Article Text

Statistics from Altmetric.com
We read with great interest the article ‘Addressing immune-related adverse events of cancer immunotherapy: how prepared are rheumatologists?’ by Kostine et al.1 The introduction of immune checkpoint inhibitor (ICI) therapy has been a major breakthrough in the management of metastatic cancer. On the downside, ICI therapy may induce unwanted autoimmune effects, the so-called immune-related adverse effects (irAEs). Various irAEs have been described that resemble a regular rheumatic disease, including polymyalgia rheumatica (ICI-PMR).2 3 The authors report that rheumatologists may lack confidence in diagnosing irAEs. Therefore, recommendations for the diagnosis of rheumatic irAEs are needed. Based on our experience with ICI-PMR, we propose that imaging could be an important part of such recommendations.
We investigated six consecutive patients with ICI-PMR by ultrasonography, and five of these patients also by [18F]-fluorodeoxyglucose-positron emission tomography/computed tomography (FDG-PET/CT) scan. Five patients fulfilled the provisional American College of Rheumatology/European League Against Rheumatism classification criteria for PMR.4 A normal C-reactive protein level in the absence of an erythrocyte sedimentation rate (ESR) test precluded PMR classification in one patient. However, this patient fulfilled both the clinical and ultrasound criteria for PMR,4 and showed findings suggestive of PMR on the FDG-PET/CT scan.5 The median age was 73 years (range 59–83; online supplementary table 1). Patients received anti-programmed cell death protein 1 (PD-1) treatment, that is, nivolumab or pembrolizumab. ICI therapy resulted in near-complete cancer remission (n=3) or a partial response (n=3). Following the start of ICI therapy, the first symptoms suggestive of ICI-PMR developed after a median of 70 days (range 1–86).
Supplemental material
Ultrasonography of patients with ICI-PMR demonstrated findings consistent with PMR.6 Shoulder examination revealed biceps tenosynovitis in five patients and subacromial–subdeltoid bursitis in three patients (online supplementary table 1, online supplementary figure 1A). Glenohumeral synovitis was not detected. Hip ultrasound was performed in three patients, but revealed no coxofemoral synovitis or trochanteric bursitis. One patient received a glucocorticoid injection of the shoulder 14 weeks before ultrasonography, while another patients used a prednisolone equivalent of 7.5 mg/day for 5 weeks due to hypophysitis and adrenal insufficiency. The other patients received no glucocorticoids prior to ultrasonography.
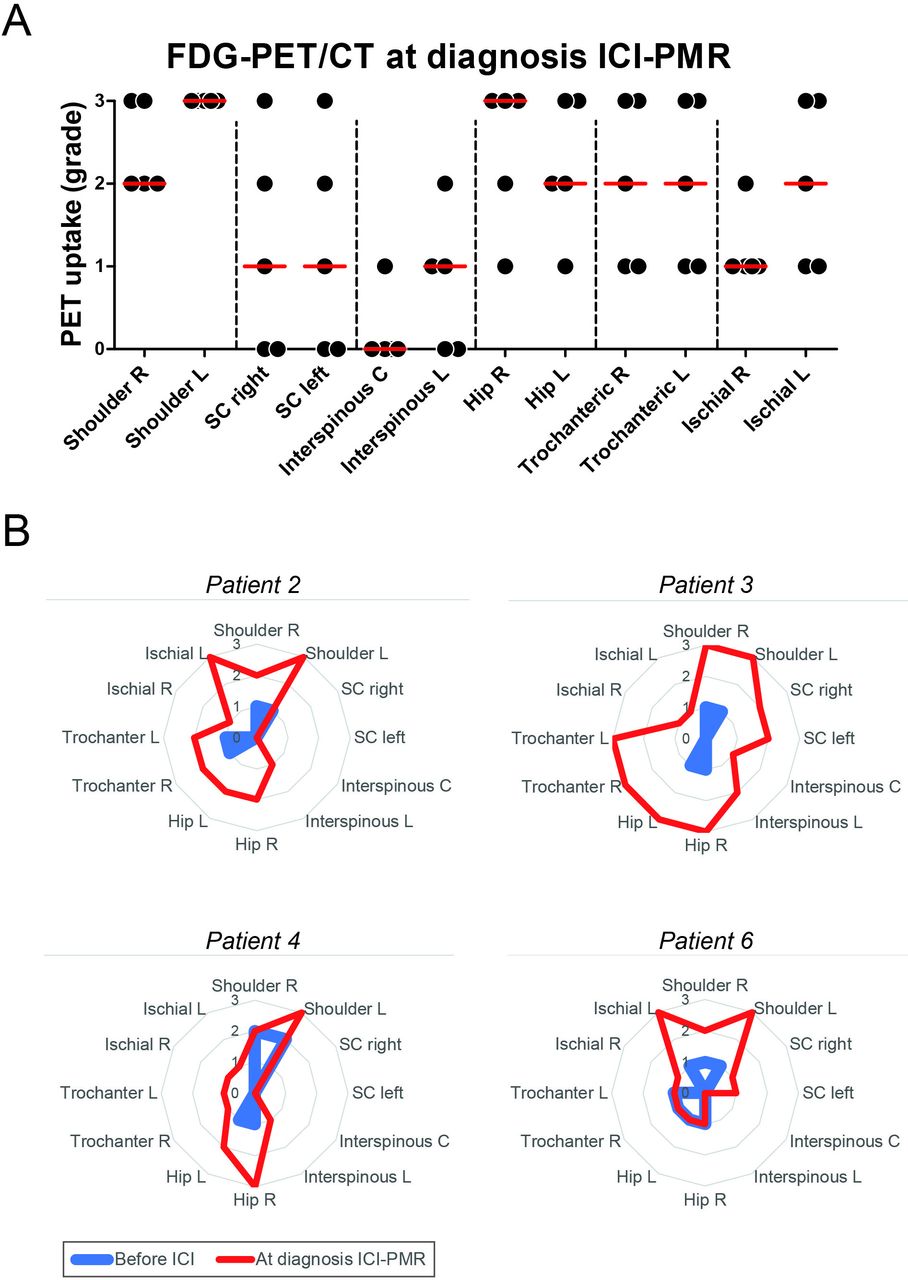
FDG-PET/CT scans of patients with regular PMR may demonstrate FDG uptake at the shoulders, hip joints, greater trochanters, ischial tuberosities, sternoclavicular joints and cervical/lumbar interspinous bursae.5 FDG-PET/CT scans of patients with ICI-PMR showed inflammation at these exact sites (online supplementary figure 1B). All FDG-PET/CT scans were obtained prior to initiation of any glucocorticoids. Scoring of FDG uptake was performed: 0, no uptake; 1, uptake lower than liver; 2 uptake equal to liver; 3, uptake higher than liver.7 All patients showed grade 2–3 uptake at the shoulders, and grade 1–3 uptake at the hip joints, greater trochanters and ischial tuberosities (figure 1A). FDG uptake at the sternoclavicular joints and cervical/lumbar interspinous bursa was present in part of the patients. In accordance with studies in regular PMR,5 part of the patients with ICI-PMR showed FDG uptake at the elbows (n=2) and hands/wrists (n=3; online supplementary figure 2). This was associated with mild synovitis of the hands/wrists on physical examination in one patient only. Recently, Calabrese et al also reported peripheral synovitis in patients with ICI-PMR.2 No evidence of giant cell arteritis was found in any of the patients.

{kind=link}
Grading of PET uptake at distinct sites in patients with immune checkpoint inhibitor-induced polymyalgia rheumatica (ICI-PMR). PET uptake was graded at the shoulders, sternoclavicular (SC) joints, cervical and lumbar interspinous bursae, hip joints, hip trochanters and ischial tuberosities (n=5). Grading was performed as previously described7: 0, no uptake; 1, uptake lower than liver; 2 uptake equal to liver; 3, uptake higher than liver. (A) PET uptake in five patients (ie, patient 1–4, and patient 6) at diagnosis of ICI-PMR. (B) PET uptake in four patients at diagnosis of ICI-PMR and prior to ICI therapy and onset of ICI-PMR.
Four patients underwent a FDG-PET/CT scan prior to ICI therapy. These scans showed grade 1–2 FDG uptake at the shoulders and hips (figure 1B). Although this mild metabolic activity may also be seen in non-inflammatory conditions, it could suggests that low-grade, subclinical inflammation was already present at these sites before ICI therapy. The checkpoint molecule PD-1 might have initially prevented the development of full-blown inflammation in these patients.
In conclusion, FDG-PET/CT and ultrasound findings in ICI-PMR are comparable to those seen in regular PMR.5 6 Imaging may thus help to confidently diagnose ICI-PMR. Low-grade FDG uptake was already observed on the FDG-PET/CT scan prior to ICI therapy, and progressed towards the full-blown PMR pattern after initiation of ICI therapy. It remains to be elucidated whether or not baseline imaging before ICI therapy may help to predict the development of rheumatic irAEs.
Ethics statements
Patient consent for publication
Ethics approval
The study was performed in accordance with the declaration of Helsinki. The study was approved by the Medical Ethical Committee of the UMCG, and all patients provided written informed consent.
Footnotes
Contributors KSMvdG, RHJAS and EB contributed to conception or design of the work. KSMvdG and RHJAS contributed to acquisition of data. All authors contributed to analysis or interpretation of data. All authors were involved in drafting of the work or revising it critically for important intellectual content. All authors provided final approval of the version published. All authors agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding The work of KSMvdG was supported by the Mandema Stipend. EB has received funding from the European Union’s Horizon 2020 research and innovation programme under grant agreement 668036.
Competing interests KSMvdG and EB as employees of the UMCG received speaker/consulting fees from Roche that were paid to the UMCG. TJNH as employee of the UMCG received sponsoring/research fee/advisory board fee/other income from BMS, AZD, Merck, Boehringer, Pfizer, Eli Lilly, Roche, Platform immunotherapy and CANCER-ID. SFO received research grants from Novartis and Celldex, paid to the institution. The other authors have nothing to declare.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; internally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.