
Abstract
Purpose
The purpose of this study was to investigate the reporting habits of clinicians who have been exposed to disruptive behaviour in the operating room (OR) and assess their satisfaction with management’s responses to this issue.
Methods
Ethics committee approval was obtained. This was a pre-specified sub-study of a larger survey examining disruptive behaviour, which was distributed to OR clinicians in seven countries. Using Likert-style questions, this study ascertained the proportion of disruptive intraoperative behaviour that clinicians reported to management, as well as their degree of satisfaction with management’s responses. Binomial logistic regression identified socio-demographic, exposure-related, and behavioural predictors that a clinician would never report disruptive behaviour.
Results
Four thousand, seven hundred and seventy-five respondents were part of the sub-study. Disruptive behaviour was under-reported by 96.5% (95% confidence interval [CI], 95.9 to 97.0) of respondents, and never reported by 30.9% (95% CI, 29.6 to 32.2) of respondents. Only 21.0% (95% CI, 19.8 to 22.2) of respondents expressed satisfaction with management’s responses. Numerous socio-demographic, exposure-related, and behavioural predictors of reporting habits were identified. Socio-demographic groups who had higher odds of never reporting disruptive behaviour included younger clinicians, clinicians without management responsibilities, both anesthesiologists and surgeons (compared with nurses), biological females, and heterosexuals (all P < 0.05).
Conclusions
Disruptive behaviour was under-reported by nearly all clinicians surveyed, and only one in five were satisfied with management’s responses. For healthcare systems to meaningfully address the issue of disruptive behaviour, management must create reporting systems that clinicians will use. They must also respond in ways that clinicians can rely on to affect necessary change.
Résumé
Objectif
L’objectif de cette étude était d’examiner les pratiques de signalements des cliniciens exposés à des comportements perturbateurs en salle d’opération (SOP) et d’évaluer leur satisfaction vis-à-vis des réactions de la direction à ce problème.
Méthode
Nous avons obtenu le consentement du comité d’éthique. Il s’agissait d’une sous-étude pré-spécifiée d’un plus grand sondage portant sur les comportements perturbateurs, distribué aux cliniciens de SOP dans sept pays. À l’aide de questions de style Likert, cette étude a déterminé la proportion de comportements perturbateurs peropératoires rapportés par les cliniciens à la direction, ainsi que leur degré de satisfaction vis-à-vis de la réponse de la direction. Une régression logistique binomiale a permis d’identifier les prédicteurs sociodémographiques, ainsi que les prédicteurs liés à l’exposition et comportementaux indiquant qu’un clinicien ne rapporterait jamais un comportement perturbateur.
Résultats
Quatre mille sept cent soixante-quinze répondants ont été inclus dans cette sous-étude. Les comportements perturbateurs étaient sous-rapportés par 96,5 % (intervalle de confiance [IC] 95 %, 95,9 à 97,0) des répondants, et jamais rapportés par 30,9 % (IC 95 %, 29,6 à 32,2) des répondants. Seuls 21,0 % (IC 95 %, 19,8 à 22,2) des répondants ont exprimé être satisfaits des réactions de la direction. De nombreux prédicteurs sociodémographiques, liés à l’exposition et comportementaux des habitudes de communication ont été identifiés. Les groupes sociodémographiques affichant une probabilité plus élevée de ne jamais rapporter les comportements perturbateurs comprenaient les cliniciens plus jeunes, les cliniciens sans responsabilités de direction, les anesthésiologistes et les chirurgiens (par rapport au personnel infirmier), les femmes biologiques et les hétérosexuels (tous P < 0,05).
Conclusion
Les comportements perturbateurs étaient sous-rapportés par la quasi-totalité des cliniciens interrogés, et seul un clinicien sur cinq s’estimait satisfait des réponses de la direction. Si les systèmes de soins de santé veulent véritablement régler le problème des comportements perturbateurs, les directions des établissements doivent créer des systèmes de communication des incidents qui seront utilisés par les cliniciens. Elles doivent également réagir de manière à ce que les cliniciens puissent avoir confiance que les changements nécessaires seront apportés.
Similar content being viewed by others


Disruptive behaviour can be defined as any interpersonal behaviour that results in a perceived threat to victims or witnesses and violates a reasonable person’s standard of respectful behaviour.1,2 This behaviour is prevalent in the healthcare setting,3,4 including the operating room (OR).2 It can negatively affect clinician well-being,5,6,7 undermine patient care,1,8,9,10,11,12,13 and inhibit effective resource management.5,14,15,16,17,18 The Joint Commission issued a sentinel alert in 2008 about disruptive behaviour,19 and pre-eminent medical associations have developed position statements addressing the issue.20,21
To prevent recurrence and to effectively deal with disruptive clinicians, management must respond promptly and decisively. Nevertheless, management’s ability to respond is limited by the willingness of clinicians to report events. It is therefore essential to identify predictors that a clinician will not report disruptive behaviour. In addition, ensuring that clinicians are satisfied with the ways in which management responds is also important. Satisfaction with management’s responses to disruptive behaviour contributes to overall job satisfaction, which is associated with decreased staff turnover, decreased absenteeism, increased productivity, and increased job commitment.
Previous studies have identified that clinicians under-report disruptive behaviour in some healthcare settings.22,23,24,25,26,27,28 In addition, there is some evidence that clinicians are not satisfied with how management deals with these incidents.22,29,30 Nevertheless, these studies have not specifically examined how often disruptive intraoperative behavior is reported to management, nor the satisfaction of OR clinicians to management’s responses. In addition, no quantitative models have identified predictors that a clinician would never report disruptive behaviour.
The primary purposes of this study were to quantify the proportion of clinicians who under-report disruptive behaviour, as well as the proportion who never report disruptive behaviour. The secondary purposes were to identify predictors that a clinician would never report disruptive behaviour, and to quantify clinician satisfaction with management’s responses to the issue.
Methods
Design and sampling
This was a pre-specified sub-study of a larger survey examining exposure and behavioural responses to disruptive behaviour.4 The full details of the sampling frame and survey distribution have been described elsewhere.4 In brief, 23 perioperative organizations in seven countries distributed a survey to their members. The sampling frame included anesthesiologists, nurses (including nurse anesthetists), surgeons, operative technicians, and senior medical students. Several measures were taken to maximize the response rate. We acquired the support of perioperative associations and had them send the survey to their membership on our behalf. We also had the associations send out a reminder to complete the survey one week after the initial distribution. Where possible, we also had the associations send the membership advance notice that the survey would be sent out.
Measurement
Clinicians in this sub-study answered Likert-style questions regarding the proportion of disruptive behaviour that they reported to management and how satisfied they were with management’s responses (Fig. 1). Broad socio-demographic information was collected about all respondents. In addition, exposure and responses to disruptive behaviour were measured using two previously developed scales.31 Five forms of exposure were measured, including behaviour directed toward the respondent (personal), toward colleagues within the respondent’s profession (in-group), toward others in the OR (outgroup), toward patients, and toward no one in particular (undirected). Four behavioural response strategies that a clinician could adopt when confronted with disruptive behaviour were measured (passive, assertive, manipulative, and malicious).

Survey questions assessing the reporting of disruptive behaviour and satisfaction with management’s response
Statistical analysis
A modified wave analysis was performed to identify potential non-response bias (which could inflate or artificially decrease the prevalence estimates).32 The wave analysis involved using two separate Kruskal–Wallis tests to evaluate whether the average time to respond varied between individuals with different reporting habits or satisfaction levels. Post hoc Mann–Whitney U tests were then used to identify pairwise differences among the groups for the satisfaction outcome. The wave analysis placed all respondents and non-respondents on a continuum based on their motivation to complete the survey. Early responders were assumed to be the most motivated, those with longer response times less motivated, and non-respondents the least motivated.33 While the outcome measures of non-respondents are unknown, inferences can be made about them based on differences in response time between groups with different reporting habits and levels of satisfaction. These inferences include the prospect of there being non-response bias based on the outcome measures.33 For example, if individuals with better reporting habits took longer to respond, this would provide evidence that participants with good reporting were less likely to complete the survey. Because of underpopulated categories in the reporting outcome and a lack of proportional odds, the reporting variable was reduced to a binary variable (0%, > 0%).
Binomial logistic regression was used to identify factors predicting the likelihood that a clinician would report 0% of the disruptive behaviour they were exposed to, i.e., would never report. A binary model was used for the aforementioned reasons. Candidate predictors fell into three broad categories: respondent socio-demographics, the five types of exposure to disruptive behaviour, and the four behavioural responses to disruptive behaviour. Confidence intervals were calculated using the Clopper–Pearson method. The model included any respondents who indicated being exposed to disruptive behaviour and answered the question regarding reporting.
Results
Response rate
It was calculated that the survey was distributed to at least 101,624 clinicians, of whom 7,465 responded. 4,775 provided answers to at least one of the questions assessing reporting or satisfaction (response rate of 4.7%). Seventy respondents provided answers for the reporting and satisfaction questions but reported no exposure to the 14 examples of disruptive behaviour. To avoid including respondents who justifiably did not report incidents to management (given that they had nothing to report), these 70 individuals were excluded from the analysis. The respondent socio-demographics, exposure, and responses are summarized in Table 1 (A and B). The amount of missing data was small, with the number of clinicians who had missing data being 1.59%, and the number of cells with missing data being 0.08%. Based on this, pairwise deletion of missing data was used.
Wave analysis
There were no statistically significant differences in the time to respond to the survey between clinicians who never reported and clinicians who reported some amount of disruptive behaviour (χ2 = 0.108, P = 0.742). In addition, there was no significant difference in response time between the five satisfaction groups (χ2 = 8.15, P = 0.086).
Reporting
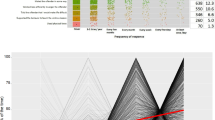
The percentage of respondents reporting different amounts of disruptive behaviour is shown in Fig. 2A. Of note, 96.5% (95% confidence interval [CI], 95.9 to 97.0) of respondents under-reported disruptive behaviour. The distribution was skewed toward substantial under-reporting, with 73.9% (95% CI, 72.6 to 75.1) of clinicians indicating they had reported less than 1/5 of the disruptive behaviour they were exposed to and 30.9% (95% CI, 29.6 to 32.2) indicating that they had never reported.

This combined violin and dot plot shows the distribution of responses to the question assessing reporting to management (panel A) and satisfaction with management’s responses (panel B). The width of the violin figure at each response category represents the probability density of that response. For clarity, the proportion of clinicians endorsing each response category is included. The underlying dot plot shows the raw data with vertical and horizontal jitter added for clarity
Socio-demographic predictors of non-reporting
The results of the binomial logistic regression model are shown in Table 2. After controlling for country, we found that age, management responsibility, profession, sex, and sexual orientation all predicted reporting habits. Because of the need to combine several response options to the reporting question into a single category (> 0%), the model was unable to predict the amount of disruptive behaviour that a clinician would report; however, the model was able to predict the odds that a clinician would never report disruptive behaviour. Socio-demographic groups who had higher odds of never reporting disruptive behaviour included younger clinicians, clinicians without management responsibilities, both anesthesiologists and surgeons (compared with nurses), biological females, and heterosexuals (all P < 0.05, Table 2). Increasing amounts of exposure to personal, in-group, outgroup, and undirected forms of disruptive behaviour predicted lower odds that a clinician would never report (all P < 0.05, Table 2). Nevertheless, a greater exposure to disruptive behaviour that is directed toward patients did not affect the odds that a clinician would never report (P = 0.56). The general response strategy that clinicians used when dealing with disruptive behaviour also predicted the odds of never reporting. Specifically, clinicians who more frequently adopt a passive response strategy to disruptive behaviour were more likely to never report (P < 0.001) while those who more frequently adopt an assertive response strategy were less likely to never report (P < 0.001). In contrast, the odds of never reporting were unaffected by how often clinicians responded using either a manipulative (P = 0.42) or malicious response strategy (P = 0.81).
Satisfaction
Clinician satisfaction with management’s responses to disruptive behaviour is shown in Fig. 2B. Only 21.0% (95% CI, 19.8 to 22.2) of clinicians expressed some degree of satisfaction (either satisfied or very satisfied).
Discussion
This survey of OR clinicians shows that nearly all the respondents under-report disruptive behaviour to management, and more than 30% never report. After controlling for country of work, certain socio-demographic groups were more likely to never report. These included younger clinicians, those not in management positions, anesthesiologists and surgeons (compared with nurses), females, and heterosexuals. Of additional concern is that only one in five clinicians were unequivocally satisfied with management’s responses to disruptive behaviour.
When interpreting the amount of disruptive behaviour reported, it is important to distinguish between collective and individual under-reporting. Collective under-reporting refers to the proportion of disruptive events that are not reported by anyone, while individual under-reporting refers to the proportion of disruptive events that a given clinician does not report. While individual under-reporting does not always lead to collective under-reporting, it is associated with undesirable outcomes under all circumstances. At one extreme, under-reporting by individual clinicians could result in a large collective under-reporting. This can hinder management’s ability to address disruptive behaviour, can normalize the behaviour, and can lead to more instances of disruptive behaviour. At the other extreme, at least one victim/witness could report each incident of disruptive behaviour, resulting in no collective under-reporting. Nevertheless, increased individual reporting provides benefits independent of its effect on collective reporting. In this regard, having multiple reports of a single incident provides additional context and information to help managers validate and clarify initial reports. Multiple reports can also galvanize managers to act and can potentially escalate the reports to multiple managerial channels.
The reasons that some socio-demographic groups are more likely to never report is unclear and should be further investigated. While we have identified the socio-demographic predictors of reporting independent of the frequency of exposure to five types of disruptive behaviour, this does not control for differences in the severity of the behaviours experienced. These socio-demographic groups may also differ in their subjective perceptions of how important it is to report the behaviour. In other instances, poor reporting habits may reflect the group’s perceived or actual lack of power to report incidents without repercussions. Clinicians with greater exposure to disruptive behaviour were less likely to never report. Nevertheless, when faced with increasing verbal mistreatment of patients, the odds that a clinician would never report remained unchanged. Thus, increasing mistreatment of patients does not appear to motivate clinicians to start reporting. The odds that a clinician would never report were not significantly affected by their institutions’ type of funding (non-profit or privately funded). Similarly, whether a clinician was or was not a visible minority did not predict non-reporting.
The low rate of clinician satisfaction with management’s responses to disruptive behaviour may be the result of several factors. Dissatisfaction may occur when management does not respond to a reported incident in a manner that clinicians think is adequate, does not respond at all, or responds but does not debrief staff about remediating or punitive actions. Being satisfied with management’s responses to disruptive behaviour is essential to maintain overall career satisfaction. This in turn is associated with decreased staff turnover, decreased absenteeism, increased productivity, and increased career commitment.
This study provides important information to OR managers. Clinicians are both under-reporting disruptive behaviour and are dissatisfied with management’s responses. Consequently, management should take additional steps to address both reporting and satisfaction. To ensure that individual clinicians increase their reporting, managers should educate clinicians on the consequences of disruptive behaviour and emphasize that reporting is essential to managing and preventing it. Management should also make special efforts to encourage reporting from clinicians who never report. A change in the behaviour of these clinicians would maximize increases to both individual and collective reporting and would ensure that reports represent the experience of all OR clinicians. To increase satisfaction, institutions should seek the input of clinicians while creating policies and procedures that address disruptive behaviour. Management must then consistently implement these policies without unjust leniency based on the stature or income generation of the clinician who is acting disruptively.
Our study has several limitations. Both the survey distribution rate and survey response rate were low. The low distribution rate may indicate a hesitance for perioperative associations to examine these sensitive issues. A low response rate increases concerns regarding the generalizability of the results to the broader population of clinicians because of the large potential for non-response bias. Nevertheless, the wave analysis indicated that there is no significant relationship between the time to respond to the survey and either reporting habits or satisfaction. Furthermore, even if we recruited an additional 4,766 participants (thereby doubling the sample size for the reporting outcome) and we observed the unlikely result that all of the additional respondents had perfect reporting habits, this would still result in under-reporting from 48.5% of respondents, and complete non-reporting from 15.5% of respondents. In this case, under-reporting and non-reporting would remain concerns. Thus, an extremely large non-response bias would need to be present for the prevalence estimates to decrease below levels that merit concern. It is also important to note that the absolute number of clinicians who under-report disruptive behaviour is concerning, regardless of the proportion of clinicians that this represents. In addition, the identification of predictors that a clinician would never report disruptive behaviour is less affected by response rate than it is by having an adequate spread of predictor and outcome values. In characterizing relationships between variables, sample representativeness is less critical than recruiting an adequate number of respondents with different predictor values and outcomes.34 A second limitation is that the assessment scale for satisfaction included a neutral response category. Neutral responses can be difficult to interpret, as this option can be endorsed by a range of individuals, including those who hold a truly neutral viewpoint, those who have insufficient knowledge to answer the question (e.g., those who are unaware how management responded), and those who have insufficient motivation to respond (e.g., those who don’t care how management responded—perhaps because they see the issue as being trivial).35 Nevertheless, this ambiguity would likely be compounded if the neutral category were removed, as this would force these groups to “feign” some degree of satisfaction or dissatisfaction.35 The other alternative would be to parse out these various options, which would deviate from the Likert scale format and likely create response categories that were poorly populated. It would also increase the time to respond to each question and therefore increase the risk of respondent attrition. Thus, the inclusion of a “neutral” category was the best option.
Despite these limitations, this study provides strong evidence that disruptive behaviour in the OR is under-reported and that clinicians are not satisfied with management’s responses. The large sample size (n = 4,775) increases the generalizability of our results and provides more precise estimates. The distribution of the survey across seven countries also increases the generalizability of these results. Distribution of the survey to all operative professions as well as students working in the OR ensures that the survey targeted all possible reporters of disruptive intraoperative behaviour and thereby better establishes the scope of the problem.
Conclusions
Disruptive behaviour in the OR is under-reported, and OR clinicians are not satisfied with the way management responds to incidents. Future research should identify the amount of collective under-reporting by comparing the number of disruptive events directly observed by researchers with the number subsequently reported to management. In addition, the reasons for these low levels of reporting and satisfaction should be identified. By establishing the scope of the problem in the operative context, we show that there is a need for managers and healthcare leaders to act. Adequate reporting is both critical and necessary in preventing the re-occurrence of disruptive behaviour, and in turn, safeguarding the well-being of both clinicians and patients.
References
Villafranca A, Hamlin C, Enns S, Jacobsohn E. Disruptive behaviour in the perioperative setting: a contemporary review. Can J Anesth 2017; 64: 128-40.
Villafranca A, Fast I, Jacobsohn E. Disruptive behavior in the operating room: prevalence, consequences, prevention, and management. Curr Opin Anaesthesiol 2018; 31: 366-74.
Rosenstein AH, O’Daniel M. Impact and implications of disruptive behavior in the perioperative arena. J Am Coll Surg 2006; 203: 96-105.
Villafranca A, Hiebert B, Hamlin C, et al. Prevalence and predictors of exposure to disruptive behaviour in the operating room. Can J Anesth 2019; 66: 781-94.
Pfifferling JH. The disruptive physician. A quality of professional life factor. Physician Exec 1999; 25: 56-61.
Laschinger H, Grau AL, Finegan J, Wilk P. New graduate nurses’ experiences of bullying and burnout in hospital settings. J Adv Nurs 2010; 66: 2732-42.
Quine L. Workplace bullying in nurses. J Heal Psychol 2001; 6: 73-84.
The Joint Commission. Summary Data of Sentinel Events Reviewed by The Joint Commission. 2012. Available from URL: https://www.jointcommission.org/assets/1/18/2004_4Q_2012_SE_Stats_Summary.pdf (accessed August 2019)”
The Joint Commission. Sentinel Event Statistics Released for 2014. Available from URL: https://www.jointcommission.org/issues/article.aspx?Article=jjLkoItVZhkxEyGe4AT5NDyAZaTPkWXc50Ic3pERKGw%3D (accessed August 2019).
Mazzocco K, Petitti DB, Fong KT, et al. Surgical team behaviors and patient outcomes. Am J Surg 2009; 197: 678-85.
Schaeffer MH. Environmental stress and individual decision-making: implications for the patient. Patient Educ Couns 1989; 13: 221-35.
Arora S, Sevdalis N, Nestel D, Woloshynowych M, Darzi A, Kneebone R. The impact of stress on surgical performance: a systematic review of the literature. Surgery 2010; 147(318–30): e6.
O’Daniel M, Rosenstein AH. Disruptive behavior and clinical outcomes: perceptions of nurses and physicians. Am J Nurs 2005; 105: 54-64.
Pfifferling JH. Managing the unmanageable: the disruptive physician. Fam Pract Manag 1997; 4: 76-78, 83, 87-92.
Berry PA, Gillespie GL, Gates D, Schafer Jl. Novice nurse productivity following workplace bullying. J Nurs Scholarsh 2012; 44: 80-7.
Hogh A, Hoel H, Carneiro IG. Bullying and employee turnover among healthcare workers: a three-wave prospective study. J Nurs Manag 2011; 19: 742-51.
Klaassen M, Kleiner B. New developments concerning negligent retention. Managerial Law 2001; 43: 62-8.
Rao MB, Rao MM. Trust betrayed - depraved doctor or negligent hospital? IUP J Manag Res 2016; XV: 53-72.
The Joint Commission. Behaviours That Undermine A Culture of Safety. Sentinel Event Alert 2008. Available from URL: https://www.jointcommission.org/sentinel_event_alert_issue_40_behaviors_that_undermine_a_culture_of_safety/ (accessed August 2019).
Institute for Healthcare Improvement. Lucian Leape Institute. Through the Eyes of the Workforce: creating joy, meaning, and safer health care. Boston, MA: National Patient Safety Foundation; 2013.
AORN. AORN Position Statement on a Healthy Perioperative Practice Environment 2015; 1-5. Available from URL: https://www.aorn.org/-/media/aorn/guidelines/position-statements/posstat-safety-healthy-practice.pdf (accessed August 2019).
Maddineshat M, Rosenstein AH, Akaberi A, Tabatabaeichehr M. Disruptive behaviours in an emergency department: the perspective of physicians and nurses. J Caring Sci 2016; 5: 241-9.
Swafford L. Lateral Violence in the Emergency Department. Hunt School of Nursing. Nursing Theses and Capstone Projects 2014. Available from URL: https://pdfs.semanticscholar.org/1867/b28ed05c8ab8effaa70827136043a2cebeb9.pdf (accessed August 2019).
Maddineshat M, Hashemi M, Tabatabaeichehr M. Evaluation of the disruptive behaviours among treatment teams and its reflection on the therapy process of patients in the operating room: the impact of personal conflicts. J Educ Health Promot 2017. https://doi.org/10.4103/jehp.jehp_47_16.
Walrath JM, Dang D, Nyberg D. An organizational assessment of disruptive clinician behavior findings and implications. J Nurs Care Qual 2013; 28: 110-21.
Smith J. Bullying in the Nursing Workplace: a Study of Perioperative Nurses. 2011. Available from URL: https://pqdtopen.proquest.com/doc/907103858.html?FMT=ABS (accessed August 2019).
Vessey JA, Demarco RF, Gaffney D, et al. Bullying of staff registered nurses in the workplace: a preliminary study for developing personal and organizational strategies for the transformation of hostile to healthy workplace environments. J Prof Nurs 2009; 25: 299-306.
Rosenstein AH. Physician disruptive behaviors: five year progress report. World J Clin Cases 2015; 3: 930-4.
Institute for Safe Medical Practices. Intimidation: Mapping a Plan for Cultural Change in Healthcare (Part II). 2004. Available from URL: https://www.ismp.org/resources/intimidation-mapping-plan-cultural-change-healthcare-part-ii (accessed August 2019).
Institute for Safe Medical Practices. Intimidation: Practitioners Speak Up About This Unresolved Problem (Part I). 2004. Available from URL: https://www.ismp.org/resources/intimidation-practitioners-speak-about-unresolved-problem-part-i (accessed August 2019).
Villafranca A, Hamlin C, Rodebaugh TL, Robinson S, Jacobsohn E. Development of survey scales for measuring exposure and behavioral responses to disruptive intraoperative behavior. J Patient Saf 2017. https://doi.org/10.1097/PTS.0000000000000423.
Lin IF, Schaeffer NC. Using survey participants to estimate the impact of nonparticipation. Public Opin Q 1995; 59: 236-58.
Lewis EF, Hardy M, Snaith B. Estimating the effect of nonresponse bias in a survey of hospital organizations. Eval Health Prof 2013; 36: 330-51.
Chandler J, Shapiro D. Conducting clinical research using crowdsourced convenience samples. Annu Rev Clin Psychol 2016; 12: 53-81.
Friedman HH, Amoo T. Rating the rating scales. J Mark Manag 1999; 9: 114-23.
Author contributions
Ian Fast contributed to all aspects of this study, including conception and design of the study; analysis and interpretation of the data, and drafting of the manuscript. Alexander Villafranca contributed to all aspects of this study, including conception and design of the study; acquisition, analysis, and interpretation of the data, and drafting of the manuscript. Bernadette Henrichs contributed to the conception and design of the study, acquisition of the data, and editing of the manuscript. Kirby Magid contributed to the interpretation of the data, data analysis, and drafting of the manuscript. Chris Christodoulou and Eric Jacobsohn contributed to the conception and design of the study, interpretation of the data, and drafting of the manuscript.
Acknowledgements
We would like to thank the Academic Oversight Committee of the Department of Anesthesia, Perioperative and Pain Medicine at the University of Manitoba (Winnipeg, MB, Canada) for providing financial support of this project. We also appreciate the help of the 23 organizations who distributed the survey and the time and effort of all respondents.
Conflicts of interest
None.
Funding statement
The Academic Oversight Committee of the Department of Anesthesia, Perioperative and Pain Medicine at the University of Manitoba (Winnipeg, MB, Canada), Max Rady College of Medicine provided financial support for this project.
Editorial responsibility
This submission was handled by Dr. Philip M. Jones, Associate Editor, Canadian Journal of Anesthesia.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is accompanied by an editorial. Please see Can J Anesth 2020; 67: this issue.
Rights and permissions
About this article

Cite this article
Fast, I., Villafranca, A., Henrichs, B. et al. Disruptive behaviour in the operating room is under-reported: an international survey. Can J Anesth/J Can Anesth 67, 177–185 (2020). https://doi.org/10.1007/s12630-019-01540-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12630-019-01540-3