
Abstract
People living with HIV (PLWH) in the antiretroviral therapy (ART) era may lose more life-years to tobacco use than to HIV. Yet, smoking rates are more than twice as high among PLWH than the general population, contributing not just to mortality but to other adverse health outcomes, including neurocognitive deficits (neuroHIV). There is growing evidence that synergy with chronic inflammation and immune dysregulation that persists despite ART may be one mechanism by which tobacco smoking contributes to neuroHIV. This review will summarize the differential effects of nicotine vs tobacco smoking on inflammation in addition to the effects of tobacco smoke components on HIV disease progression. We will also discuss biomarkers of inflammation via neuroimaging as well as biomarkers of nicotine dependence (e.g., nicotine metabolite ratio). Tobacco smoking and nicotine may impact ART drug metabolism and conversely, certain ARTs may impact nicotine metabolism. Thus, we will review these bidirectional relationships and how they may contribute to neuroHIV and other adverse outcomes. We will also discuss the effects of tobacco use on the interaction between peripheral organs (lungs, heart, kidney) and subsequent CNS function in the context of HIV. Lastly, given the dramatic rise in the use of electronic nicotine delivery systems, we will discuss the implications of vaping on these processes. Despite the growing recognition of the importance of addressing tobacco use among PLWH, more research is necessary at both the preclinical and clinical level to disentangle the potentially synergistic effects of tobacco use, nicotine, HIV, cognition and immune dysregulation, as well as identify optimal approaches to reduce tobacco use.

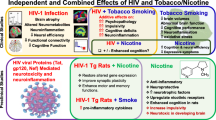
Proposed model of the relationships among HIV, ART, smoking, inflammation, and neurocognition. Solid lines represent relationships supported by evidence. Dashed lines represent relationships for which there is not enough evidence to make a conclusion. (a) HIV infection produces elevated levels of inflammation even among virally suppressed individuals. (b) HIV is associated with deficits in cognition function. (c) Smoking rates are higher among PLWH, compared to the general population. (d) The nicotine metabolite ratio (NMR) is associated with smoking behavior. (e) HIV and tobacco use are both associated with higher rates of psychiatric comorbidities, such as depression, and elevated levels of chronic stress. These factors may represent other mechanisms linking HIV and tobacco use. (f) The relationship between nicotine, tobacco smoking, and inflammation is complex, but it is well-established that smoking induces inflammation; the evidence for nicotine as anti-inflammatory is supported in some studies, but not others. (g) The relationship between tobacco use and neurocognition may differ for the effects of nicotine (acute nicotine use may have beneficial effects) vs. tobacco smoking (chronic use may impair cognition). (h) Elevated levels of inflammation may be associated with deficits in cognition. (i) PLWH may metabolize nicotine faster than those without HIV; the mechanism is not yet known and the finding needs validation in larger samples. We also hypothesize that if HIV-infection increases nicotine metabolism, then we should observe an attenuation effect once ART is initiated. (j) It is possible that the increase in NMR is due to ART effects on CYP2A6. (k) We hypothesize that faster nicotine metabolism may result in higher levels of inflammation since nicotine has anti-inflammatory properties.



Similar content being viewed by others


References
Abbud RA, Finegan CK, Guay LA, Rich EA (1995) Enhanced production of human immunodeficiency virus type 1 by in vitro-infected alveolar macrophages from otherwise healthy cigarette smokers. J Infect Dis 172:859–863
Abers MS, Shandera WX, Kass JS (2014) Neurological and psychiatric adverse effects of antiretroviral drugs. CNS Drugs 28:131–145. https://doi.org/10.1007/s40263-013-0132-4
Aguiar JA et al (2019) The impact of cigarette smoke exposure, COPD, or asthma status on ABC transporter gene expression in human airway epithelial cells. Sci Rep 9:153. https://doi.org/10.1038/s41598-018-36248-9
Akhtar-Khaleel WZ et al (2017) Association of midlife smoking status with change in processing speed and mental flexibility among HIV-seropositive and HIV-seronegative older men: the Multicenter AIDS Cohort Study. J Neurovirol 23:239–249. https://doi.org/10.1007/s13365-016-0496-6
Alderton WK, Cooper CE, Knowles RG (2001) Nitric oxide synthases: structure, function and inhibition. Biochem J 357:593–615
Allais L et al (2016) Chronic cigarette smoke exposure induces microbial and inflammatory shifts and mucin changes in the murine gut. Environ Microbiol 18:1352–1363. https://doi.org/10.1111/1462-2920.12934
Allenby CE, Boylan KA, Lerman C, Falcone M (2016) Precision Medicine for Tobacco Dependence: Development and Validation of the Nicotine Metabolite Ratio. J Neuroimmune Pharmacol 11:471–483. https://doi.org/10.1007/s11481-016-9656-y
Almodovar S (2014) The complexity of HIV persistence and pathogenesis in the lung under antiretroviral therapy: challenges beyond AIDS. Viral Immunol 27:186–199. https://doi.org/10.1089/vim.2013.0130
Altekruse SF et al (2018) Cancer burden attributable to cigarette smoking among HIV-infected people in North America. AIDS 32:513–521. https://doi.org/10.1097/QAD.0000000000001721
Ambrose JA, Barua RS (2004) The pathophysiology of cigarette smoking and cardiovascular disease: an update. J Am Coll Cardiol 43:1731–1737. https://doi.org/10.1016/j.jacc.2003.12.047
An Y et al (2012) Cigarette smoke promotes drug resistance and expansion of cancer stem cell-like side population. PLoS One 7:e47919. https://doi.org/10.1371/journal.pone.0047919
Ande A, McArthur C, Kumar A, Kumar S (2013) Tobacco smoking effect on HIV-1 pathogenesis: role of cytochrome P450 isozymes. Expert Opin Drug Metab Toxicol 9:1453–1464. https://doi.org/10.1517/17425255.2013.816285
Ande A et al (2015) Effect of mild-to-moderate smoking on viral load, cytokines, oxidative stress, and cytochrome P450 enzymes in HIV-infected individuals. PLoS One 10:e0122402. https://doi.org/10.1371/journal.pone.0122402
Antinori A et al (2007) Updated research nosology for HIV-associated neurocognitive disorders. Neurology 69:1789–1799. https://doi.org/10.1212/01.WNL.0000287431.88658.8b
Antiretroviral Therapy Cohort C (2008) Life expectancy of individuals on combination antiretroviral therapy in high-income countries: a collaborative analysis of 14 cohort studies. Lancet (London, England) 372:293–299. https://doi.org/10.1016/S0140-6736(08)61113-7
Anzenbacher P, Anzenbacherova E (2001) Cytochromes P450 and metabolism of xenobiotics. Cell Mol Life Sci 58:737–747
Arany I, Hall S, Reed DK, Reed CT, Dixit M (2016) Nicotine Enhances High-Fat Diet-Induced Oxidative Stress in the Kidney. Nicotine Tob Res 18:1628–1634. https://doi.org/10.1093/ntr/ntw029
Armstrong DA et al (2019) DNA Methylation Changes in Regional Lung Macrophages Are Associated with Metabolic Differences. ImmunoHorizons 3:274–281. https://doi.org/10.4049/immunohorizons.1900042
Arnson Y, Shoenfeld Y, Amital H (2010) Effects of tobacco smoke on immunity, inflammation and autoimmunity. J Autoimmun:34, J258–J265. https://doi.org/10.1016/j.jaut.2009.12.003
Ashare RL, Wetherill RR (2018) The Intersection of Sex Differences, Tobacco Use, and Inflammation: Implications for Psychiatric Disorders. Curr Psychiatry Rep 20:75. https://doi.org/10.1007/s11920-018-0946-3
Ashare RL, Falcone M, Lerman C (2014) Cognitive function during nicotine withdrawal: Implications for nicotine dependence treatment. Neuropharmacology 76(Pt B):581–591. https://doi.org/10.1016/j.neuropharm.2013.04.034
Ashare RL et al (2019a) Differences in the rate of nicotine metabolism among smokers with and without HIV. AIDS 33:1083–1088. https://doi.org/10.1097/qad.0000000000002127
Ashare RL et al (2019b) Placebo-controlled randomized clinical trial testing the efficacy and safety of varenicline for smokers with HIV. Drug Alcohol Depend 200:26–33. https://doi.org/10.1016/j.drugalcdep.2019.03.011
Asthana A, Johnson HM, Piper ME, Fiore MC, Baker TB, Stein JH (2010) Effects of smoking intensity and cessation on inflammatory markers in a large cohort of active smokers. Am Heart J 160:458–463. https://doi.org/10.1016/j.ahj.2010.06.006
Badrick E, Kirschbaum C, Kumari M (2007) The relationship between smoking status and cortisol secretion. J Clin Endocrinol Metab 92:819–824. https://doi.org/10.1210/jc.2006-2155
Baez-Pagan CA, Delgado-Velez M, Lasalde-Dominicci JA (2015) Activation of the Macrophage alpha7 Nicotinic Acetylcholine Receptor and Control of Inflammation. J Neuroimmune Pharmacol 10:468–476. https://doi.org/10.1007/s11481-015-9601-5
Baldassarri SR et al (2018) Use of Electronic Cigarettes Leads to Significant Beta2-Nicotinic Acetylcholine Receptor Occupancy: Evidence From a PET Imaging Study Nicotine. Tob Res 20:425–433. https://doi.org/10.1093/ntr/ntx091
Ballester LY et al (2012) Up-regulation of the neuronal nicotinic receptor alpha7 by HIV glycoprotein 120: potential implications for HIV-associated neurocognitive disorder. J Biol Chem 287:3079–3086. https://doi.org/10.1074/jbc.M111.262543
Bell SK, Mena G, Dean J, Boyd M, Gilks C, Gartner C (2017) Vaporised nicotine and tobacco harm reduction for addressing smoking among people living with HIV: A cross-sectional survey of Australian HIV health practitioners’ attitudes. Drug Alcohol Depend 177:67–70. https://doi.org/10.1016/j.drugalcdep.2017.03.023
Benowitz NL (2009) Pharmacology of nicotine: addiction, smoking-induced disease, and therapeutics. Annu Rev Pharmacol Toxicol 49:57–71. https://doi.org/10.1146/annurev.pharmtox.48.113006.094742
Benowitz NL, Jacob P 3rd (2001) Trans-3’-hydroxycotinine: disposition kinetics, effects and plasma levels during cigarette smoking. Br J Clin Pharmacol 51:53–59
Benowitz NL, Pomerleau OF, Pomerleau CS, Jacob P 3rd (2003) Nicotine metabolite ratio as a predictor of cigarette consumption Nicotine. Tob Res 5:621–624
Benowitz NL, Hukkanen J, Jacob P, 3rd (2009) Nicotine chemistry, metabolism, kinetics and biomarkers Handbook of experimental pharmacology:29-60 https://doi.org/10.1007/978-3-540-69248-5_2
Berno G et al (2014) Analysis of single-nucleotide polymorphisms (SNPs) in human CYP3A4 and CYP3A5 genes: potential implications for the metabolism of HIV drugs. BMC Med Genet:15–76. https://doi.org/10.1186/1471-2350-15-76
Biondi-Zoccai G et al (2019) Acute Effects of Heat-Not-Burn, Electronic Vaping, and Traditional Tobacco Combustion Cigarettes: The Sapienza University of Rome-Vascular Assessment of Proatherosclerotic Effects of Smoking ( SUR - VAPES ) 2 Randomized Trial. J Am Heart Assoc 8:e010455. https://doi.org/10.1161/jaha.118.010455
Boelaert JR, Piette J, Weinberg GA, Sappey C, Weinberg ED (1996) Iron and oxidative stress as a mechanism for the enhanced production of human immunodeficiency virus by alveolar macrophages from otherwise healthy cigarette smokers. J Infect Dis 173:1045–1047. https://doi.org/10.1093/infdis/173.4.1045a
Borsook D, Becerra L, Hargreaves R (2006) A role for fMRI in optimizing CNS drug development. Nat Rev Drug Discov 5:411–424. https://doi.org/10.1038/nrd2027
Bracci L, Lozzi L, Rustici M, Neri P (1992) Binding of HIV-1 gp120 to the nicotinic receptor. FEBS Lett 311:115–118
Brody AL et al (2006) Cigarette smoking saturates brain alpha 4 beta 2 nicotinic acetylcholine receptors. Arch Gen Psychiatry 63:907–915. https://doi.org/10.1001/archpsyc.63.8.907
Brody AL et al (2009) Brain nicotinic acetylcholine receptor occupancy: effect of smoking a denicotinized cigarette. Int J Neuropsychopharmacol 12:305–316. https://doi.org/10.1017/S146114570800922X
Brody AL et al (2011) Effect of secondhand smoke on occupancy of nicotinic acetylcholine receptors in brain. Arch Gen Psychiatry 68:953–960. https://doi.org/10.1001/archgenpsychiatry.2011.51
Brody AL et al (2013) Treatment for tobacco dependence: effect on brain nicotinic acetylcholine receptor density. Neuropsychopharmacology 38:1548–1556. https://doi.org/10.1038/npp.2013.53
Brody AL et al (2014) Brain nicotinic acetylcholine receptor availability and response to smoking cessation treatment: a randomized trial. JAMA Psychiatry 71:797–805. https://doi.org/10.1001/jamapsychiatry.2014.138
Brody AL et al (2017) Effect of Cigarette Smoking on a Marker for Neuroinflammation: A [(11)C]DAA1106 Positron Emission Tomography Study. Neuropsychopharmacology 42:1630–1639. https://doi.org/10.1038/npp.2017.48
Brody AL et al (2018) Effect of overnight smoking abstinence on a marker for microglial activation: a [(11)C]DAA1106 positron emission tomography study. Psychopharmacology (Berl) 235:3525–3534. https://doi.org/10.1007/s00213-018-5077-3
Brown AK et al (2007) Radiation dosimetry and biodistribution in monkey and man of 11C-PBR28: a PET radioligand to image inflammation. J Nucl Med 48:2072–2079. https://doi.org/10.2967/jnumed.107.044842
Bryant VE, Kahler CW, Devlin KN, Monti PM, Cohen RA (2013) The effects of cigarette smoking on learning and memory performance among people living with HIV/AIDS. AIDS Care 25:1308–1316. https://doi.org/10.1080/09540121.2013.764965
Butler SL et al (2011) Disease-modifying therapeutic concepts for HIV in the era of highly active antiretroviral therapy. J Acquir Immune Defic Syndr 58:297–303. https://doi.org/10.1097/QAI.0b013e31822ccfcc
Capo-Velez CM, Delgado-Velez M, Baez-Pagan CA, Lasalde-Dominicci JA (2018a) Nicotinic Acetylcholine Receptors in HIV: Possible Roles During HAND and Inflammation. Cell Mol Neurobiol 38:1335–1348. https://doi.org/10.1007/s10571-018-0603-8
Capo-Velez CM et al (2018b) The alpha7-nicotinic receptor contributes to gp120-induced neurotoxicity: implications in HIV-associated neurocognitive disorders. Sci Rep 8:1829. https://doi.org/10.1038/s41598-018-20271-x
Capurso G, Lahner E (2017) The interaction between smoking, alcohol and the gut microbiome. Best Pract Res Clin Gastroenterol 31:579–588. https://doi.org/10.1016/j.bpg.2017.10.006
Cavalcante GIT et al (2017) HIV antiretroviral drug Efavirenz induces anxiety-like and depression-like behavior in rats: evaluation of neurotransmitter alterations in the striatum. Eur J Pharmacol 799:7–15. https://doi.org/10.1016/j.ejphar.2017.02.009
CDC (2017) HIV surveillance reports, vol 29. Centers for Disease Control and Prevention, Atlanta
Chand HS et al (2018) Cigarette smoke and HIV synergistically affect lung pathology in cynomolgus macaques. J Clin Invest 128:5428–5433. https://doi.org/10.1172/JCI121935
Chang L, Lim A, Lau E, Alicata D (2017) Chronic Tobacco-Smoking on Psychopathological Symptoms, Impulsivity and Cognitive Deficits in HIV-Infected Individuals. J Neuroimmune Pharmacol 12:389–401. https://doi.org/10.1007/s11481-017-9728-7
Chatterjee S, Tao JQ, Johncola A, Guo W, Caporale A, Langham MC, Wehrli FW (2019) Acute exposure to e-cigarettes causes inflammation and pulmonary endothelial oxidative stress in nonsmoking, healthy young subjects. Am J Physiol Lung Cell Mol Physiol 317:L155–L166. https://doi.org/10.1152/ajplung.00110.2019
Chaumont M et al (2018) Differential Effects of E-Cigarette on Microvascular Endothelial Function, Arterial Stiffness and Oxidative Stress: A Randomized Crossover Trial. Sci Rep 8:10378. https://doi.org/10.1038/s41598-018-28723-0
Chauveau F, Boutin H, Van Camp N, Dolle F, Tavitian B (2008) Nuclear imaging of neuroinflammation: a comprehensive review of [11C]PK11195 challengers. Eur J Nucl Med Mol Imaging 35:2304–2319. https://doi.org/10.1007/s00259-008-0908-9
Chenoweth MJ, O'Loughlin J, Sylvestre MP, Tyndale RF (2013) CYP2A6 slow nicotine metabolism is associated with increased quitting by adolescent smokers. Pharmacogenet Genomics 23:232–235. https://doi.org/10.1097/FPC.0b013e32835f834d
Chenoweth MJ et al (2014) Known and novel sources of variability in the nicotine metabolite ratio in a large sample of treatment-seeking smokers. Cancer Epidemiol Biomarkers Prev 23:1773–1782. https://doi.org/10.1158/1055-9965.EPI-14-0427
Chinnapaiyan S, Dutta R, Bala J, Parira T, Agudelo M, Nair M, Unwalla HJ (2018) Cigarette smoke promotes HIV infection of primary bronchial epithelium and additively suppresses CFTR function. Sci Rep 8:7984. https://doi.org/10.1038/s41598-018-26095-z
Cioe PA, Gordon REF, Guthrie KM, Freiberg MS, Kahler CW (2018) Perceived barriers to smoking cessation and perceptions of electronic cigarettes among persons living with HIV. AIDS Care 30:1469–1475. https://doi.org/10.1080/09540121.2018.1489103
Cole MP, Freeman BA (2009) Promotion of cardiovascular disease by exposure to the air pollutant ozone. Am J Physiol Lung Cell Mol Physiol 297:L205–L208. https://doi.org/10.1152/ajplung.00187.2009
Cosgrove KP et al (2009) beta2-Nicotinic acetylcholine receptor availability during acute and prolonged abstinence from tobacco smoking Arch Gen Psychiatry 66:666-676. https://doi.org/10.1001/archgenpsychiatry.2009.41
Cosgrove KP et al (2012) Sex differences in availability of beta2*-nicotinic acetylcholine receptors in recently abstinent tobacco smokers. Arch Gen Psychiatry 69:418–427. https://doi.org/10.1001/archgenpsychiatry.2011.1465
Coughlin JM et al (2014) Regional brain distribution of translocator protein using [(11)C]DPA-713 PET in individuals infected with HIV. J Neurovirol 20:219–232. https://doi.org/10.1007/s13365-014-0239-5
Coughlin JM et al (2018) (18)F-XTRA PET for Enhanced Imaging of the Extrathalamic alpha4beta2 Nicotinic Acetylcholine Receptor. J Nucl Med 59:1603–1608. https://doi.org/10.2967/jnumed.117.205492
Cui WY, Li MD (2010) Nicotinic modulation of innate immune pathways via alpha7 nicotinic acetylcholine receptor. J Neuroimmune Pharmacology 5:479–488. https://doi.org/10.1007/s11481-010-9210-2
Culhane MA et al (2008) Predictors of early abstinence in smokers with schizophrenia. J Clin Psychiatry 69:1743–1750
D’Arcy PF (1984) Tobacco smoking and drugs: a clinically important interaction? Drug Intell Clin Pharm 18:302–307. https://doi.org/10.1177/106002808401800405
De Simone R, Ajmone-Cat MA, Carnevale D, Minghetti L (2005) Activation of alpha7 nicotinic acetylcholine receptor by nicotine selectively up-regulates cyclooxygenase-2 and prostaglandin E2 in rat microglial cultures. J Neuroinflammation 2:4. https://doi.org/10.1186/1742-2094-2-4
de Vries M et al (2018) From blood to lung tissue: effect of cigarette smoke on DNA methylation and lung function. Resp Res 19:212. https://doi.org/10.1186/s12931-018-0904-y
Delgado-Velez M et al (2015) The alpha7-nicotinic receptor is upregulated in immune cells from HIV-seropositive women: consequences to the cholinergic anti-inflammatory response. Clin Transl Immunology 4:e53. https://doi.org/10.1038/cti.2015.31
Deuther-Conrad W et al (2008) Norchloro-fluoro-homoepibatidine (NCFHEB) - a promising radioligand for neuroimaging nicotinic acetylcholine receptors with PET. Eur Neuropsychopharmacol 18:222–229. https://doi.org/10.1016/j.euroneuro.2007.07.002
Do AN et al (2014) Excess burden of depression among HIV-infected persons receiving medical care in the united states: data from the medical monitoring project and the behavioral risk factor surveillance system. PLoS One 9:e92842. https://doi.org/10.1371/journal.pone.0092842
Doorduin J, de Vries EF, Willemsen AT, de Groot JC, Dierckx RA, Klein HC (2009) Neuroinflammation in schizophrenia-related psychosis: a PET study. J Nucl Med 50:1801–1807. https://doi.org/10.2967/jnumed.109.066647
Doyle KL et al (2013) Real-world impact of neurocognitive deficits in acute and early HIV infection. J Neurovirol 19:565–573. https://doi.org/10.1007/s13365-013-0218-2
Durazzo TC, Rothlind JC, Cardenas VA, Studholme C, Weiner MW, Meyerhoff DJ (2007) Chronic cigarette smoking and heavy drinking in human immunodeficiency virus: consequences for neurocognition and brain morphology. Alcohol 41:489–501. https://doi.org/10.1016/j.alcohol.2007.07.007
Durazzo TC, Meyerhoff DJ, Nixon SJ (2012) A comprehensive assessment of neurocognition in middle-aged chronic cigarette smokers. Drug Alcohol Depend 122:105–111. https://doi.org/10.1016/j.drugalcdep.2011.09.019
Earla R, Ande A, McArthur C, Kumar A, Kumar S (2014) Enhanced nicotine metabolism in HIV-1-positive smokers compared with HIV-negative smokers: simultaneous determination of nicotine and its four metabolites in their plasma using a simple and sensitive electrospray ionization liquid chromatography-tandem mass spectrometry technique. Drug Metab Dispos 42:282–293. https://doi.org/10.1124/dmd.113.055186
Ekins S, Mathews P, Saito EK, Diaz N, Naylor D, Chung J, McMurtray AM (2017) alpha7-Nicotinic acetylcholine receptor inhibition by indinavir: implications for cognitive dysfunction in treated HIV disease. AIDS 31:1083–1089. https://doi.org/10.1097/QAD.0000000000001488
Eltorai AE, Choi AR, Eltorai AS (2019) Impact of Electronic Cigarettes on Various Organ Systems. Respir Care 64:328–336. https://doi.org/10.4187/respcare.06300
Endres CJ, Coughlin JM, Gage KL, Watkins CC, Kassiou M, Pomper MG (2012) Radiation dosimetry and biodistribution of the TSPO ligand 11C-DPA-713 in humans. J Nucl Med 53:330–335. https://doi.org/10.2967/jnumed.111.094565
Esplugues JV (2002) NO as a signalling molecule in the nervous system. Br J Pharmacol 135:1079–1095. https://doi.org/10.1038/sj.bjp.0704569
Feldman C, Anderson R (2013) Cigarette smoking and mechanisms of susceptibility to infections of the respiratory tract and other organ systems. J Infect 67:169–184. https://doi.org/10.1016/j.jinf.2013.05.004
Feldman JG et al (2006) Association of cigarette smoking with HIV prognosis among women in the HAART era: a report from the women's interagency HIV study Am J Public Health 96:1060-1065. https://doi.org/10.2105/ajph.2005.062745
Feldman DN et al (2009) CYP1A1 genotype modifies the impact of smoking on effectiveness of HAART among women AIDS education and prevention : official publication of the International Society for AIDS. Education 21:81–93. https://doi.org/10.1521/aeap.2009.21.3_supp.81
Forman-Hoffman VL, Hedden SL, Glasheen C, Davies C, Colpe LJ (2016) The role of mental illness on cigarette dependence and successful quitting in a nationally representative, household-based sample of U.S. adults. Ann Epidemiol 26:447–454. https://doi.org/10.1016/j.annepidem.2016.05.004
Frazier EL, Sutton MY, Brooks JT, Shouse RL, Weiser J (2018) Trends in cigarette smoking among adults with HIV compared with the general adult population, United States - 2009-2014. Prev Med 111:231–234. https://doi.org/10.1016/j.ypmed.2018.03.007
Fries M et al (2005) S-100 protein and neurohistopathologic changes in a porcine model of acute lung injury. Anesthesiology 102:761–767. https://doi.org/10.1097/00000542-200504000-00011
Friis-Moller N et al (2003) Combination antiretroviral therapy and the risk of myocardial infarction. N Engl J Med 349:1993–2003. https://doi.org/10.1056/NEJMoa030218
Gallezot JD et al (2005) In vivo imaging of human cerebral nicotinic acetylcholine receptors with 2-18F-fluoro-A-85380 and PET. J Nucl Med 46:240–247
Gamarel KE, Westfall AO, Lally MA, Hosek S, Wilson CM, Adolescent Medicine Trials Network for HIVAI (2018) Tobacco Use and Sustained Viral Suppression in Youth Living with HIV. AIDS Behav 22:2018–2025. https://doi.org/10.1007/s10461-017-1915-2
Gao Z, Nissen JC, Ji K, Tsirka SE (2014) The experimental autoimmune encephalomyelitis disease course is modulated by nicotine and other cigarette smoke components. PLoS One 9:e107979. https://doi.org/10.1371/journal.pone.0107979
Gao X, Zhang Y, Breitling LP, Brenner H (2016) Tobacco smoking and methylation of genes related to lung cancer development. Oncotarget 7:59017–59028. https://doi.org/10.18632/oncotarget.10007
Garcia-Arcos I et al (2016) Chronic electronic cigarette exposure in mice induces features of COPD in a nicotine-dependent manner. Thorax 71:1119–1129. https://doi.org/10.1136/thoraxjnl-2015-208039
Garvey LJ, Pavese N, Politis M, Ramlackhansingh A, Brooks DJ, Taylor-Robinson SD, Winston A (2014) Increased microglia activation in neurologically asymptomatic HIV-infected patients receiving effective ART. AIDS 28:67–72. https://doi.org/10.1097/01.aids.0000432467.54003.f7
Gatch MB et al (2013) The HIV Antiretroviral Drug Efavirenz has LSD-Like Properties. Neuropsychopharmacology 38:2373–2384. https://doi.org/10.1038/npp.2013.135
Ghosh D, Mishra MK, Das S, Kaushik DK, Basu A (2009) Tobacco carcinogen induces microglial activation and subsequent neuronal damage. J Neurochem 110:1070–1081. https://doi.org/10.1111/j.1471-4159.2009.06203.x
Goncalves RB, Coletta RD, Silverio KG, Benevides L, Casati MZ, da Silva JS, Nociti FH Jr (2011) Impact of smoking on inflammation: overview of molecular mechanisms. Inflamm Res 60:409–424. https://doi.org/10.1007/s00011-011-0308-7
Grelotti DJ et al (2014) Whoonga: Potential recreational use of HIV antiretroviral medication in South Africa. AIDS Behav 18:511–518. https://doi.org/10.1007/s10461-013-0575-0
Gu DF, Hinks LJ, Morton NE, Day IN (2000) The use of long PCR to confirm three common alleles at the CYP2A6 locus and the relationship between genotype and smoking habit. Ann Hum Genet 64:383–390
Guo Q et al (2013) Quantification of the specific translocator protein signal of 18F-PBR111 in healthy humans: a genetic polymorphism effect on in vivo binding. J Nucl Med 54:1915–1923. https://doi.org/10.2967/jnumed.113.121020
Guttman Y, Nudel A, Kerem Z (2019) Polymorphism in Cytochrome P450 3A4 Is Ethnicity Related. Front Genet 10:224. https://doi.org/10.3389/fgene.2019.00224
Hajek P et al (2019) A Randomized Trial of E-Cigarettes versus Nicotine-Replacement. Therapy N Engl J Med 380:629–637. https://doi.org/10.1056/NEJMoa1808779
Hall HI et al (2008) Estimation of HIV incidence in the United States. JAMA 300:520–529. https://doi.org/10.1001/jama.300.5.520
Hall ME et al (2016) Cigarette Smoking and Chronic Kidney Disease in African Americans in the Jackson Heart Study. J Am Heart Assoc:5. https://doi.org/10.1161/JAHA.116.003280
Hamano R, Takahashi HK, Iwagaki H, Yoshino T, Nishibori M, Tanaka N (2006) Stimulation of alpha7 nicotinic acetylcholine receptor inhibits CD14 and the toll-like receptor 4 expression in human monocytes. Shock 26:358–364. https://doi.org/10.1097/01.shk.0000228168.86845.60
Hammoud DA et al (2005) Imaging glial cell activation with [11C]-R-PK11195 in patients with AIDS. J Neurovirol 11:346–355. https://doi.org/10.1080/13550280500187351
Han H, Yang Z, Chang SL, Li MD (2018) Modulatory Effects of Nicotine on neuroHIV/neuroAIDS. J Neuroimmune Pharmacol 13:467–478. https://doi.org/10.1007/s11481-018-9806-5
Harrison JD et al (2017) The nature and consequences of cognitive deficits among tobacco smokers with HIV: a comparison to tobacco smokers without HIV. J Neurovirol 23:550–557. https://doi.org/10.1007/s13365-017-0526-z
Hasday JD, Bascom R, Costa JJ, Fitzgerald T, Dubin W (1999) Bacterial endotoxin is an active component of cigarette smoke. Chest 115:829–835. https://doi.org/10.1378/chest.115.3.829
Hawkins BT, Abbruscato TJ, Egleton RD, Brown RC, Huber JD, Campos CR, Davis TP (2004) Nicotine increases in vivo blood-brain barrier permeability and alters cerebral microvascular tight junction protein distribution. Brain Res 1027:48–58. https://doi.org/10.1016/j.brainres.2004.08.043
Heaton RK et al (2010) HIV-associated neurocognitive disorders persist in the era of potent antiretroviral therapy: CHARTER Study. Neurology 75:2087–2096. https://doi.org/10.1212/WNL.0b013e318200d727
Heaton RK et al (2011) HIV-associated neurocognitive disorders before and during the era of combination antiretroviral therapy: differences in rates, nature, and predictors. J Neurovirol 17:3–16. https://doi.org/10.1007/s13365-010-0006-1
Heaton RK et al (2015) Neurocognitive change in the era of HIV combination antiretroviral therapy: the longitudinal CHARTER study. Clin Infect Dis 60:473–480. https://doi.org/10.1093/cid/ciu862
Helleberg M et al (2013) Mortality attributable to smoking among HIV-1-infected individuals: a nationwide, population-based cohort study. Clin Infect Dis 56:727–734. https://doi.org/10.1093/cid/cis933
Helleberg M et al (2015) Smoking and life expectancy among HIV-infected individuals on antiretroviral therapy in Europe and North America. AIDS 29:221–229. https://doi.org/10.1097/qad.0000000000000540
Henry TS, Kanne JP, Kligerman SJ (2019) Imaging of Vaping-Associated Lung Disease New England. J Med. https://doi.org/10.1056/NEJMc1911995
Herrero P et al (2012) Feasibility and dosimetry studies for 18F-NOS as a potential PET radiopharmaceutical for inducible nitric oxide synthase in humans. J Nucl Med 53:994–1001. https://doi.org/10.2967/jnumed.111.088518
Herron JW, Nerurkar L, Cavanagh J (2018) Neuroimmune Biomarkers in Mental Illness. Curr Top Behav Neurosci 40:45–78. https://doi.org/10.1007/7854_2018_45
Hillmer AT et al (2016) Imaging of cerebral alpha4beta2* nicotinic acetylcholine receptors with (-)-[(18)F]Flubatine PET: Implementation of bolus plus constant infusion and sensitivity to acetylcholine in human brain. Neuroimage 141:71–80. https://doi.org/10.1016/j.neuroimage.2016.07.026
Hitsman B, Moss TG, Montoya ID, George TP (2009) Treatment of tobacco dependence in mental health and addictive disorders. Can J Psychiatry 54:368–378. https://doi.org/10.1177/070674370905400604
Hitsman B et al (2013) Past major depression and smoking cessation outcome: a systematic review and meta-analysis update. Addiction 108:294–306. https://doi.org/10.1111/add.12009
Hom S, Chen L, Wang T, Ghebrehiwet B, Yin W, Rubenstein DA (2016) Platelet activation, adhesion, inflammation, and aggregation potential are altered in the presence of electronic cigarette extracts of variable nicotine concentrations. Platelets 27:694–702. https://doi.org/10.3109/09537104.2016.1158403
Hopkins RO, Weaver LK, Pope D, Orme JF, Bigler ED, Larson LV (1999) Neuropsychological sequelae and impaired health status in survivors of severe acute respiratory distress syndrome. Am J Respir Crit Care Med 160:50–56. https://doi.org/10.1164/ajrccm.160.1.9708059
Horti AG et al (1998) 2-[18F]Fluoro-A-85380, an in vivo tracer for the nicotinic acetylcholine receptors. Nucl Med Biol 25:599–603. https://doi.org/10.1016/s0969-8051(98)00031-6
Hossain M et al (2009) Tobacco smoke: a critical etiological factor for vascular impairment at the blood-brain barrier. Brain Res 1287:192–205. https://doi.org/10.1016/j.brainres.2009.06.033
Hua P, Feng W, Ji S, Raij L, Jaimes EA (2010) Nicotine worsens the severity of nephropathy in diabetic mice: implications for the progression of kidney disease in smokers. Am J Physiol Renal Physiol 299:F732–F739. https://doi.org/10.1152/ajprenal.00293.2010
Hukkanen J, Jacob P 3rd, Benowitz NL (2005) Metabolism and disposition kinetics of nicotine. Pharmacol Rev 57:79–115. https://doi.org/10.1124/pr.57.1.3
Humfleet GL, Hall SM, Delucchi KL, Dilley JW (2013) A randomized clinical trial of smoking cessation treatments provided in HIV clinical care settings. Nicotine Tob Res 15:1436–1445. https://doi.org/10.1093/ntr/ntt005
Hunt PW, Lee SA, Siedner MJ (2016) Immunologic Biomarkers, Morbidity, and Mortality in Treated HIV Infection. J Infect Dis 214(Suppl 2):S44–S50. https://doi.org/10.1093/infdis/jiw275
Imboden M et al (2019) Epigenome-wide association study of lung function level and its change. Eur Respir J:54. https://doi.org/10.1183/13993003.00457-2019
Irunde JI, Luboobi LS, Nkansah-Gyekye Y (2017) Modeling tobacco smoking effect on HIV antiretroviral therapy. J Math Comput Sci 7:1046–1073
Jain G, Jaimes EA (2013) Nicotine signaling and progression of chronic kidney disease in smokers. Biochem Pharmacol 86:1215–1223. https://doi.org/10.1016/j.bcp.2013.07.014
Jamal A, King BA, Neff LJ, Whitmill J, Babb SD, Graffunder CM (2016) Current Cigarette Smoking Among Adults - United States, 2005-2015. MMWR Morb Mortal Wkly Rep 65:1205–1211. https://doi.org/10.15585/mmwr.mm6544a2
Jin M et al (2012) A LC-MS/MS method for concurrent determination of nicotine metabolites and role of CYP2A6 in nicotine metabolism in U937 macrophages: implications in oxidative stress in HIV + smokers. J Neuroimmune Pharmacol 7:289–299. https://doi.org/10.1007/s11481-011-9283-6
Jones DK, Knosche TR, Turner R (2013) White matter integrity, fiber count, and other fallacies: the do’s and don’ts of diffusion MRI. Neuroimage 73:239–254. https://doi.org/10.1016/j.neuroimage.2012.06.081
Kalkman HO, Feuerbach D (2016) Modulatory effects of alpha7 nAChRs on the immune system and its relevance for CNS disorders. Cell Mol Life Sci 73:2511–2530. https://doi.org/10.1007/s00018-016-2175-4
Kaneki M, Shimizu N, Yamada D, Chang K (2007) Nitrosative stress and pathogenesis of insulin resistance. Antioxid Redox Signal 9:319–329. https://doi.org/10.1089/ars.2006.1464
Kaufmann A et al (2015) Rate of nicotine metabolism and smoking cessation outcomes in a community-based sample of treatment-seeking smokers. Addict Behav 51:93–99. https://doi.org/10.1016/j.addbeh.2015.07.019
Keith A, Dong Y, Shuter J, Himelhoch S (2016) Behavioral Interventions for Tobacco Use in HIV-Infected Smokers: A Meta-Analysis. J Acquir Immune Defic Syndr 72:527–533. https://doi.org/10.1097/qai.0000000000001007
Kianoush S et al (2017) Association Between Smoking and Serum GlycA and High-Sensitivity C-Reactive Protein Levels: The Multi-Ethnic Study of Atherosclerosis (MESA) and Brazilian Longitudinal Study of Adult Health (ELSA-Brasil). J Am Heart Assoc 6. https://doi.org/10.1161/jaha.117.006545
Kim YK, Shin C (2018) The Microbiota-Gut-Brain Axis in Neuropsychiatric Disorders: Pathophysiological Mechanisms and Novel Treatments. Curr Neuropharmacol 16:559–573. https://doi.org/10.2174/1570159x15666170915141036
Kimes AS, Chefer SI, Matochik JA, Contoreggi CS, Vaupel DB, Stein EA, Mukhin AG (2008) Quantification of nicotinic acetylcholine receptors in the human brain with PET: bolus plus infusion administration of 2-[18F]F-A85380. Neuroimage 39:717–727. https://doi.org/10.1016/j.neuroimage.2007.09.015
King CC, Piper ME, Gepner AD, Fiore MC, Baker TB, Stein JH (2017) Longitudinal Impact of Smoking and Smoking Cessation on Inflammatory Markers of Cardiovascular Disease Risk. Arterioscler Thromb Vasc Biol 37:374–379. https://doi.org/10.1161/atvbaha.116.308728
Koch A et al (2007) Inducible NO synthase expression in endomyocardial biopsies after heart transplantation in relation to the postoperative course. Eur J Cardiothorac Surg 32:639–643. https://doi.org/10.1016/j.ejcts.2007.06.041
Kodidela S, Ranjit S, Sinha N, McArthur C, Kumar A, Kumar S (2018) Cytokine profiling of exosomes derived from the plasma of HIV-infected alcohol drinkers and cigarette smokers. PLoS One 13:e0201144. https://doi.org/10.1371/journal.pone.0201144
Kreisl WC et al (2013) A genetic polymorphism for translocator protein 18 kDa affects both in vitro and in vivo radioligand binding in human brain to this putative biomarker of neuroinflammation. J Cereb Blood Flow Metab 33:53–58. https://doi.org/10.1038/jcbfm.2012.131
Krishnan-Sarin S et al (2007) Behavioral impulsivity predicts treatment outcome in a smoking cessation program for adolescent smokers. Drug Alcohol Depend 88:79–82. https://doi.org/10.1016/j.drugalcdep.2006.09.006
Kubota T et al (2006) CYP2A6 polymorphisms are associated with nicotine dependence and influence withdrawal symptoms in smoking cessation. Pharmacogenomics J 6:115–119. https://doi.org/10.1038/sj.tpj.6500348
Kumar S, Rao PS, Earla R, Kumar A (2015) Drug-drug interactions between anti-retroviral therapies and drugs of abuse in HIV systems. Expert Opin Drug Metab Toxicol 11:343–355. https://doi.org/10.1517/17425255.2015.996546
Kuwabara H et al (2012) PET Imaging of nicotinic acetylcholine receptors in baboons with 18F-AZAN, a radioligand with improved brain kinetics. J Nucl Med 53:121–129. https://doi.org/10.2967/jnumed.111.092338
Larsson L, Pehrson C, Dechen T, Crane-Godreau M (2012) Microbiological components in mainstream and sidestream cigarette smoke. Tobacco Induced Diseases 10:13. https://doi.org/10.1186/1617-9625-10-13
Layden JE et al (2019) Pulmonary Illness Related to E-Cigarette Use in Illinois and Wisconsin — Preliminary Report. New Engl J Med. https://doi.org/10.1056/NEJMoa1911614
Lechner M, Lirk P, Rieder J (2005) Inducible nitric oxide synthase (iNOS) in tumor biology: the two sides of the same coin Semin. Cancer Biol 15:277–289. https://doi.org/10.1016/j.semcancer.2005.04.004
Lederman MM, Funderburg NT, Sekaly RP, Klatt NR, Hunt PW (2013) Residual immune dysregulation syndrome in treated HIV infection. Adv Immunol 119:51–83. https://doi.org/10.1016/b978-0-12-407707-2.00002-3
Ledgerwood DM, Yskes R (2016) Smoking Cessation for People Living With HIV/AIDS: A Literature Review and Synthesis. Nicotine Tob Res 18:2177–2184. https://doi.org/10.1093/ntr/ntw126
Lerman C, Tyndale R, Patterson F, Wileyto EP, Shields PG, Pinto A, Benowitz N (2006) Nicotine metabolite ratio predicts efficacy of transdermal nicotine for smoking cessation. Clin Pharmacol Ther 79:600–608. https://doi.org/10.1016/j.clpt.2006.02.006
Lerman C et al (2015) Use of the nicotine metabolite ratio as a genetically informed biomarker of response to nicotine patch or varenicline for smoking cessation: a randomised, double-blind placebo-controlled trial. Lancet Respir Med 3:131–138. https://doi.org/10.1016/S2213-2600(14)70294-2
Liang H, Chang L, Chen R, Oishi K, Ernst T (2018) Independent and Combined Effects of Chronic HIV-Infection and Tobacco Smoking on Brain Microstructure. J Neuroimmune Pharmacol 13:509–522. https://doi.org/10.1007/s11481-018-9810-9
Liu L et al (2017) Alpha7 nicotinic acetylcholine receptor is required for amyloid pathology in brain endothelial cells induced by Glycoprotein 120, methamphetamine and nicotine. Sci Rep 7:40467. https://doi.org/10.1038/srep40467
Lotfipour S, Mandelkern M, Brody AL (2011) Quantitative Molecular Imaging of Neuronal Nicotinic Acetylcholine Receptors in the Human Brain with A-85380 Radiotracers. Curr Med Imaging Rev 7:107–112. https://doi.org/10.2174/157340511795445676
Lotfipour S, Mandelkern M, Alvarez-Estrada M, Brody AL (2012) A single administration of low-dose varenicline saturates alpha4beta2* nicotinic acetylcholine receptors in the human brain. Neuropsychopharmacology 37:1738–1748. https://doi.org/10.1038/npp.2012.20
Loughead J, Wileyto EP, Ruparel K, Falcone M, Hopson R, Gur R, Lerman C (2015) Working memory-related neural activity predicts future smoking relapse. Neuropsychopharmacology 40:1311–1320. https://doi.org/10.1038/npp.2014.318
Maddock SD, Cirulis MM, Callahan SJ, Keenan LM, Pirozzi CS, Raman SM, Aberegg SK (2019) Pulmonary Lipid-Laden Macrophages and Vaping. N Engl J Med. https://doi.org/10.1056/NEJMc1912038
Mahy M, Autenrieth CS, Stanecki K, Wynd S (2014) Increasing trends in HIV prevalence among people aged 50 years and older: evidence from estimates and survey data AIDS 28 Suppl 4:S453-S459 doi:https://doi.org/10.1097/QAD.0000000000000479
Manda VK, Mittapalli RK, Bohn KA, Adkins CE, Lockman PR (2010a) Nicotine and cotinine increases the brain penetration of saquinavir in rat. J Neurochem 115:1495–1507. https://doi.org/10.1111/j.1471-4159.2010.07054.x
Manda VK, Mittapalli RK, Geldenhuys WJ, Lockman PR (2010b) Chronic exposure to nicotine and saquinavir decreases endothelial Notch-4 expression and disrupts blood-brain barrier integrity. J Neurochem 115:515–525. https://doi.org/10.1111/j.1471-4159.2010.06948.x
McArthur JC, Steiner J, Sacktor N, Nath A (2010) Human immunodeficiency virus-associated neurocognitive disorders: Mind the gap. Ann Neurol 67:699–714. https://doi.org/10.1002/ana.22053
McDonagh EM, Lau JL, Alvarellos ML, Altman RB, Klein TE (2015) PharmGKB summary: Efavirenz pathway, pharmacokinetics. Pharmacogenet Genomics 25:363–376. https://doi.org/10.1097/FPC.0000000000000145
McEvoy JW et al (2015) Relationship of cigarette smoking with inflammation and subclinical vascular disease: the Multi-Ethnic Study of Atherosclerosis. Arterioscler Thromb Vasc Biol 35:1002–1010. https://doi.org/10.1161/atvbaha.114.304960
Mdodo R, Frazier EL, Dube SR, Mattson CL, Sutton MY, Brooks JT, Skarbinski J (2015) Cigarette smoking prevalence among adults with HIV compared with the general adult population in the United States: cross-sectional surveys. Ann Intern Med 162:335–344. https://doi.org/10.7326/M14-0954
Mendelson JH, Sholar MB, Goletiani N, Siegel AJ, Mello NK (2005) Effects of low- and high-nicotine cigarette smoking on mood states and the HPA axis in men. Neuropsychopharmacology 30:1751–1763. https://doi.org/10.1038/sj.npp.1300753
Mercie P et al (2018) Efficacy and safety of varenicline for smoking cessation in people living with HIV in France (ANRS 144 Inter-ACTIV): a randomised controlled phase 3 clinical trial. Lancet HIV 5:e126–e135. https://doi.org/10.1016/s2352-3018(18)30002-x
Messner B, Bernhard D (2014) Smoking and cardiovascular disease: mechanisms of endothelial dysfunction and early atherogenesis. Arterioscler Thromb Vasc Biol 34:509–515. https://doi.org/10.1161/ATVBAHA.113.300156
Midde NM, Gomez AM, Harrod SB, Zhu J (2011) Genetically expressed HIV-1 viral proteins attenuate nicotine-induced behavioral sensitization and alter mesocorticolimbic ERK and CREB signaling in rats. Pharmacol Biochem Behav 98:587–597. https://doi.org/10.1016/j.pbb.2011.03.013
Miguez-Burbano MJ, Wyatt C, Lewis JE, Rodriguez A, Duncan R (2010) Ignoring the obvious missing piece of chronic kidney disease in HIV: cigarette smoking. J Assoc Nurses AIDS Care 21:16–24. https://doi.org/10.1016/j.jana.2009.07.005
Mirbolouk M et al (2018) Prevalence and Distribution of E-Cigarette Use Among U.S. Adults: Behavioral Risk Factor Surveillance System, 2016. Ann Intern Med 169:429–438. https://doi.org/10.7326/M17-3440
Modjarrad K, Vermund SH (2010) Effect of treating co-infections on HIV-1 viral load: a systematic review. Lancet Infect Dis 10:455–463. https://doi.org/10.1016/S1473-3099(10)70093-1
Moheimani RS, Bhetraratana M, Yin F, Peters KM, Gornbein J, Araujo JA, Middlekauff HR (2017) Increased Cardiac Sympathetic Activity and Oxidative Stress in Habitual Electronic Cigarette Users: Implications for Cardiovascular Risk. JAMA Cardiol 2:278–284. https://doi.org/10.1001/jamacardio.2016.5303
Möller M, Fourie J, Harvey BH (2018) Efavirenz exposure, alone and in combination with known drugs of abuse, engenders addictive-like bio-behavioural changes in rats. Sci Rep 8:12837. https://doi.org/10.1038/s41598-018-29978-3
Monnig MA, Kahler CW, Lee H, Pantalone DW, Mayer KH, Cohen RA, Monti PM (2016) Effects of smoking and alcohol use on neurocognitive functioning in heavy drinking, HIV-positive men who have sex with men. AIDS Care 28:300–305. https://doi.org/10.1080/09540121.2015.1093595
Mu Y, Patters BJ, Midde NM, He H, Kumar S, Cory TJ (2018) Tobacco and Antiretrovirals Modulate Transporter, Metabolic Enzyme, and Antioxidant Enzyme Expression and Function in Polarized Macrophages. Curr HIV Res 16:354–363. https://doi.org/10.2174/1570162X17666190130114531
Muiru AN et al (2019) Kidney disease risk factors associate with urine biomarkers concentrations in HIV-positive persons; a cross-sectional study. BMC Nephrol 20:4. https://doi.org/10.1186/s12882-018-1192-y
Mumaw CL et al (2016) Microglial priming through the lung-brain axis: the role of air pollution-induced circulating factors. FASEB J 30:1880–1891. https://doi.org/10.1096/fj.201500047
Naik P et al (2014) Oxidative and pro-inflammatory impact of regular and denicotinized cigarettes on blood brain barrier endothelial cells: is smoking reduced or nicotine-free products really safe? BMC Neurosci 15:51. https://doi.org/10.1186/1471-2202-15-51
Nanni MG, Caruso R, Mitchell AJ, Meggiolaro E, Grassi L (2015) Depression in HIV infected patients: a review. Curr Psy Rep 17:530. https://doi.org/10.1007/s11920-014-0530-4
Nesil T, Cao J, Yang Z, Chang SL, Li MD (2015) Nicotine attenuates the effect of HIV-1 proteins on the neural circuits of working and contextual memories. Mol Brain 8:43. https://doi.org/10.1186/s13041-015-0134-x
Notter T, Coughlin JM, Sawa A, Meyer U (2018) Reconceptualization of translocator protein as a biomarker of neuroinflammation in psychiatry. Mol Psychiatry 23:36–47. https://doi.org/10.1038/mp.2017.232
Ogunwale MA, Li M, Ramakrishnam Raju MV, Chen Y, Nantz MH, Conklin DJ, Fu XA (2017) Aldehyde Detection in Electronic Cigarette Aerosols. ACS Omega 2:1207–1214. https://doi.org/10.1021/acsomega.6b00489
Pacek LR, Cioe PA (2015) Tobacco Use, Use Disorders, and Smoking Cessation Interventions in Persons Living With HIV. Curr HIV/AIDS Rep 12:413–420. https://doi.org/10.1007/s11904-015-0281-9
Pacek LR, Crum RM (2015) A Review of the Literature Concerning HIV and Cigarette Smoking: Morbidity and Mortality, Associations with Individual- and Social-Level Characteristics, and Smoking Cessation Efforts. Addict Res Theory 23:10–23. https://doi.org/10.3109/16066359.2014.920013
Pacek LR, Rass O, Johnson MW (2017) Positive smoking cessation-related interactions with HIV care providers increase the likelihood of interest in cessation among HIV-positive cigarette smokers. AIDS Care 29:1309–1314. https://doi.org/10.1080/09540121.2017.1330532
Pal D, Mitra AK (2006) MDR- and CYP3A4-mediated drug-drug interactions. J Neuroimmune Pharmacol 1:323–339. https://doi.org/10.1007/s11481-006-9034-2
Pal D, Kwatra D, Minocha M, Paturi DK, Budda B, Mitra AK (2011) Efflux transporters- and cytochrome P-450-mediated interactions between drugs of abuse and antiretrovirals. Life Sci 88:959–971. https://doi.org/10.1016/j.lfs.2010.09.012
Palella FJ, Jr. et al. (1998) Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. HIV Outpatient Study Investigators N Engl J Med 338:853-860 https://doi.org/10.1056/NEJM199803263381301
Patterson F et al (2010) Working memory deficits predict short-term smoking resumption following brief abstinence. Drug Alcohol Depend 106:61–64. https://doi.org/10.1016/j.drugalcdep.2009.07.020
Paul RH et al (2006) Cognitive status of young and older cigarette smokers: data from the international brain database. J Clin Neurosci 13:457–465. https://doi.org/10.1016/j.jocn.2005.04.012
Peres FS, Barreto SM, Camelo LV, Ribeiro ALP, Vidigal PG, Duncan BB, Giatti L (2017) Time From Smoking Cessation and Inflammatory Markers: New Evidence From a Cross-Sectional Analysis of ELSA-Brasil. Nicotine Tob Res 19:852–858. https://doi.org/10.1093/ntr/ntx032
Piliguian M, Zhu AZ, Zhou Q, Benowitz NL, Ahluwalia JS, Sanderson Cox L, Tyndale RF (2014) Novel CYP2A6 variants identified in African Americans are associated with slow nicotine metabolism in vitro and in vivo. Pharmacogenet Genomics 24:118–128. https://doi.org/10.1097/FPC.0000000000000026
Pollack TM, Duong HT, Pham TT, Do CD, Colby D (2017) Cigarette smoking is associated with high HIV viral load among adults presenting for antiretroviral therapy in Vietnam. PLoS One 12:e0173534. https://doi.org/10.1371/journal.pone.0173534
Pool ER, Dogar O, Lindsay RP, Weatherburn P, Siddiqi K (2016) Interventions for tobacco use cessation in people living with HIV and AIDS. Cochrane Database Syst Rev:CD011120. https://doi.org/10.1002/14651858.CD011120.pub2
Portilla I et al (2019) Neurocognitive Impairment in Well-Controlled HIV-Infected Patients: A Cross-Sectional Study. AIDS Res Hum Retroviruses 35:634–641. https://doi.org/10.1089/aid.2018.0279
Powell JH, Pickering AD, Dawkins L, West R, Powell JF (2004) Cognitive and psychological correlates of smoking abstinence, and predictors of successful cessation. Addict Behav 29:1407–1426
Prasad K, Dhar I, Caspar-Bell G (2015) Role of Advanced Glycation End Products and Its Receptors in the Pathogenesis of Cigarette Smoke-Induced Cardiovascular Disease. Int J Angiol 24:75–80. https://doi.org/10.1055/s-0034-1396413
Pratt LA, Brody DJ (2010) Depression and smoking in the U.S. household population aged 20 and over, 2005-2008 NCHS Data Brief:1-8
Qasim H, Karim ZA, Rivera JO, Khasawneh FT, Alshbool FZ (2017) Impact of Electronic Cigarettes on the Cardiovascular System. J Am Heart Assoc:6. https://doi.org/10.1161/jaha.117.006353
Quik M, Perez XA, Bordia T (2012) Nicotine as a potential neuroprotective agent for Parkinson’s disease. Mov Disord 27:947–957. https://doi.org/10.1002/mds.25028
Rahmioglu N et al (2011) Genetic epidemiology of induced CYP3A4 activity. Pharmacogenet Genomics:21, 642–651. https://doi.org/10.1097/FPC.0b013e3283498ecf
Ramos FM, Delgado-Velez M, Ortiz AL, Baez-Pagan CA, Quesada O, Lasalde-Dominicci JA (2016) Expression of CHRFAM7A and CHRNA7 in neuronal cells and postmortem brain of HIV-infected patients: considerations for HIV-associated neurocognitive disorder. J Neurovirol 22:327–335. https://doi.org/10.1007/s13365-015-0401-8
Ranjit S, Sinha N, Kodidela S, Kumar S (2018) Benzo(a)pyrene in Cigarette Smoke Enhances HIV-1 Replication through NF-kappaB Activation via CYP-Mediated Oxidative Stress Pathway. Sci Rep 8:10394. https://doi.org/10.1038/s41598-018-28500-z
Rao P, Ande A, Sinha N, Kumar A, Kumar S (2016) Effects of Cigarette Smoke Condensate on Oxidative Stress, Apoptotic Cell Death, and HIV Replication in Human Monocytic Cells. PLoS One 11:e0155791. https://doi.org/10.1371/journal.pone.0155791
Reddy KP et al (2017) Lung Cancer Mortality Associated With Smoking and Smoking Cessation Among People Living With HIV in the United States. JAMA Intern Med 177:1613–1621. https://doi.org/10.1001/jamainternmed.2017.4349
Robertson K, Yosief S (2014) Neurocognitive assessment in the diagnosis of HIV-associated neurocognitive disorders. Semin Neurol 34:21–26. https://doi.org/10.1055/s-0034-1372339
Robertson K, Landay A, Miyahara S, Vecchio A, Masters MC, Brown TT, Taiwo BO (2019) Limited correlation between systemic biomarkers and neurocognitive performance before and during HIV treatment. J Neurovirol. https://doi.org/10.1007/s13365-019-00795-2
Rock RB, Gekker G, Aravalli RN, Hu S, Sheng WS, Peterson PK (2008) Potentiation of HIV-1 expression in microglial cells by nicotine: involvement of transforming growth factor-beta 1. J Neuroimmune Pharmacol 3:143–149. https://doi.org/10.1007/s11481-007-9098-7
Rodgman A, Perfetti TA (2013) The Chemical Components of Tobacco and Tobacco Smoke. 2nd edn. CRC Press, Taylor & Francis Group,
Rohleder N, Kirschbaum C (2006) The hypothalamic-pituitary-adrenal (HPA) axis in habitual smokers. Int J Psychophysiol 59:236–243. https://doi.org/10.1016/j.ijpsycho.2005.10.012
Rosenblat JD, Cha DS, Mansur RB, McIntyre RS (2014) Inflamed moods: a review of the interactions between inflammation and mood disorders. Prog Neuropsychopharmacol Biol Psychiatry 53:23–34. https://doi.org/10.1016/j.pnpbp.2014.01.013
Rubin LH, Maki PM (2019) HIV, Depression, and Cognitive Impairment in the Era of Effective Antiretroviral Therapy. Curr HIV/AIDS Rep 16:82–95. https://doi.org/10.1007/s11904-019-00421-0
Rusjan PM, Wilson AA, Bloomfield PM, Vitcu I, Meyer JH, Houle S, Mizrahi R (2011) Quantitation of translocator protein binding in human brain with the novel radioligand [18F]-FEPPA and positron emission tomography. J Cereb Blood Flow Metab 31:1807–1816. https://doi.org/10.1038/jcbfm.2011.55
Sabri O et al (2015) First-in-human PET quantification study of cerebral alpha4beta2* nicotinic acetylcholine receptors using the novel specific radioligand (-)-[(18)F]Flubatine. Neuroimage 118:199–208. https://doi.org/10.1016/j.neuroimage.2015.05.065
Sacktor N et al (2016) Prevalence of HIV-associated neurocognitive disorders in the Multicenter AIDS Cohort Study. Neurology 86:334–340. https://doi.org/10.1212/wnl.0000000000002277
Samji H et al (2013) Closing the gap: increases in life expectancy among treated HIV-positive individuals in the United States and Canada. PLoS One 8:e81355. https://doi.org/10.1371/journal.pone.0081355
Santos G-M, Tan J, Turner C, Raymond HF (2019) Demographic, Behavioral, and Social Characteristics Associated With Smoking and Vaping Among Men Who Have Sex With Men in San Francisco Am J Mens Health 13:1557988319847833 doi:https://doi.org/10.1177/1557988319847833
Scheffler S, Dieken H, Krischenowski O, Forster C, Branscheid D, Aufderheide M (2015) Evaluation of E-cigarette liquid vapor and mainstream cigarette smoke after direct exposure of primary human bronchial epithelial cells. Int J Environ Res Public Health 12:3915–3925. https://doi.org/10.3390/ijerph120403915
Schnoll RA, Patterson F, Wileyto EP, Tyndale RF, Benowitz N, Lerman C (2009) Nicotine metabolic rate predicts successful smoking cessation with transdermal nicotine: a validation study. Pharmacol Biochem Behav 92:6–11. https://doi.org/10.1016/j.pbb.2008.10.016
Schnoll RA et al (2019) Brief Report: Rate of Nicotine Metabolism and Tobacco Use Among Persons With HIV: Implications for Treatment and Research. J Acquir Immune Defic Syndr 80:e36–e40. https://doi.org/10.1097/QAI.0000000000001895
Schouten J, Cinque P, Gisslen M, Reiss P, Portegies P (2011) HIV-1 infection and cognitive impairment in the cART era: a review. AIDS 25:561–575. https://doi.org/10.1097/QAD.0b013e3283437f9a
Shah A, Gangwani MR, Chaudhari NS, Glazyrin A, Bhat HK, Kumar A (2016) Neurotoxicity in the Post-HAART Era: Caution for the Antiretroviral Therapeutics. Neurotoxicity Res 30:677–697. https://doi.org/10.1007/s12640-016-9646-0
Shi FD, Piao WH, Kuo YP, Campagnolo DI, Vollmer TL, Lukas RJ (2009) Nicotinic attenuation of central nervous system inflammation and autoimmunity. J Immunol 182:1730–1739. https://doi.org/10.4049/jimmunol.182.3.1730
Shields PG et al (2017) A Review of Pulmonary Toxicity of Electronic Cigarettes in the Context of Smoking: A Focus on Inflammation. Cancer Epidemiol Biomarkers Prev 26:1175–1191. https://doi.org/10.1158/1055-9965.Epi-17-0358
Shiels MS et al (2014) Cigarette smoking and variations in systemic immune and inflammation markers. J Natl Cancer Inst 106. https://doi.org/10.1093/jnci/dju294
Shimohama S, Kawamata J (2018) Roles of nicotinic acetylcholine receptors in the pathology and treatment of Alzheimer’s and Parkinson’s diseases. In: Akaike A, Shimohama S, Misu Y, Akaike A, Shimohama S, Misu Y (eds) Nicotinic acetylcholine receptor signaling in neuroprotection. Springer Singapore, Singapore, p 137–158
Shizu M et al (2008) Cigarette smoke condensate upregulates the gene and protein expression of proinflammatory cytokines in human fibroblast-like synoviocyte line. J Interferon Cytokine Res 28:509–521. https://doi.org/10.1089/jir.2007.0081
Singh T, Arrazola RA, Corey CG, Husten CG, Neff LJ, Homa DM, King BA (2016) Tobacco use among middle and high school students--United States, 2011-2015. MMWR Morb Mortal Wkly Rep 65:361–367
Sivandzade F, Cucullo L (2019) Assessing the protective effect of rosiglitazone against electronic cigarette/tobacco smoke-induced blood-brain barrier impairment. BMC Neurosci 20:15. https://doi.org/10.1186/s12868-019-0497-5
Smith KJ, Lassmann H (2002) The role of nitric oxide in multiple sclerosis. Lancet Neurol 1:232–241
Sopori M (2002) Effects of cigarette smoke on the immune system. Nat Rev Immunol 2:372–377. https://doi.org/10.1038/nri803
Spira A et al (2004) Effects of cigarette smoke on the human airway epithelial cell transcriptome. Proc Natl Acad Sci U S A 101:10143–10148. https://doi.org/10.1073/pnas.0401422101
Stampfli MR, Anderson GP (2009) How cigarette smoke skews immune responses to promote infection, lung disease and cancer. Nat Rev Immunol 9:377–384. https://doi.org/10.1038/nri2530
Steel HC et al (2018) Effects of Tobacco Usage and Antiretroviral Therapy on Biomarkers of Systemic Immune Activation in HIV-Infected Participants. Mediators Inflamm 2018:8357109. https://doi.org/10.1155/2018/8357109
Stevens RD, Puybasset L (2011) The brain-lung-brain axis. Intensive Care Med 37:1054–1056. https://doi.org/10.1007/s00134-011-2233-1
Stroud JC, Oltman A, Han A, Bates DL, Chen L (2009) Structural basis of HIV-1 activation by NF-kappaB--a higher-order complex of p50:RelA bound to the HIV-1 LTR. J Mol Biol 393:98–112. https://doi.org/10.1016/j.jmb.2009.08.023
Sullivan JP et al (1996) A-85380 [3-(2(S)-azetidinylmethoxy) pyridine]: in vitro pharmacological properties of a novel, high affinity alpha 4 beta 2 nicotinic acetylcholine receptor ligand. Neuropharmacology 35:725–734. https://doi.org/10.1016/0028-3908(96)84644-2
Suzuki T et al (2006) Microglial alpha7 nicotinic acetylcholine receptors drive a phospholipase C/IP3 pathway and modulate the cell activation toward a neuroprotective role. J Neurosci Res 83:1461–1470. https://doi.org/10.1002/jnr.20850
Taghavi T, St Helen G, Benowitz NL, Tyndale RF (2017) Effect of UGT2B10, UGT2B17, FMO3, and OCT2 genetic variation on nicotine and cotinine pharmacokinetics and smoking in African Americans. Pharmacogenet Genomics 27:143–154. https://doi.org/10.1097/fpc.0000000000000269
Tanner JA, Tyndale RF (2017) Variation in CYP2A6 Activity and Personalized Medicine. J Pers Med 7. https://doi.org/10.3390/jpm7040018
Thames AD, Arentoft A, Rivera-Mindt M, Hinkin CH (2013) Functional disability in medication management and driving among individuals with HIV: a 1-year follow-up study. J Clin Exp Neuropsychol 35:49–58. https://doi.org/10.1080/13803395.2012.747596
Tibuakuu M et al (2017) The association between cigarette smoking and inflammation: The Genetic Epidemiology Network of Arteriopathy (GENOA) study. PLoS One 12:e0184914. https://doi.org/10.1371/journal.pone.0184914
Torres OV, O’Dell LE (2016) Stress is a principal factor that promotes tobacco use in females. Prog Neuropsychopharmacol Biol Psychiatry 65:260–268. https://doi.org/10.1016/j.pnpbp.2015.04.005
Tsima B, Ratcliffe SJ, Schnoll R, Frank I, Kolson DL, Gross R (2018) Is Tobacco Use Associated with Neurocognitive Dysfunction in Individuals with HIV? J Int Assoc Provid AIDS Care 17:2325958218768018. https://doi.org/10.1177/2325958218768018
Tweed JO, Hsia SH, Lutfy K, Friedman TC (2012) The endocrine effects of nicotine and cigarette smoke. Trends Endocrinol Metab 23:334–342. https://doi.org/10.1016/j.tem.2012.03.006
USDHHS (2010) How Tobacco Smoke Causes Disease: The Biology and Behavioral Basis for Smoking-Attributable Disease: A Report of the Surgeon General. U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, Atlanta
Valette H et al (1999) Imaging central nicotinic acetylcholine receptors in baboons with [18F]fluoro-A-85380. J Nucl Med 40:1374–1380
Valiathan R, Miguez MJ, Patel B, Arheart KL, Asthana D (2014) Tobacco smoking increases immune activation and impairs T-cell function in HIV infected patients on antiretrovirals: a cross-sectional pilot study. PLoS One 9:e97698. https://doi.org/10.1371/journal.pone.0097698
Van de Wijer L et al (2019) Neuropsychiatric symptoms in Tanzanian HIV-infected children receiving long-term efavirenz treatment: a multicentre, cross-sectional, observational study. Lancet HIV 6:e250–e258. https://doi.org/10.1016/S2352-3018(18)30329-1
Van Keulen HV et al (2017) Serum levels of nitric oxide and cytokines in smokers at the beginning and after 4months of treatment for smoking cessatio. Int J Cardiol 230:327–331. https://doi.org/10.1016/j.ijcard.2016.12.111
Van Laecke S, Van Biesen W (2017) Smoking and chronic kidney disease: seeing the signs through the smoke? Nephrology Dialysis Transplantation 32:403–405. https://doi.org/10.1093/ndt/gfw448
Vassallo R, Tamada K, Lau JS, Kroening PR, Chen L (2005) Cigarette smoke extract suppresses human dendritic cell function leading to preferential induction of Th-2 priming. J Immunol 175:2684–2691. https://doi.org/10.4049/jimmunol.175.4.2684
Vassallo R, Kroening PR, Parambil J, Kita H (2008) Nicotine and oxidative cigarette smoke constituents induce immune-modulatory and pro-inflammatory dendritic cell responses. Mol Immunol 45:3321–3329. https://doi.org/10.1016/j.molimm.2008.04.014
Venneti S, Lopresti BJ, Wiley CA (2006) The peripheral benzodiazepine receptor (Translocator protein 18kDa) in microglia: from pathology to imaging. Prog Neurobiol 80:308–322. https://doi.org/10.1016/j.pneurobio.2006.10.002
Vera JH et al (2016) Neuroinflammation in treated HIV-positive individuals: A TSPO PET study. Neurology 86:1425–1432. https://doi.org/10.1212/WNL.0000000000002485
Vidrine DJ et al (2018) HIV Care Initiation: A Teachable Moment for Smoking Cessation? Nicotine Tob Res 20:1109–1116. https://doi.org/10.1093/ntr/ntx218
Walubo A (2007) The role of cytochrome P450 in antiretroviral drug interactions. Expert Opin Drug Metab Toxicol 3:583–598. https://doi.org/10.1517/17425225.3.4.583
Wang W, Li X, Xu J (2015) Exposure to cigarette smoke downregulates beta2-adrenergic receptor expression and upregulates inflammation in alveolar macrophages. Inhal Toxicol 27:488–494. https://doi.org/10.3109/08958378.2015.1075628
Wassenaar CA et al (2015) UGT1A and UGT2B genetic variation alters nicotine and nitrosamine glucuronidation in european and african american smokers. Cancer Epidemiol Biomarkers Prev 24:94–104. https://doi.org/10.1158/1055-9965.epi-14-0804
Wei P, Liu Q, Li D, Zheng Q, Zhou J, Li J (2015) Acute nicotine treatment attenuates lipopolysaccharide-induced cognitive dysfunction by increasing BDNF expression and inhibiting neuroinflammation in the rat hippocampus. Neurosci Lett 604:161–166. https://doi.org/10.1016/j.neulet.2015.08.008
Weinberger AH, Seng EK, Esan H, Shuter J (2018) Perceived risks and benefits of quitting smoking in a sample of adults living with HIV/AIDS AIDS Care 30:564–568. https://doi.org/10.1080/09540121.2017.1382678
Weiser M, Zarka S, Werbeloff N, Kravitz E, Lubin G (2010) Cognitive test scores in male adolescent cigarette smokers compared to non-smokers: a population-based study. Addiction 105:358–363. https://doi.org/10.1111/j.1360-0443.2009.02740.x
Whalen C, Horsburgh CR, Hom D, Lahart C, Simberkoff M, Ellner J (1995) Accelerated course of human immunodeficiency virus infection after tuberculosis. Am J Respir Crit Care Med 151:129–135. https://doi.org/10.1164/ajrccm.151.1.7812542
WHO (2019) Progress report on HIV, viral hepatitis and sexually transmitted infections. World Health Organization, Geneva
Wiley CA et al (2006) Positron emission tomography imaging of peripheral benzodiazepine receptor binding in human immunodeficiency virus-infected subjects with and without cognitive impairment. J Neurovirol 12:262–271. https://doi.org/10.1080/13550280600873868
Wittebole X, Hahm S, Coyle SM, Kumar A, Calvano SE, Lowry SF (2007) Nicotine exposure alters in vivo human responses to endotoxin. Clin Exp Immunol 147:28–34. https://doi.org/10.1111/j.1365-2249.2006.03248.x
Wojna V et al (2007) Associations of cigarette smoking with viral immune and cognitive function in human immunodeficiency virus-seropositive women. J Neurovirol 13:561–568. https://doi.org/10.1080/13550280701620747
Wong DF et al (2013) PET imaging of high-affinity alpha4beta2 nicotinic acetylcholine receptors in humans with 18F-AZAN, a radioligand with optimal brain kinetics. J Nucl Med 54:1308–1314. https://doi.org/10.2967/jnumed.112.108001
Woodcock EA, Hillmer AT, Mason GF, Cosgrove KP (2019) Imaging Biomarkers of the Neuroimmune System among Substance Use Disorders: A Systematic Review. Mol Neuropsychiatry 5:125–146. https://doi.org/10.1159/000499621
Woods SP et al (2004) Interrater reliability of clinical ratings and neurocognitive diagnoses in HIV. J Clin Exp Neuropsychol 26:759–778. https://doi.org/10.1080/13803390490509565
Yanagita M, Kobayashi R, Kojima Y, Mori K, Murakami S (2012) Nicotine modulates the immunological function of dendritic cells through peroxisome proliferator-activated receptor-gamma upregulation. Cell Immunol 274:26–33. https://doi.org/10.1016/j.cellimm.2012.02.007
Yang Z, Nesil T, Connaghan KP, Li MD, Chang SL (2016) Modulation Effect of HIV-1 Viral Proteins and Nicotine on Expression of the Immune-Related Genes in Brain of the HIV-1 Transgenic Rats. J Neuroimmune Pharmacol 11:562–571. https://doi.org/10.1007/s11481-016-9679-4
Yang Z, Nesil T, Wingo T, Chang SL, Li MD (2017) HIV-1 Proteins Influence Novelty-Seeking Behavior and Alter Region-Specific Transcriptional Responses to Chronic Nicotine Treatment in HIV-1Tg Rats. Nicotine Tob Res 19:1024–1032. https://doi.org/10.1093/ntr/ntx047
Yao Y, Hoffer A, Chang CY, Puga A (1995) Dioxin activates HIV-1 gene expression by an oxidative stress pathway requiring a functional cytochrome P450 CYP1A1 enzyme. Environ Health Perspect 103:366–371. https://doi.org/10.1289/ehp.95103366
Yek C et al (2016) Standard vaccines increase HIV-1 transcription during antiretroviral therapy. AIDS 30:2289–2298. https://doi.org/10.1097/QAD.0000000000001201
Yombi JC, Pozniak A, Boffito M, Jones R, Khoo S, Levy J, Post FA (2014) Antiretrovirals and the kidney in current clinical practice: renal pharmacokinetics, alterations of renal function and renal toxicity. AIDS 28:621–632. https://doi.org/10.1097/QAD.0000000000000103
Yoshikawa H et al. (2006) Nicotine inhibits the production of proinflammatory mediators in human monocytes by suppression of I-?B phosphorylation and nuclear factor-?B transcriptional activity through nicotinic acetylcholine receptor ?7 Clin Exp Immunol 146:116-123 doi:https://doi.org/10.1111/j.1365-2249.2006.03169.x
Yuan NY, Kaul M (2019) Beneficial and Adverse Effects of cART Affect Neurocognitive Function in HIV-1 Infection: Balancing Viral Suppression against Neuronal Stress and Injury. J Neuroimmune Pharmacol. https://doi.org/10.1007/s11481-019-09868-9
Zanger UM, Schwab M (2013) Cytochrome P450 enzymes in drug metabolism: regulation of gene expression, enzyme activities, and impact of genetic variation. Pharmacol Ther 138:103–141. https://doi.org/10.1016/j.pharmthera.2012.12.007
Zevin S, Benowitz NL (1999) Drug interactions with tobacco smoking. An update. Clin Pharmacokinet 36:425–438
Zhang B et al (2015) Alpha7 nicotinic acetylcholine receptor is required for blood-brain barrier injury-related CNS disorders caused by Cryptococcus neoformans and HIV-1 associated comorbidity factors. BMC Infect Dis 15:352. https://doi.org/10.1186/s12879-015-1075-9
Zhao L, Li F, Zhang Y, Elbourkadi N, Wang Z, Yu C, Taylor EW (2010) Mechanisms and genes involved in enhancement of HIV infectivity by tobacco smoke. Toxicology 278:242–248. https://doi.org/10.1016/j.tox.2010.09.010
Zhu AZ, Zhou Q, Cox LS, Ahluwalia JS, Benowitz NL, Tyndale RF (2013) Variation in trans-3’-hydroxycotinine glucuronidation does not alter the nicotine metabolite ratio or nicotine intake. PLoS One 8:e70938. https://doi.org/10.1371/journal.pone.0070938
Zhu X, Han Y, Du J, Liu R, Jin K, Yi W (2017) Microbiota-gut-brain axis and the central nervous system. Oncotarget 8:53829–53838. https://doi.org/10.18632/oncotarget.17754
Zhu J et al (2018) CYP1A1 and 1B1-mediated metabolic pathways of dolutegravir, an HIV integrase inhibitor. Biochem Pharmacol 158:174–184. https://doi.org/10.1016/j.bcp.2018.10.012
Ziedonis D et al (2008) Tobacco use and cessation in psychiatric disorders: National Institute of Mental Health report. Nicotine Tob Res 10:1691–1715. https://doi.org/10.1080/14622200802443569
Funding
This research was supported by grants from the National Institutes of Health (K24 DA045244; R01 DA042682; R01 DA044906) and through core services and support from the Penn Center for AIDS Research (P30 AI045008) and the Penn Mental Health AIDS Research Center (P30 MH097488).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of Interest
Dr. Schnoll receives medication and placebo free of charge from Pfizer for clinical trials and has provided consultation to Pfizer, GlaxoSmithKline, and Curaleaf. Dr. Gross serves on a Pfizer Data and Safety Monitoring Board for a drug unrelated to smoking or HIV. Dr. Ashare has an investigator-initiated grant from Novo Nordisk for a drug unrelated to the current paper.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Ghura, S., Gross, R., Jordan-Sciutto, K. et al. Bidirectional Associations among Nicotine and Tobacco Smoke, NeuroHIV, and Antiretroviral Therapy. J Neuroimmune Pharmacol 15, 694–714 (2020). https://doi.org/10.1007/s11481-019-09897-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11481-019-09897-4