it was a continuous variable and therefore more informative than season. However, for ozone, the Poisson model included a cubic spline for the day of the year instead of temperature, due to the seasonal trend of the ozone, which is higher in spring–summer than in winter. Using the mixed Poisson regression models including temperature and town of residence as confounding factors, we found that MN frequency was positively associated with body mass index (BMI) and exposure to second-hand smoke at home and negatively associated with adherence to Mediterranean diet and parent’s education (Table 1). The complete results regarding the associations between MN frequency and all the data retrieved by questionnaire are reported in Additional file 1: Table S2.
The Poisson regression mixed models including all the variables in Table 1 as confounding factors showed a positive, though not statistically significant association between MN frequency and concentration of polycyclic aromatic hydrocarbons (PAHs), their nitro-compounds (nitroPAHs), carcinogenic PAHs (cPAHs) and benzo(a)pyrene (BaP) in PM0.5 samples (Table 2). The strongest associations were found for nitroPAHs (IRR = 1.391, 95% CIs 0.464–4.172, p = 0.556) and BaP (IRR = 1.205, 95% CIs 0.980–1.481, p = 0.078).
No relationship between MN frequency and in vitro PM0.5 mutagenicity was found including in the model the net revertant values obtained for all the strains of Salmonella typhimurium used in the Ames test (TA100, TA98, TA98NR, YG1021) (Table 3).
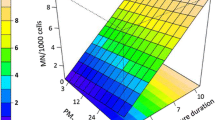
The analysis of the association between MN frequency and level of air quality parameters measured by ARPAs showed positive and statistically significant associations for PM10 (peak value of the previous 21 days), PM2.5 (peak value of the previous 21 days and mean value of the 15- to 21-day lag period), benzene (mean value of the 15- to 21-day lag period), SO2 (peak values of the previous 21 days) and ozone (peak values of the previous 21 days) (Table 4). Particularly, an 18.9% (95% CIs 2.2–38.4%) increment of the risk of having MN in buccal cells for each μg/m3 increase of benzene concentration was apparent, while the increase of the risk for the other associations was between 0.2% and 1.4% for one unit increase of the level of each pollutant.
The analysis regarding the complete set of pollutant measures is reported in Additional file 1: Table S3. Almost all the positive associations between MN frequency and air pollutant levels were observed for the exposure levels in the 3rd week before biological sampling, for all pollutants but SO2, for which a significant association was found also with the peak value of the previous 14 days. For ozone, positive associations were observed for almost all exposure measures.
To investigate the risk of having MN in buccal cells when exposure levels exceeded the thresholds established by the EU Ambient Air Quality Directives and WHO Air Quality Guidelines, the Poisson regression models were applied dichotomizing air pollutant levels at the thresholds. Considering EU Ambient Air Quality Directives, a positive association was found between MN frequency and PM10 exposure higher than the annual limit value of 40 μg/m3 in the 15- to 21-day lag period preceding the biological sampling, with an increase of the risk of 17.9% (95% CIs 0.6–38.1%, p = 0.042) (Table 5). On the other hand, considering WHO Air Quality Guidelines, the exposures to levels of PM10, benzene and BaP higher than the annual limits were associated with increased MN frequency. In particular, being exposed to pollutant concentration over the thresholds increased the risk of 22.5% (95% CIs 3.9–44.3%, p = 0.015) for PM10, of 27.8% (95% CIs 3.8–57.3%, p = 0.021) for benzene and of 59.8% (95% CIs 21.0–111.1%, p = 0.001) for BaP. The complete results of the analysis considering EU and WHO limits are reported in the Additional file 1: Tables S4 and S5.
Discussion
We investigated the association between MN frequency and air pollution exposure in 2139 buccal cell samples of primary school children living in five Italian towns. We found an increase of risk of having MN in buccal cells for an increase of the levels of benzene, ozone, PM2.5, PM10 and SO2 registered in the lag time of 15–21 days before cell sampling.
The ability of outdoor air pollution and of many of its components to induce different types of genetic effects, including MN formation, is supported by strong mechanistic evidence in both humans and experimental systems [8]. However, few studies investigated MN frequency in children exposed to air pollution. Most of them found higher MN frequencies in children exposed to high compared to low levels of air pollutants [33, 39,40,41,42,43,44], and some found a statistical association between MN frequency and single air pollutants. For example, Ceretti et al. [45] found an association with PM10 and NO2 in 181 buccal cells samples of preschool children in Brescia. Ozone was associated with MN frequency in both exfoliated buccal cells and peripheral blood lymphocytes of 64 children aged 4–12 years from USA [46]. BaP was associated with MN frequency evaluated in umbilical cord blood lymphocytes of 178 Czech newborns [42]. However, other studies provided negative or inconsistent results regarding the association between MN frequency and air pollutant exposure in children’s cells [47,48,49].
Micronuclei are small additional nuclei, formed of acentric chromosomal fragments or whole chromosomes that are not included in the main daughter nucleus during nuclear division (Fig. 3). They are stable cytogenetic alterations, which can represent early biological events along the pathway of cancer development and are associated with the chromosome instability phenotype often seen in cancer [50]. Actually, a significant increase of all cancer incidence was found in groups of subjects with high MN frequency in peripheral blood lymphocytes [15], identifying this biomarker as a predictive of cancer development. Moreover, MN frequency in peripheral lymphocytes of healthy individuals was associated with the risk of cardiovascular diseases [51] and neurodegenerative disorders [52]. Even if these associations have been found for MN detected in lymphocytes, they can be probably referred also to MN in buccal cells, for the strong correlation between MN frequency in these two types of cells [53, 54]. For this reason, we decided to measure MN frequency in exfoliated buccal cells, which are directly exposed to airborne compounds, can be collected by noninvasive sampling and can be analyzed without establishing cell culture [54]. The most significant exposure period for observing associations with MN frequency corresponded to the 15–21 days before biological sampling. This was consistent with the lifetime of the exfoliated buccal cells, which in 7–21 days differentiate and migrate from basal layer to the keratinized surface layer, and the mechanism of the MN formation, which needs that the stem basal cells, with the chromosomal damage, express it as MN during nuclear division [55, 56].

Image of buccal mucosa cells stained with the Feulgen plus Light Green method and observed through fluorescence microscopy (magnification 1000x). On the left, a differentiated cell without damage; on the right, a differentiated cell with three micronuclei
We also evaluated the association between MN frequency and air pollutant levels according to the limits established by the EU Ambient Air Quality Directives and WHO Air Quality Guidelines. The WHO guidelines seem more protective for exposure to PM10, benzene and BaP than the EU directives. However, they both were insufficient to protect children from the genotoxic activity of air pollutants. Indeed, we found positive association of MN frequency with PM2.5 and, even more, SO2 and ozone for which children’s exposure was under the EU and WHO limits. Similarly, conclusions of the ESCAPE project showed that exposure to particulate matter may increase the risk for lung cancer even at concentrations below the existing EU air quality limit values for PM10 (40 μg/m3) and PM2.5 (25 μg/m3) [57]. These results were consistent with the assumption for which a threshold for PM exposure below which no health damage is observed has not been identified [58].
Strengths and weaknesses of the study: This study has various strengths. First, it has a large sample size, including 2139 biological samples, collected in two seasons for 1149 children. To our knowledge, this is the largest sample size in studies investigating the association of MN frequency in children’s cells with air pollution. Second, the study recruited children living in five towns and in two different seasons, allowing to assess the effect of different mixtures of air pollutants, in the periods of the year with the highest and lowest levels of air pollutants in Italy.
This study has some limits, too. The main limit is the lack of evaluation of children’s personal exposure to air pollutants. Epidemiological studies often refer air pollutant levels to subjects’ residence [59]. However, we preferred to use daily levels of air pollutants measured by the ARPAs and PM0.5 sampling at school during biological sampling days because children involved stayed at school for quite the whole day and lived near the attended school. Nevertheless, indirect measures of exposure to other potential agents causing DNA damage were provided by questionnaires, as it is often done in epidemiological research of health effects of air pollution.
Conclusions
The MAPEC_LIFE project found an association between MN frequency detected in buccal cells of children and levels of some air pollutants, such as PM10, PM2.5, benzene, SO2 and ozone. These associations supported the role of air pollution exposure in inducing DNA damage, even at concentrations below present EU limits, which may be indicative of the environmental pressure which populations are exposed to in urban areas.
According to these results, some suggestions emerged for public health policy. First, apart from the routinely measured air quality parameters, some airborne pollutants, such as BaP, which induced biological damage, are candidates for air quality monitoring. Second, air pollution directives need to be constantly revised according to research findings, including these regarding early biological effects. Last, the buccal MN cytome assay is a simple, cost-effective and noninvasive test, which may be useful for monitoring air pollution biological effects. In particular, it may be used to detect specific exposure situations dangerous to health, to identify population groups with high susceptibility and to monitor the impact of interventions for ambient air pollution control.
Methods
The protocol of the study was described in detail in Feretti et al. [18]. In brief, the study was carried out on primary school children (6- to 8-year old) living in five Italian towns, characterized by different levels and features of air pollution. Brescia and Torino are located in North Italy, in the highly industrialized area of the Po Valley, one of the most polluted areas in Europe [6], where the theoretical increase of cancer risk for children due to benzene exposure estimated applying the standard United States Environmental Protection Agency (USEPA) methodology was found higher than acceptability threshold [19]. Pisa and Perugia are located in Central Italy, a medium–low polluted area. Lecce is located in a very low polluted area, in Southern Italy [20]. The project was approved by the Ethics Committees of the local Health Authorities of each town. Informed consent was obtained from children’s parents after an explanation of the intent of the study, possible results and their meaning. Only children whose parents filled in the consent form were included in the study. A comic assent form was also presented to children before biological sampling. The children who refused to provide buccal cell sample were excluded.
About 200 children were recruited from primary schools in each urban area. Children with severe diseases and those who had been exposed to antineoplastic agents, had undergone radiation therapy or X-rays in the previous 12 months, or had a dental prosthetic, were excluded. A cluster sampling design was adopted. The primary sampling unit was the school, which was randomly chosen in each town. Schools with less than 100 students were not considered. Furthermore, all children of the first, second and third classes of each selected school were asked to participate in the study.
Exfoliated buccal cells were sampled twice, in winter (between November 2014 and March 2015) and spring (between April and June 2015), which are characterized by very different concentration of air pollutants in Italy. Micronucleus (MN) frequency was measured as a biomarker of early effect, according to the buccal micronucleus cytome assay (BMCyt assay) procedure by Thomas and Fenech [21]. To reduce variability among centers, cells were collected and fixed by each recruiting unit and then sent to a unique laboratory for the slide preparation and analysis. For each subject, two coded slides were prepared and read blind by trained scorers that determined initially the frequency of different cell types in 1000 cells and then MN frequency among a minimum of 2000 differentiated cells. All the details of biological sampling procedure, test method and assay results were reported in Villarini et al. [22].
A questionnaire to collect information on socio-demographic and other features of the children was administered to children’s parents twice, before each biological sampling. It included questions about children’s exposures to genotoxic substances different from outdoor air pollution (indoor air pollution, second-hand smoke, consumption of food potentially containing genotoxic compounds), some lifestyle aspects (physical activity, time spent outside, dietary habits) and some parent’s characteristics (nation of birth, education level, employment status), which are potential confounding factors of the relationship between air pollution exposure and biomarkers of early effects. The analysis of reliability of the questionnaire and the socio-economic, lifestyle and socio-cultural characteristics of the children have been already published [23,24,25,26].
Child exposure to air pollution was evaluated by both collecting ultra-fine particulate matter (PM0.5) samples near the selected schools and gathering data about the concentration of the main air pollutants from the Regional Agencies of Environmental Protection (ARPAs). PM0.5 sampling was carried out in the area adjacent to each school in the same days of the biological sampling, using a high-volume air sampler which collected PM0.5 on fiberglass filters for 72 consecutive hours. Chemical analysis of the organic extracts of the samples was conducted to assess the concentration of polycyclic aromatic hydrocarbons (PAHs) and their nitro-compounds (nitroPAHs). Furthermore, in vitro genotoxicity was evaluated using Ames test on Salmonella typhimurium (TA100, TA98, TA98NR, YG1021 strains), cytokinesis-block MN (CBMN) test on A549 cells and comet assay on A549 and BEAS-2B cells. Methods and descriptive results of PM0.5 sampling and analysis were reported in Bonetta et al. [27].
We retrieved data on levels of the air pollutants regulated by the EU Ambient Air Quality Directives, i.e., PM10, PM2.5, NO2, SO2, benzene, O3 [28], which are measured daily by the Air Quality Monitoring Network of the ARPAs, accessing to the free databases on their websites [29,30,31,32,33] in the five towns during study period. Given the small size (less than 200.000 inhabitants) of four towns (Brescia, Perugia, Pisa and Lecce) and the small number of monitoring stations in each of them, the exposure level attributed to each child was calculated as the average of the levels detected by all the town stations. Torino, in contrast, is a big town (about 880.000 inhabitants), which has a large number of monitoring stations in the different urban areas that allowed us to couple a monitoring station to each school. As buccal cells have a maximum 3-week life, we assessed the associations between MN frequency and air pollutant concentrations in the 3 weeks before cell sampling. Various air pollutant measures were used: (a) averages of the daily concentrations of the 7, 14 and 21 days preceding the biological sampling, (b) averages of each of three 1-week lag periods before biological sampling (1–7, 8–14, 15–21 days) and (c) peak concentrations—i.e., maximum hourly concentrations—in the 7, 14 and 21 days preceding biological sampling. For PM10, also the number of exceedance days of the daily EU law limit (50 µg/m3) occurring in the 7, 14 and 21 days preceding biological sampling was considered.
Since meteorological conditions influence air pollutant levels and might determine health effects, we retrieved values of temperature, relative humidity, wind intensity and rainfall measured by the ARPAs during the period of the PM0.5 samplings. Since data on relative humidity, wind intensity and rainfall were not available for all the towns, only temperature was analyzed as a possible confounding factor for the relationship between MN frequency and air pollutants.
The sample size was determined considering the expected effect size, the natural variability of the study outcome, a type I error probability fixed at 5%, two sided, and a type II error probability fixed at 5%. Regarding effect size and natural variability, we used information from a previous study, which found a mean MN frequency of 1.43 (± 0.84) and 1.13 (± 0.63) per 1000 cells in children living in areas at higher and lower levels of PM2.5, respectively, with about 5 μg/m3 of mean difference between them during the study period [34]. A sample size of about 200 children per exposure level should have been large enough to assess a mean difference of 0.20 MN/1000 cells between exposed and non-exposed, using a two-tailed t-Student test for unpaired data and considering also the clustered sampling strategy applied. Estimating a loss of approximately 20% of samples, because of incomplete or incorrectly filled in questionnaires and/or an insufficient number of cells collected through biological sampling, an oversampling of participants was planned, resulting in about 240 children recruited per town.
Statistical analysis
The MN count was considered as the response variable in multiple Poisson regression models. The data were doubly structured, consisting in two repeated measure within subject at level one, and of grouped subjects per each sampled school, as primary sampling unit at level two. However, subjects with only one MN measure were also included. To account of this data structure, we specified a hierarchical mixed effect model with subject and school-specific random intercepts. Fitting the Poisson regression models, Incidence Rate Ratios (IRRs) for each independent variable were estimated with their 95% confidence intervals (95% CIs). We checked for over-dispersion and eventually provided robust standard error of the estimates.
The analysis plan was (1) modeling of town of residence, season and temperature; (2) inclusion of potential confounders and indirect measures of exposure obtained via questionnaire; and (3) inclusion of air pollutants’ data.
In the first step of the analysis, we described the univariate associations between MN frequency and town of residence, season and temperature. In the second step of the analysis, we evaluated the association of MN frequency with each demographic and exposure variable collected through the questionnaire by multiple hierarchical mixed effect Poisson regression models including town of residence and temperature. Some variables were dichotomized due to the small number of subjects in some categories: mother’s and father’s education level as high (university degree) vs low, score of adherence to Mediterranean diet as high (6–10 units) vs low. In the third step of the analysis, we assessed the association between MN frequency and air pollution exposure. Regarding PM0.5 samples collected near each school, we investigated the association with the concentration of PM0.5, PAHs, nitroPAHs, carcinogenic PAHs (cPAHs) and Benzo(a)pyrene (BaP) by multiple hierarchical mixed effect Poisson regression models including temperature, town of residence and the previously identified confounding factors at step 2. The association between MN frequency and in vitro PM0.5 mutagenicity was analyzed as well, including in the model the net revertant values obtained for all the strains of Salmonella typhimurium used in the Ames test (TA100, TA98, TA98NR, YG1021). Regarding the air pollutants monitored by ARPAs in each town, all the measures described above were considered for each pollutant. Temperature (or cubic spline for time trend for ozone, since the high collinearity between ozone and temperature), town of residence and confounding factors from the questionnaire selected as previously defined were included in the model too.
As stated above, air pollutant variables collected thorough ambient monitors were cluster-level variables, with each cluster corresponding to an enrolled school. The statistical models included a cluster-specific random effect to account for intraclass correlation.
Possible non-linearity in concentration–response function was assessed fitting a cubic spline or a restricted polynomial function. Interaction terms were tested by likelihood ratio tests.
We also took account, for seasonality, fitting a cubic spline on day of the year, although this approach can be conservative because we collected measurements only in a few months of the year.
To assess the risk predictive capacity of air quality legislation, concentration of air pollutants was dichotomized according to the threshold levels established in both the EU Ambient Air Quality Directives [28, 35] and the WHO Air Quality Guidelines [36, 37]. These dichotomous variables were included in the same Poisson regression model to assess their association with MN frequency, taking into account all confounding factors considered in previous analysis. We refined the models using a backward selection algorithm with inclusion criterion p < 0.05, according to VanderWeele and Shpitser [38].
All tests were two-tailed tests with p < 0.05. Statistical analyses were conducted using the STATA 14.2 statistical package (Stata Corp, College Station, TX, USA).
Availability of data and materials
Data on levels of the air pollutants regulated by the EU Ambient Air Quality Directives and measured by the Air Quality Monitoring Network in the five towns were retrieved on the free databases of the Regional Agencies for Environmental Protection (ARPAs), accessing their websites (see Reference list). All the other data and statistical code are available from the corresponding author (elisabetta.ceretti1@unibs.it)
Change history
29 July 2020
An amendment to this paper has been published and can be accessed via the original.
Abbreviations
- ARPAs:
-
Regional Agencies of Environmental Protection
- BaP:
-
Benzo(a)pyrene
- BMI:
-
Body mass index
- IARC:
-
International Agency for Research on Cancer
- IRR:
-
Incidence Rate Ratio
- MN:
-
Micronucleus
- PAHs:
-
Polycyclic aromatic hydrocarbons
- nitroPAHs:
-
Polycyclic aromatic hydrocarbon nitro-compounds
- cPAHs:
-
Carcinogenic polycyclic aromatic hydrocarbons
- USEPA:
-
United States Environmental Protection Agency
- WHO:
-
World Health Organization
References
Wendling ZA, Esty DC, Emerson JW et al The 2018 Environmental Performance Index Report. New Haven, CT: Yale Center for Environmental Law and Policy 2018. https://epi.envirocenter.yale.edu/node/36476
HEI. State of Global Air 2019. Special Report. Boston, Health Effects Institute, HEI, 2019
Burnett R, Chen H, Szyszkowicz M et al (2018) Global estimates of mortality associated with long-term exposure to outdoor fine particulate matter. Proc Natl Acad Sci USA 115:9592–9597. https://doi.org/10.1073/pnas.1803222115
Cohen AJ, Brauer M, Burnett R et al (2017) Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: an analysis of data from the Global Burden of Diseases Study 2015. Lancet 389:1907–1918. https://doi.org/10.1016/S0140-6736(17)30505-6
Thurston GD, Kipen H, Annesi-Maesano I et al (2017) A joint ERS/ATS policy statement: what constitutes an adverse health effect of air pollution? An analytical framework. Eur Respir J 49:1600419. https://doi.org/10.1183/13993003.00419-2016
EEA. Air quality in Europe—2018 Report. European Environment Agency, Copenhagen, Denmark. 2018
Zhao CN, Xu Z, Wu GC et al (2019) Emerging role of air pollution in autoimmune diseases. Autoimmun Rev 18:607–614. https://doi.org/10.1016/j.autrev.2018.12.010
IARC (International Agency for Research on Cancer). Outdoor air pollution. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans, 109 2015
WHO. Health aspects of air pollution. Results from the WHO project “Systematic review of health aspects of air pollution in Europe”. World Health Organisation. 2004
Landrigan PJ, Fuller R, Acosta NJR et al (2018) The Lancet Commission on pollution and health. Lancet 391:462–512. https://doi.org/10.1016/S0140-6736(17)32345-0
Holland N, Fucic A, Merlo DF et al (2011) Micronuclei in neonates and children: effects of environmental, genetic, demographic and disease variables. Mutagenesis 26:51–56. https://doi.org/10.1093/mutage/geq064
Wild CP, Kleinjans J (2003) Children and increased susceptibility to environmental carcinogens: evidence or empathy? Cancer Epidemiol Biomarkers Prev 12:1389–1394
Bennett DA, Waters MD (2000) Applying biomarker research. Environ Health Perspect 108:907. https://doi.org/10.1289/ehp.00108907
Vineis P, Husgafvel-Pursiainen K (2005) Air pollution and cancer: biomarker studies in human populations. Carcinogenesis 26:1846–1855. https://doi.org/10.1093/carcin/bgi216
Bonassi S, Znaor A, Ceppi M et al (2007) An increased micronucleus frequency in peripheral blood lymphocytes predicts the risk of cancer in humans. Carcinogenesis 28:625–631. https://doi.org/10.1093/carcin/bgl177
de Oliveira BF, Chacra AP, Frauches TS et al (2014) A curated review of recent literature of biomarkers used for assessing air pollution exposures and effects in humans. J Toxicol Environ Health B Crit Rev 17:369–410. https://doi.org/10.1080/10937404.2014.976893
Desai G, Chu L, Guo Y et al (2017) Biomarkers used in studying air pollution exposure during pregnancy and perinatal outcomes: a review. Biomarkers 22:489–501. https://doi.org/10.1080/1354750X.2017.1339294
Feretti D, Ceretti E, De Donno A et al (2014) Monitoring air pollution effects on children for supporting public health policy: the protocol of the prospective cohort mapec study. BMJ Open 4:e006096. https://doi.org/10.1136/bmjopen-2014-006096
De Donno A, De Giorgi M, Bagordo F et al (2018) Health risk associated with exposure to PM10 and benzene in three Italian towns. Int J Environ Res Public Health 15:1672. https://doi.org/10.3390/ijerph15081672
ISPRA. Stato dell’Ambiente 83/18. Qualità dell’ambiente urbano. XIV Rapporto. Roma: Istituto Superiore per la Protezione e la Ricerca Ambientale 2018
Thomas P, Fenech M (2011) Buccal micronucleus cytome assay. Methods Mol Biol 682:235–248. https://doi.org/10.1007/978-1-60327-409-8_17
Villarini M, Levorato S, Salvatori T et al (2018) Buccal micronucleus cytome assay in primary school children: a descriptive analysis of the MAPEC_LIFE multicenter cohort study. Int J Hyg Environ Health 221:883–892. https://doi.org/10.1016/j.ijheh.2018.05.014
Zani C, Donato F, Grioni S et al (2015) Feasibility and reliability of a questionnaire for evaluation of the exposure to indoor and outdoor air pollutants, diet and physical activity in 6–8-year-old children. Ann Ig 27:646–656. https://doi.org/10.7416/ai.2015.2056
Zani C, Ceretti E, Grioni S et al (2016) Are 6–8 year old Italian children moving away from the Mediterranean diet? Ann Ig 28:339–348. https://doi.org/10.7416/ai.2016.2114
Grassi T, De Donno A, Bagordo F et al (2016) Socioeconomic and environmental factors associated with overweight and obesity in children aged 6–8 years living in Five Italian cities (the MAPEC_LIFE Cohort). Int J Environ Res Public Health 13:1002. https://doi.org/10.3390/ijerph13101002
Bagordo F, De Donno A, Grassi T et al (2017) Lifestyles and socio-cultural factors among children aged 6–8 years from five Italian towns: the MAPEC_LIFE study cohort. BMC Public Health 17:233. https://doi.org/10.1186/s12889-017-4142-x
Bonetta Sa, Bonetta Si, Schilirò T et al (2019) Mutagenic and genotoxic effects induced by PM0.5 of different Italian towns in human cells and bacteria: The MAPEC_LIFE study. Environ Pollut 245:1124–1135. https://doi.org/10.1016/j.envpol.2018.11.017
EU. Directive 2008/50/EC of the European Parliament and of the Council of 21 May 2008 on ambient air quality and cleaner air for Europe (OJ L 152, 11.6.2008, p. 1–44). 2008
ARPA Lombardia. Regional Agency for the Protection of the Environment of the Lombardy, Milan, Italy. http://www.arpalombardia.it/Pages/ARPA_Home_Page.aspx
ARPA Piemonte. Regional Agency for the Protection of the Environment of the Piedmont, Turin, Italy. http://www.arpa.piemonte.it
ARPA Puglia, Regional Agency for the Protection of the Environment of the Puglia, Bari Italy. http://www.arpa.puglia.it/web/guest/arpa_home
ARPA Toscana. Regional Agency for the Protection of the Environment of the Tuscany, Florence, Italy. http://www.arpat.toscana.it
ARPA Umbria. Regional Agency for the Protection of the Environment of the Umbria, Perugia, Italy. http://www.arpa.umbria.it
Sisenando HA, de Batistuzzo SR et al (2012) Micronucleus frequency in children exposed to biomass burning in the Brazilian Legal Amazon region: a control case study. BMC Oral Health 12:6. https://doi.org/10.1186/1472-6831-12-6
EU. Directive 2004/107/EC of the European Parliament and of the Council of 15 December 2004 relating to arsenic, cadmium, mercury, nickel and polycyclic aromatic hydrocarbons in ambient air (OJ L 23, 26.1.2005, pp. 3-16). 2004
WHO. Air quality guidelines for Europe. World Health Organization, Regional Office for Europe, Copenhagen. 2000
WHO. Air quality guidelines: global update 2005—particulate matter, ozone, nitrogen dioxide and sulphur dioxide. World Health Organization, Regional Office for Europe, Copenhagen. 2006
VanderWeele TJ, Shpitser I (2011) A new criterion for confounder selection. Biometrics 67:1406–1413. https://doi.org/10.1111/j.1541-0420.2011.01619.x
Lahiri T, Roy S, Basu C et al (2000) Air pollution in Calcutta elicits adverse pulmonary reaction in children. Indian J Med Res 112:21–26
Pedersen M, Vinzents P, Petersen JH et al (2006) Cytogenetic effects in children and mothers exposed to air pollution assessed by the frequency of micronuclei and fluorescence in situ hybridization (FISH): a family pilot study in the Czech Republic. Mutat Res 608:112–120. https://doi.org/10.1016/j.mrgentox.2006.02.013
Pedersen M, Wichmann J, Autrup H et al (2009) Increased micronuclei and bulky DNA adducts in cord blood after maternal exposures to traffic-related air pollution. Environ Res 109:1012–1020. https://doi.org/10.1016/j.envres.2009.08.011
Rossnerova A, Spatova M, Pastorkova A et al (2011) Micronuclei levels in mothers and their newborns from regions with different types of air pollution. Mutat Res 715:72–78. https://doi.org/10.1016/j.mrfmmm.2011.07.011
Fleck AS, Vieira M, Amantéa SL et al (2014) A comparison of the human buccal cell assay and the pollen abortion assay in assessing genotoxicity in an urban–rural gradient. Int J Environ Res Public Health 11:8825–8838. https://doi.org/10.3390/ijerph110908825
Coronas MV, Rocha JA, Salvadori DM et al (2016) Evaluation of area contaminated by wood treatment activities: genetic markers in the environment and in the child population. Chemosphere 144:1207–1215. https://doi.org/10.1016/j.chemosphere.2015.09.084
Ceretti E, Feretti D, Viola GCV et al (2014) DNA damage in buccal mucosa cells of pre-school children exposed to high levels of urban air pollutants. PLoS ONE 9:e96524. https://doi.org/10.1371/journal.pone.0096524
Huen K, Gunn L, Duramad P et al (2006) Application of a geographic information system to explore associations between air pollution and micronucleus frequencies in African American children and adults. Environ Mol Mutagen 47:236–246. https://doi.org/10.1002/em.20193
Idolo A, Grassi T, Bagordo F et al (2018) Micronuclei in exfoliated buccal cells of children living in a cluster area of Salento (Southern Italy) with a high incidence of lingu cancer: the IMP.AIR study. Int J Environ Res Public Health 15:1659. https://doi.org/10.3390/ijerph15081659
O’Callaghan-Gordo C, Fthenou E, Pedersen M et al (2015) Outdoor air pollution exposures and micronuclei frequencies in lymphocytes from pregnant women and newborns in Crete, Greece (Rhea cohort). Environ Res 143:170–176. https://doi.org/10.1016/j.envres.2015.10.011
Marcon A, Fracasso ME, Marchetti P et al (2014) Outdoor formaldehyde and NO2 exposures and markers of genotoxicity in children living near chipboard industries. Environ Health Perspect 122:639–645. https://doi.org/10.1289/ehp.1307259
Fenech M (2002) Chromosomal biomarkers of genomic instability relevant to cancer. Drug Discov Today 22:1128–1137. https://doi.org/10.1016/S1359-6446(02)02502-3
Murgia E, Maggini V, Barale R et al (2007) Micronuclei, genetic polymorphisms and cardiovascular disease mortality in a nested case–control study in Italy. Mutat Res 621:113–118. https://doi.org/10.1016/j.mrfmmm.2007.02.015
Migliore L, Coppedè F, Fenech M et al (2011) Association of micronucleus frequency with neurodegenerative diseases. Mutagenesis 26:85–92. https://doi.org/10.1093/mutage/geq067
Ceppi M, Biasotti B, Fenech M et al (2010) Human population studies with the exfoliated buccal micronucleus assay: statistical and epidemiological issues. Mutat Res 705:11–19. https://doi.org/10.1016/j.mrrev.2009.11.001
Bonassi S, Coskun E, Ceppi M et al (2011) The HUman MicroNucleus project on eXfoLiated buccal cells (HUMNXL): the role of life-style, host factors, occupational exposures, health status, and assay protocol. Mutat Res 728:88–97. https://doi.org/10.1016/j.mrrev.2011.06.005
Holland N, Bolognesi C, Kirsch-Volders M et al (2008) The micronucleus assay in human buccal cells as a tool for biomonitoring DNA damage: the HUMN project perspective on current status and knowledge gaps. Mutat Res 659:93–108. https://doi.org/10.1016/j.mrrev.2008.03.007
Thomas P, Holland N, Bolognesi C et al (2009) Buccal micronucleus cytome assay. Nat Protoc 4:825–837. https://doi.org/10.1038/nprot.2009.53
Raaschou-Nielsen O, Andersen ZJ, Beelen R et al (2013) Air pollution and lung cancer incidence in 17 European cohorts: prospective analyses from the European Study of Cohorts for Air Pollution Effects (ESCAPE). Lancet Oncol 14:813–822. https://doi.org/10.1016/S1470-2045(13)70279-1
WHO. Ambient air pollution: A global assessment of exposure and burden of disease. World Health Organization, Geneva, 2016
Eeftens M, Beelen R, de Hoogh K et al (2012) Development of land use regression models for PM2.5, PM2.5 absorbance, PM10 and PMcoarse in 20 European Study Areas; Results of the ESCAPE Project. Environ Sci Technol 46:11195–11205
Acknowledgements
The authors are grateful to the children and their parents for their participation in this study. The authors also wish to thank directors, teachers and janitors of the primary schools involved: Istituto Comprensivo “Est1” (schools “Raffaello” and “Giovanni XXIII”) and Istituto Comprensivo “Nord2” (schools “Arici” and “Quasimodo”) in Brescia; IV Circolo “Castromediano” (schools of Via Cantobelli and Via Valzani), V Circolo “Tempesta” (schools of Via da Taranto and Via Ofanto) and Istituto Paritario “Suore Discepole di Gesù Eucaristico” in Lecce; Istituto Comprensivo “Perugia2” (schools “Ciabatti” and “S. Erminio”) and 2° Circolo “Camparozzi” (schools “Don Milani”, “Villaggio Kennedy” and “Comparozzi”) in Perugia; Istituto Comprensivo “Tongiorgi” (schools “Collodi” and “Filzi”), Istituto Comprensivo “Galilei” (schools “De Sanctis” and “Gereschi”) and Istituto Comprensivo “Pisano” (school “Newbery”) in Pisa; Istituto Comprensivo “Tommaseo” (schools “Tommaseo” and “d’Assisi”), Istituto Comprensivo “Alpi” (schools “D’Acquisto”, “Deledda” and “Perotti”) and Circolo Didattico “Gobetti” (schools “Gobetti” and “Sclarandi”) in Torino. The MAPEC_LIFE Study Group: Andrea Festa1, Gaia Claudia Viviana Viola1, Ilaria Zerbini1, Cristina Fatigoni2, Sara Levorato2, Silvano Monarca2, Tania Salvatori2, Samuele Vannini2, Gabriele Donzelli3, Francesco Bagordo4, Mattia De Giorgi4, Marcello Guido4, Alessandra Panico4, Francesca Serio4, Maria Rosaria Tumolo4, Silvia Bonetta5, Marta Gea5, Giorgio Gilli5, Cristina Pignata5, Tiziana Schilirò5, Valeria Romanazzi5, Camilla Furia6, Beatrice Bruni7, Beatrice Casini7 (1Department of Medical and Surgical Specialties, Radiological Science and Public Health, University of Brescia, 11 Viale Europa, 25123 Brescia, Italy; 2Department of Pharmaceutical Sciences, Unit of Public Health, University of Perugia, Via del Giochetto, 06122 Perugia, Italy; 3Department of Biology, University of Pisa, 35/39 Via S. Zeno, 56127, Pisa, Italy; 4Department of Biological and Environmental Science and Technology, University of Salento, 165 Via Monteroni, 73100 Lecce, Italy; 5Department of Public Health and Pediatrics, University of Torino, 94 Piazza Polonia, 10126 Torino, Italy; 6Brescia Municipality, 1 Piazza Repubblica, 25100 Brescia, Italy; 7Department of Translational Research, N.T.M.S., University of Pisa, 35/39 Via S. Zeno, 56127, Pisa, Italy).
Funding
This project was supported by a grant from the European Commission Life + Programme 2012 (Grant ID: LIFE12 ENV/IT/000614 MAPEC_LIFE). The funder had no role in the design and conduct of the study; collection, analysis and interpretation of the data; preparation, review or approval of the manuscript; or decision to submit the manuscript for publication. The researchers were independent of the study funder.
Author information
Authors and Affiliations
Consortia
Contributions
All authors made substantial contributions to conception, design, implementation and management of the project (EC, FD, MM, ADD, ECa, DF, AC, AlB, SiB, UG), children’s recruitment (CZ, LC, MiV, MaV, TG, SaB), lab analysis performance (MiV, EC, MaV, GP, AI, SaB), data acquisition (CZ, DF, LC, MiV, GP, MM, TG, ECa), and data analysis and interpretation (EC, FD, AnB, UG). EC, FD and UG drafted the article and all other authors revised it critically for important intellectual content, approved the final draft, and agreed to be accountable for all aspects of the work. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The MAPEC_LIFE project has been approved by the local Ethics Committees of the Coordinating Unit (Brescia), first, and of the other towns involved in the study (Lecce, Perugia, Pisa, and Torino). Names of the Ethics Committees and dates of approval: Comitato Etico Provinciale della Provincia di Brescia, 15/1/2014 (approval n. NP1577); Comitato Etico of the ASL Lecce, 3/4/2014 (approval n. 9); Comitato Universitario di Bioetica of the University of Perugia, 9/5/2014; Comitato Etico Pediatrico Regionale of the Tuscany Region, 25/2/2014 (approval n. 29); Comitato di Bioetica d’Ateneo of the University of Torino, 27/3/2014.
Consent for publication
Not applicable.
Competing interests
The authors declare they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Additional file 1: Table S1.
Levels of air pollutants monitored by Regional Agencies for Environmental Protection in the 3 weeks preceding the biological samplings in winter and spring. Mean (± standard deviation, SD), minimum and maximum levels of exposure are reported. Table S2. Analysis of the associations between MN frequency and children’s features. Incidence Rate Ratio (IRR), 95% Confidence Intervals (95% CIs) and p value are reported. Table S3. Analysis of the associations between MN frequency and air pollutant levels. For each compound, the complete set of pollutant measures included in the model are specified. The Incidence Rate Ratio (IRR), 95% Confidence Intervals (95% CIs) and p value are reported. Table S4. Analysis of the associations between MN frequency and dichotomized air pollutant variables. Number of samples (N) and mean MN frequency ± SD (MN/1000) are reported for children exposed to levels lower (<) or higher (>) than the EU Ambient Air Quality Directive limits. The associations are expressed as IRR and 95%CIs. Table S5. Analysis of the associations between MN frequency and dichotomized air pollutant variables. Number of samples (N) and mean MN frequency ± SD (MN/1000) are reported for children exposed to levels lower (<) or higher (>) than the WHO Air Quality Guidelines (AQG). The associations are expressed as IRR and 95%CIs.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ceretti, E., Donato, F., Zani, C. et al. Results from the European Union MAPEC_LIFE cohort study on air pollution and chromosomal damage in children: are public health policies sufficiently protective?. Environ Sci Eur 32, 74 (2020). https://doi.org/10.1186/s12302-020-00352-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12302-020-00352-3