
Abstract
Purpose
We sought to validate a French translation of the Iowa Satisfaction with Anesthesia Scale (ISAS), a tool to assess the patient’s satisfaction with monitored anesthesia care for surgery. The ISAS tool is particularly pertinent as surgery with monitored anesthesia care is increasingly used in ambulatory surgery settings.
Methods
We studied content validity, internal consistency, convergent validity (vs physician-estimated satisfaction), and test-retest reliability of the French version of the ISAS (ISAS-F) in 122 adult patients undergoing a brief outpatient invasive procedure under conscious sedation. The ISAS-F was answered twice by the patient, once in the postanesthesia care unit and once before discharge from the ambulatory care unit.
Results
The median [interquartile range (IQR)] time of completion at the first assessment was 2 [2–4] min. The total median [IQR] ISAS-F score was 2.3 [1.8–2.7]. Internal consistency of the ISAS-F was found to be good (Cronbach’s α = 0.68). Test-retest reliability was significant, with an intra-class correlation coefficient at 0.74 (95% confidence interval [CI], 0.63 to 0.85). The ISAS-F score correlated with the physician-estimated satisfaction score, with an intra-class correlation coefficient of 0.28 (95% CI, 0.12 to 0.44; P = 0.01).
Discussion
This validated version of the ISAS can now be used by French-speaking researchers and physicians to assess patient satisfaction with the anesthesia technique.
Résumé
Objectif
Nous avons voulu valider une traduction française de l’échelle de satisfaction par rapport à l’anesthésie de l’Iowa (ISAS), un outil d’évaluation de la satisfaction du patient par rapport aux soins sous surveillance anesthésique lors de chirurgies. L’outil ISAS est particulièrement pertinent étant donné que les chirurgies réalisées sous surveillance anesthésique sont de plus en plus fréquemment utilisées dans le contexte de chirurgie ambulatoire.
Méthode
Nous avons étudié la validité de contenu, la cohérence interne, la validité convergente (vs la satisfaction estimée par le médecin) et la fiabilité de test-retest de la version française de l’ISAS (ISAS-F) auprès de 122 patients adultes subissant une courte intervention ambulatoire sous sédation légère. Les patients ont répondu deux fois au ISAS-F, soit une fois en salle de réveil et une seconde fois avant de recevoir leur congé de l’unité de soins ambulatoires.
Résultats
Le temps médian [écart interquartile (ÉIQ)] pour compléter le test lors de la première évaluation était de 2 [2–4] min. Le score total médian [ÉIQ] sur l’ISAS-F était de 2,3 [1,8–2,7]. La cohérence interne de l’ISAS-F était bonne (α de Cronbach = 0,68). La fiabilité de test-retest était appréciable, avec un coefficient de corrélation intraclasse de 0,74 (intervalle de confiance [IC] 95 %, 0,63 à 0,85). Le score sur l’ISAS-F était corrélé au score de satisfaction tel qu’estimé par le médecin, avec un coefficient de corrélation intraclasse de 0,28 (IC 95 %, 0,12 à 0,44; P = 0,01).
Discussion
Cette version validée de l’ISAS peut désormais être utilisée par les chercheurs et médecins francophones afin d’évaluer la satisfaction des patients avec la technique anesthésique employée.
Similar content being viewed by others

Monitored anesthesia care consists of conscious (and usually intravenous) sedation in which the level of consciousness is maintained enough to allow the patient to communicate and react to unexpected sensations. It can be associated with systemic analgesia or locoregional anesthesia. It is increasingly being used in outpatient procedures that are especially painful or anxiety-provoking, such as dental extractions, radio-interventional surgery, or cutaneous surgery. According to the World Health Organization (WHO), patient satisfaction is a main point of the patient-centred pattern of care, and for this purpose, an English-language version of the Iowa Satisfaction with Anesthesia Scale (ISAS) was developed.1 The ISAS is a self-administered questionnaire with 11 simple items corresponding alternatively to negative or positive feelings, to avoid acquiescence bias.2 For each item, the offered answer is a Likert-like six-point nominal scale, and each response is given as a satisfaction score ranging from − 3 to 3. The total satisfaction score is the unweighted average of these 11 scores, so its expected range is also − 3 to 3. Since then, the ISAS has been used in systematic reviews.3,4,5 It is the only validated score to assess patient satisfaction after conscious intravenous sedation for surgery,5,6 and its sensitivity to change has been used in a clinical trial of dexmedetomidine.7
Validated Spanish and Polish versions are available,8,9 and although a French version has been tested for ocular surgery,10,11 this was only a simple direct translation and did not follow the recommended processes of a transcultural validation (see Methods) as recommended by the United States Food and Drug Administration12 and the WHO.13 The aim of this study was to validate a French version of the ISAS by analyzing construct validity, internal consistency, convergent validity, and test-retest reliability, in a sample of patients undergoing scheduled brief surgical procedures needing conscious sedation.
Methods
According to French law, legal authorizations were not required for this study as it was research in social sciences as well as a satisfaction survey. Ethical approval was given by the Research Ethics Committee of the French Society of Anaesthesia and Intensive Care (Comité d’Éthique pour la Recherche en Anesthésie et Réanimation, IRB 00010254-2018-052) on 1 April 2018. All participants gave their informed consent to participate.
The study plan was in accordance with the recommendations for transcultural validation.14,15,16 The involvement of several people with various backgrounds helped build a tool that people could commonly understand by preventing individual subjectivity. The tool should not only be written in the native language of the target population but also consider the culture of the target population (e.g., habits, beliefs, and interpretations). The initial forward translation must be done at least by two independent bilingual translators whose mother tongue is the target language, and at least one should be naive of the tool’s structure and aims. Discrepancies between versions should be corrected in a comprehensive synthesis. Back-translation is mandatory to check conformity with the original version; this must be done by two persons whose mother tongue is the source language, and both must be unaware of the concepts explored.
The study took place in the department of perioperative medicine of the University Hospital of Clermont-Ferrand. The inclusion criteria were patients aged 18–70 yr; currently understanding, speaking, and reading French; scheduled for an ambulatory invasive procedure (radio-interventional or maxillofacial surgery) under conscious sedation; and able to give informed consent. Conscious sedation was justified by the noxious but short-lasting aspect of the procedure (e.g., because of the small incision, deep needle puncture, or tissue dissection). We aimed at a balanced recruitment between radio-interventional and maxillofacial procedures.
All eligible consecutive patients were approached to participate throughout the study period. The patients’ demographic and morphometric data were collected. When arriving into the operating room, the patient’s signed consent was checked by the anesthetist in charge. Conscious sedation was conducted following a protocol chosen at the physician’s preference. Depending on the procedure, local anesthesia was also performed as indicated. At the end of the procedure, the physician in charge answered a questionnaire that had the same structure as the ISAS-F, except that the presentation and items were adapted in such a way that the physician was asked to imagine he/she answered for the patient. The patient was asked to answer the ISAS-F in the postanesthesia care unit, at least 15 min after the beginning of a phase defined by the absence of any abnormal vital signs, and when fully conscious, defined as a score of 5 on the Observer’s Assessment of Alertness/Sedation Scale.17 A second self-assessment was done by the patient before discharge from the ambulatory unit (about three hours after the first assessment). This second assessment (i.e., retest) was done only by one half of the original patient sample, while the other half responded to a short questionnaire to give their appreciation of the questionnaire itself (i.e., the readability, support for writing, time allowed to answer, understandability of the questions, space to express free comments, and appropriateness for assessing their satisfaction). The other perioperative data were reported on a standardized case report form.
The primary outcome was the psychometric properties of the ISAS-F, including its construct validity, internal consistency, test-retest reliability, and convergent validity. For this last point, a questionnaire using the same items as the ISAS-F was dedicated to the physician’s assessment, and was completed independently from the patient’s one. The total ISAS-F score was calculated according to the same rules as for the original version—i.e., by averaging each of the 11 subscores.
Statistical analyses
Qualitative data have been expressed as the number of cases and percentage (%). Quantitative data have been expressed as mean (standard deviation [SD]) in case of a Gaussian distribution, and median [interquartile range (IQR)] otherwise. The level of significance was set at 5%. Acceptability of the ISAS-F has been assessed by 1) the completion rate for each item (with a target set at 85%), 2) the responses the patients gave regarding their appreciation of the ISAS-F, and 3) the time needed to complete the questionnaire. The ability of the ISAS-F to discriminate was assessed by checking a floor and ceiling effect for the whole score. Internal consistency was assessed by the Cronbach’s α coefficient. Construct validity was assessed by between-items correlation matrix. Between-items correlations were assessed by Pearson’s or Spearman’s correlation coefficients, depending on the distribution. Test-retest reliability was assessed by intra-class correlation coefficients and a Bland and Altman plot. Convergent validity (patient- vs physician-assessed) was assessed by the intra-class correlation coefficient.
The required sample size was estimated at 120 subjects, in accordance with the current recommendations for such validation studies,18 and as was used for the validation of the Spanish version.8 This was considered sufficient to detect correlation coefficients superior to 0.3 for α = 5% and 1–β = 90%. We also determined a priori that 50 subjects would be necessary for test-retest reproducibility.18
Results
Translation and transcultural adaptation
In accordance with the published recommendations,14,16 we first worked from the English original version,1 which was then independently translated by three bilingual French native language translators, two of them being anesthesiologists. In addition, a published, though non-validated, French version was also taken into consideration.10 Secondly, three of the study authors who were representatives of the scientific board (A.S.F., J.E.B., and C.D.) and a specialist in scale construction (I.D.C.) debated the difference between the four versions and proposed equivalence to define the preliminary French version. Then, this first translated version was back-translated by two bilingual English native language professional translators, unaware of the original version. Thirdly, the scientific board compared the two back-translations to the original ISAS to evaluate and validate the semantic, idiomatic, conceptual, and experiential equivalences. The resultant pre-final version was validated by the creator of the ISAS (F.D.). Finally, this draft was tested by 33 members of the anesthetic team (physicians, residents, and nurses). The content of their comments was analyzed by the scientific board, and subsequent decisions were consensually taken. They determined the mean (SD) completion time to be 7 (5) min. Although 20 of them suggested reducing the redundancy, the original structure was preserved. Eight people suggested presenting the questionnaire on a single page, which was done. None of the instructions or items were changed. Lastly, a final version was elaborated by the study’s scientific board (Table 1). To prevent errors, the answer options were presented as a vertical list printed below each statement, as in the original design.1
Sample description
One hundred and twenty-three patients were included. Their characteristics and details of the procedure are shown in Table 2. The sample was representative of those usually undergoing such procedures in our hospital. The putative factors of dissatisfaction (i.e., pain, agitation/anxiety, postoperative nausea or vomiting [PONV]) were a minority. No patient required unscheduled hospitalization.
Description of the responses and acceptability
The completion rate was 99.1% (one patient declined to answer the questionnaire). The median [IQR] completion time at the first assessment was 2 [2–4] min, though four subjects needed more than six minutes to complete their answers. Fifty-eight patients answered the acceptability questionnaire before discharge; none of them felt it was too long and 4 (7.0%) reported personal difficulties in answering because of reading difficulties with no lenses, preference to binary responses, understanding difficulties, and redundancies.
The mean (SD) whole satisfaction score was 2.2 (0.7). Table 3 shows the results for each item. There was a floor- or a ceiling effect for most of the items, particularly for those related to PONV (item 1), itching (item 3), and pain (item 11), which also had a high level of disagreement.
Internal consistency
Table 4 shows the internal consistency conducted out the calculated subscores. For this analysis, the subscores related to dissatisfaction items were reversed. The correlation coefficient between each item and the total score (calculated after deletion of the tested item) was always superior to the critical value of 0.2, although it was close for the items “I threw up or felt like throwing up” and “I itched”, suggesting a poor relationship with the other satisfaction parameters. The Cronbach’s α for the whole questionnaire was 0.68.
Construct validity
Table 5 shows the correlation matrix between the subscores calculated for each item of the ISAS-F. For this analysis, the subscores related to dissatisfaction items were reversed. We intentionally separated the items with even numbers, which rather assess one putative cause of dissatisfaction (PONV, itch, cold/hot, and pain under various aspects), and those with odd numbers, which rather assess general perceptions of satisfaction. Considering the correlations within the first domain (even numbers), correlations were significant in 9/15 cases, with average-to-high coefficients (0.123 to 0.628). Within the second domain (odd numbers), correlations were always significant (10/10) with average-to-high coefficients (0.299 to 0.542). Nevertheless, in the submatrix facing the items of the first domain to those of the second, correlations were significant in only half of the cases (15/30), and coefficients were lower, especially when non-significant (0.016 to 0.174); the cross-domain correlations were mostly due to item 7 (“I was too cold or hot”) and item 2 (“I would want to have the same anesthetic again”).
Test-retest reliability
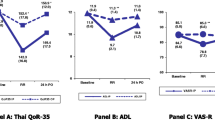
Fifty-eight patients underwent the retest. Within this subsample, the mean (SD) total ISAS-F score was 2.0 (0.7) and 2.0 (0.9) respectively for the first and second assessment (P = 0.57, Wilcoxon’s test for paired data). The intra-class coefficient of correlation was 0.74 (95% CI, 0.63 to 0.85; P < 0.001). The Figure shows the Bland-Altman plot of retest vs test.

Bland-Altman plot displaying the relationship between the retest vs test bias (y axis: difference between values from retest and test for each individual) and the theoretical real value (x axis: averaged value from test and retest for each individual). The quality of reliability is assessed by (i) the lesser number of individuals out of the 95% confidence interval limits and (ii) the monotonous distribution of these outliers along the x axis
Convergent validity
The mean (SD) total ISAS-F score as estimated by the physician was 2.0 (0.7), which was not significantly lower than the patient-assessed score (P = 0.07). The intra-class coefficient of correlation was 0.28 (95% CI, 0.12 to 0.44; P = 0.01).
Discussion
After having passed all the preliminary steps of scale building mandatory for a transcultural validation, our French version of the ISAS (ISAS-F) has passed the controls of construct validity, internal consistency, convergent validity, and test-retest reliability. Nevertheless, some quality indicators seemed to be less good than those of the validated versions of ISAS in other languages; this is addressed further below.
The ISAS-F had an excellent acceptability, as no missing data were reported, while the original study reported a 92% response rate.1 The median completion time of ISAS-F at the first assessment was two minutes, whereas the original study reported a median time of five minutes1; this could be explained partly by our presentation of the questionnaire on a single page. Completion time was also longer (mean: 6 min) in a study conducted in rural Colombia to validate a Spanish version,8 and this could potentially be explained by participants’ lower educational level.
In the current study, satisfaction with anesthesia was high, with a mean total ISAS-F score of 2.2 (while the theoretical range is -3 to 3), and a 95% rate of agreement to item 8 (“I was satisfied with my anesthetic care”). In the original study, these indicators were very close (2.1 and 96%, respectively).1 all are highly explained by the good quality of the monitored anesthesia care itself. As a result, we cannot avoid floor- or ceiling effects, especially when questions focus on a particularly infrequent event, such as PONV, itching, and hurting. In addition, satisfaction with care is generally high when recorded in industrialized countries.19
Internal consistency is usually assessed by the Cronbach’s α coefficient, which shows how the different items of the questionnaire are related to each other; a common rule states that values over 0.7 are required to assume an acceptable internal consistency.13,20 The value we observed for the whole questionnaire was very close but slightly inferior to this value (0.68). Among the previously published studies of the ISAS, our values were very close (0.68 and 0.71, respectively) to those values in a study using the original version in cataract surgery3 and in a Colombian study,8 while values were higher (respectively, 0.8 and 0.84) in the original study1 and in a trial testing dexmedetomidine vs placebo.7 We do note that the structure of the ISAS naturally alters internal consistency in some observations, as the items differ not only in what they explore but also in the way they do it. Indeed, the items with even numbers describe factual events that could have impaired satisfaction depending on the patient’s own tolerance; except for those related to pain/hurt (items 5, 9, and 11), which were interrelated in our study. The other items were less likely to impair satisfaction (PONV and itch could both be due, in part, to opioids). Conversely, the items with odd numbers describe different aspects of the patient’s perception of the whole care, and, not surprisingly, were strongly interrelated. In other words, a large part of internal consistency depends on these latter “satisfaction” items (which are naturally interrelated). The rest depends on the “bad event” items. These would impair interrelation if some events occurred more than others, and would increase interrelation if all events occurred simultaneously in a subgroup of patient (quite unlikely) or if all events were very infrequent. Thus, the better internal consistency observed in the previous dexmedetomidine trial7 could be because dissatisfaction due to pain was higher (according to items 5, 9, and 11) than in the current study. In addition, the interest of the ISAS lies more in its ability to list all the possible factors of (dis)satisfaction and to its sensitivity to interventions,7 than in its structure.
We expected a good test-retest reliability, as this was shown in all previous tests conducted under similar conditions. While the first test was generally done at the same time, reliability tended to decrease when the delay for retesting increased—i.e., an intra-class coefficient of correlation of 0.95 was observed when the delay did not exceed one hour, but decreased to 0.64 when retest was done after 12 hr or more.8 Similarly, it was low (0.57) when the first test was done before discharge and the retest several hours later.3 Nevertheless, the ISAS is not necessarily used repeatedly in clinical research. The best time to administer it should be a compromise between relevance (the patient must be fully aware and remindful of the events to assess) and feasibility.21
As satisfaction is naturally subjective, there is no other gold standard to assess it other than the patient’s satisfaction. Accordingly, we only tested convergent validity by comparing the patient’s scores with those predicted by the physician in charge. Despite a mild (but significant) correlation, this was not different to that reported in the original study.1 Only the Colombian study reported a high correlation, but the patient’s assessment was less independent from the physician’s.8
In conclusion, this French version of the ISAS has acceptable psychometrical properties, and can assess the patient’s satisfaction with monitored anesthesia care during various procedures. This ISAS-F scale should be useful for future research and should improve the quality of healthcare in French-speaking countries.
References
Dexter F, Aker J, Wright WA. Development of a measure of patient satisfaction with monitored anesthesia care: the Iowa Satisfaction with Anesthesia Scale. Anesthesiology 1997; 87: 865-73.
Hinz A, Michalski D, Schwarz R, Herzberg PY. The acquiescence effect in responding to a questionnaire. Psychosoc Med 2007; 4: Doc07.
Fung D, Cohen MM. Measuring patient satisfaction with anesthesia care: a review of current methodology. Anesth Analg 1998; 87: 1089-98.
Bell DM, Halliburton JR, Preston JC. An evaluation of anesthesia patient satisfaction instruments. AANA J 2004; 72: 211-7.
Barnett SF, Alagar RK, Grocott MP, Giannaris S, Dick JR, Moonesinghe SR. Patient-satisfaction measures in anesthesia: qualitative systematic review. Anesthesiology 2013; 119: 452-78.
Williams MR, McKeown A, Dexter F, et al. Efficacy outcome measures for procedural sedation clinical trials in adults: An ACTTION systematic review. Anesth Analg 2016; 122: 152-70.
Dexter F, Candiotti KA. Multicenter assessment of the Iowa Satisfaction with Anesthesia Scale, an instrument that measures patient satisfaction with monitored anesthesia care. Anesth Analg 2011; 113: 364-8.
García LFJ, del Real Capera A. Validation to Spanish of Iowa Satisfaction with Anesthesia Scale (ISAS) for monitored anesthesia care in ophthalmic surgery (Spanish). Rev Colomb Anestesiol 2014; 42: 272-80.
Dyk D, Ozga D, Gutysz-Wojnicka A, Lewandowski B, Wojtaszek M. Polish adaptation of the Iowa Satisfaction with Anaesthesia Scale. Pielegniarstwo XXI wieku 2016; https://doi.org/10.1515/pielxxiw-2016-0034.
Batta B, Fuchs-Buder T, Trechot F, Angioi K. Simplified topical anesthesia protocol for ambulatory cataract surgery: safety and patient and surgeon satisfaction (French). J Fr Ophtalmol 2014; 37: 548-56.
Malek I, Romdhane O, Sayadi J, et al. Cataract surgery with topical anesthesia in adults under 30 years of age: preliminary study (French). J Fr Ophtalmol 2016; 39: e297-8.
Acquadro C, Berzon R, Dubois D, et al. Incorporating the patient’s perspective into drug development and communication: an ad hoc task force report of the Patient-Reported Outcomes (PRO) Harmonization Group meeting at the Food and Drug Administration, February 16, 2001. Value Health 2003; 6: 522-31.
Skevington SM. Advancing cross-cultural research on quality of life: observations drawn from the WHOQOL development. World Health Organisation Quality of Life Assessment. Qual Life Res 2002; 11: 135-44.
Vallerand RJ. Vers une méthodologie de validation trans-culturelle de questionnaires psychologiques: implications pour la recherche en langue française. Can Psychol 1989; 30: 662-80.
Guillemin F, Bombardier C, Beaton D. Cross-cultural adaptation of health-related quality of life measures: literature review and proposed guidelines. J Clin Epidemiol 1993; 46: 1417-32.
Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine (Phila Pa 1976) 2000; 25: 3186-91.
Chernik DA, Gillings D, Laine H, et al. Validity and reliability of the Observer’s Assessment of Alertness/Sedation Scale: study with intravenous midazolam. J Clin Psychopharmacol 1990; 10: 244-51.
Terwee CB, Bot SD, de Boer MR, et al. Quality criteria were proposed for measurement properties of health status questionnaires. J Clin Epidemiol 2007; 60: 34-42.
Dualé C, Nicolas-Courbon A, Gerbaud L, Lemery D, Bonin M, Pereira B. Maternal satisfaction as an outcome criterion in research on labor analgesia: data analysis from the recent literature. Clin J Pain 2015; 31: 235-46.
Cortina JM. What is coefficient alpha? An examination of theory and application. J Appl Psychol 1993; 78: 98-104.
Chadha RM, Dexter F, Brull SJ. Lack of recall after sedation for cataract surgery and its effect on validity of measuring patient satisfaction. Korean J Anesthesiol 2019; https://doi.org/10.4097/kja.19314.
Author contributions
Anne-Sophie Falempin, Jean-Étienne Bazin, Ingrid de Chazeron, and Christian Dualé contributed to the conception of the French version of the questionnaire. Franklin Dexter created the original tool and checked the validity of the back-translated French version. Anne-Sophie Falempin, Jean-Étienne Bazin, Franklin Dexter, and Christian Dualé contributed to the conception and design of the clinical study. Anne-Sophie Falempin and Sophie Gonnu-Levallois contributed to the acquisition of data. Bruno Pereira and Christian Dualé contributed to the analysis of data. Anne-Sophie Falempin, Franklin Dexter, and Christian Dualé contributed to the interpretation of data and to drafting the manuscript.
Acknowledgements
For English to French translation: Jean-Michel Constantin and Emmanuel Futier, professors of anesthesiology and intensive care, CHU Clermont-Ferrand, Médecine Péri-Opératoire, Clermont-Ferrand, France; Université Clermont Auvergne, Clermont-Ferrand, France. For back-translation: Paul Riordan, BDS, PhD; Frances van Vyk de Vries, 1st class honours. For the pre-test: Isabelle Genès and the students in anesthesia nursing, Institut de Formation en Soins Infirmiers, Université Clermont Auvergne, Clermont-Ferrand, France. The Iowa Satisfaction with Anesthesia was used with written permission. The copyright in the scale is the property of Franklin Dexter and the University of Iowa Research Foundation.
Funding statement and conflict of interest
The Iowa Satisfaction with Anesthesia Scale is copyrighted by Franklin Dexter and the University of Iowa Research Foundation. Franklin Dexter receives no funds personally other than his salary and allowable expense reimbursements from the University of Iowa and has tenure with no incentive program. Income from uses of the Iowa Satisfaction with Anesthesia Scale is used to fund his research.
Editorial responsibility
This submission was handled by Dr. Hilary P. Grocott, Editor-in-Chief, Canadian Journal of Anesthesia.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Falempin, AS., Pereira, B., Gonnu-Levallois, S. et al. Transcultural validation of a French version of the Iowa Satisfaction with Anesthesia Scale (ISAS-F). Can J Anesth/J Can Anesth 67, 541–549 (2020). https://doi.org/10.1007/s12630-019-01563-w
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12630-019-01563-w