
Abstract
Background
There is no consensus as to when surgical intervention should be considered for recurrent ileocolic intussusceptions in a stable patient after previous successful air contrast enema.
Objective
To review the patterns of ileocolic intussusceptions, air contrast enema success rates, and pathologic lead point rates in patients with and without recurrence to evaluate whether treatment outcomes depend on the number and timing between episodes.
Materials and methods
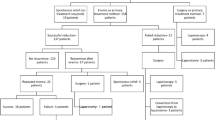
We retrospectively reviewed 683 children with air contrast enema performed for ileocolic intussusception between January 2000 and May 2018. Recurrent intussusceptions were separated into mutually exclusive categories: short-term only (≤7 days between episodes) and long-term (>7 days between episodes) intussusceptions. Long-term recurrences included both long-term only and long- and short-term intussusceptions.
Results
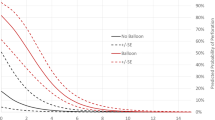
Of the 683 patients, 606 (89%) had at least 1 successful air contrast enema. Of the 606, 115 (19%) had recurrent intussusceptions after successful reduction. The air contrast enema success rate for a single intussusception was 86% (491/568) and for recurrent intussusceptions was 96% (110/115) (P=0.004). Single and recurrent intussusceptions had similar pathologic lead point rates (3.5% vs. 4.3%; P=0.593). Short-term and long-term recurrences did not differ in air contrast enema success rates (96% vs. 95%). Long-term recurrences had higher pathologic lead point rate compared to short-term only (13% vs. 0%; P=0.003). Of short-term recurrences, 99% (76/77) were ≤5 intussusceptions; 92% had successful air contrast enema without surgery.
Conclusion
The majority of recurrent intussusceptions were successfully treated by air contrast enema. Short-term recurrences have lower pathologic lead point rates, suggesting that a higher surgical threshold may be plausible relative to long-term recurrences. In the appropriate clinical context, repeat air contrast enemas are a safe option for short-term recurrences, which can be attempted at least five times, potentially precluding the need for surgical intervention.



Similar content being viewed by others

References
Buettcher M, Baer G, Bonhoeffer J et al (2007) Three-year surveillance of intussusception in children in Switzerland. Pediatrics 120:473–480
del-Pozo G, Albillos JC, Tejedor D et al (1999) Intussusception in children: current concepts in diagnosis and enema reduction. Radiographics 19:299–319
Daneman A, Alton DJ, Lobo E et al (1998) Patterns of recurrence of intussusception in children: a 17-year review. Pediatr Radiol 28:913–919
Lessenich EM, Kimia AA, Mandeville K et al (2015) The frequency of postreduction interventions after successful enema reduction of intussusception. Acad Emerg Med 22:1042–1047
Cohen MD (2002) From air to barium and back to air reduction of intussusception in children. Pediatr Radiol 32:74
Beres AL, Baird R (2013) An institutional analysis and systematic review with meta-analysis of pneumatic versus hydrostatic reduction for pediatric intussusception. Surgery 154:328–334
Kaplan SL, Magill D, Felice MA et al (2017) Intussusception reduction: effect of air vs. liquid enema on radiation dose. Pediatr Radiol 47:1471–1476
Hadidi AT, El Shal N (1999) Childhood intussusception: a comparative study of nonsurgical management. J Pediatr Surg 34:304–307
Hsu WL, Lee HC, Yeung CY et al (2012) Recurrent intussusception: when should surgical intervention be performed? Pediatr Neonatol 53:300–303
Gray MP, Li SH, Hoffmann RG, Gorelick MH (2014) Recurrence rates after intussusception enema reduction: a meta-analysis. Pediatrics 134:110–119
Champoux AN, Del Beccaro MA, Nazar-Stewart V (1994) Recurrent intussusception. Risks and features. Arch Pediatr Adolesc Med 148:474–478
Benson CD, Lloyd JR, Fischer H (1963) Intussusception in infants and children. An analysis of 300 cases. Arch Surg 86:745–751
Sadigh G, Zou KH, Razavi SA et al (2015) Meta-analysis of air versus liquid enema for intussusception reduction in children. AJR Am J Roentgenol 205:W542–W549
Schuh S, Wesson DE (1987) Intussusception in children 2 years of age or older. CMAJ 136:269–272
Niramis R, Watanatittan S, Kruatrachue A et al (2010) Management of recurrent intussusception: nonoperative or operative reduction? J Pediatr Surg 45:2175–2180
Ong NT, Beasley SW (1990) The leadpoint in intussusception. J Pediatr Surg 25:640–643
Guo WL, Hu ZC, Tan YL et al (2017) Risk factors for recurrent intussusception in children: a retrospective cohort study. BMJ Open 7:e018604
Kim JH, Lee JS, Ryu JM et al (2018) Risk factors for recurrent intussusception after fluoroscopy-guided air enema. Pediatr Emerg Care 34:484–487
Miller SF, Landes AB, Dautenhahn LW et al (1995) Intussusception: ability of fluoroscopic images obtained during air enemas to depict lead points and other abnormalities. Radiology 197:493–496
Binkovitz LA, Kolbe AB, Orth RC et al (2019) Pediatric ileocolic intussusception: new observations and unexpected implications. Pediatr Radiol 49:76–81
Khong PL, Peh WC, Lam CH et al (2000) Ultrasound-guided hydrostatic reduction of childhood intussusception: technique and demonstration. Radiographics 20:E1
Digant SM, Rucha S, Eke D (2012) Ultrasound guided reduction of an ileocolic intussusception by a hydrostatic method by using normal saline enema in paediatric patients: a study of 30 cases. J Clin Diagn Res 6:1722–1725
Mensah Y, Glover-Addy H, Etwire V et al (2011) Ultrasound guided hydrostatic reduction of intussusception in children at Korle Bu teaching hospital: an initial experience. Ghana Med J 45:128–131
Khanna G, Applegate K (2008) Ultrasound guided intussusception reduction: are we there yet? Abdom Imaging 33:38–40
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Ma, G.M.Y., Lillehei, C. & Callahan, M.J. Air contrast enema reduction of single and recurrent ileocolic intussusceptions in children: patterns, management and outcomes. Pediatr Radiol 50, 664–672 (2020). https://doi.org/10.1007/s00247-020-04612-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00247-020-04612-5