
Abstract
Objective
Chest pain is a common symptom in patients with hypertrophic cardiomyopathy (HCM), causing difficulty determining whether there is coexistent coronary artery disease (CAD). We investigated whether coronary computed tomography angiography (CCTA) can assess the prevalence and clinical significance of CAD in adult patients with HCM showing chest pain through longitudinal follow-up.
Methods
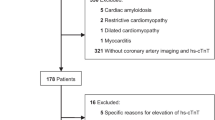
In 238 adult patients with HCM, who underwent CCTA for chest pain, we analyzed the degree of stenosis and adverse plaque characteristics (APCs) as CCTA variables. Three prediction models for adverse cardiovascular events (ACEs: all-cause mortality, myocardial infarction, unstable angina, heart failure, implantable cardioverter-defibrillator implantation, and stroke) were assessed using the combination of clinical risk factors, echocardiographic parameters, and CCTA variables.
Results
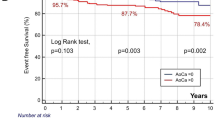
The prevalence of obstructive CAD (≥ 50% in luminal stenosis) and APC was 14.7% and 18.9%, respectively. During the follow-up period (median, 37 months; range, 2–108 months), there were 31 occurrences of ACEs (13.0%). Using multivariate Cox regression analysis, age, atrial fibrillation, low ejection fraction, obstructive CAD, and APCs were associated with ACEs (all p < 0.05). Among the prediction models for ACEs, the area under the curve (AUC) was higher (AUC = 0.92) when CCTA variables were added to the clinical (AUC = 0.84) and echocardiographic factors (AUC = 0.88) (p < 0.001).
Conclusions
Using CCTA, about 20% of symptomatic HCM patients were associated with clinically significant atherosclerosis. Adding these CCTA variables to the clinical and echocardiographic variables may increase the predictions of ACEs; therefore, evaluating coronary atherosclerosis using CCTA may be helpful for symptomatic HCM patients.
Key Points
• Chest pain in adult patients with hypertrophic cardiomyopathy (HCM) remains challenging to distinguish from coronary artery disease.
• Coronary computed tomography angiography (CCTA) can assess the severity and characteristics of coronary atherosclerosis in symptomatic HCM patients.
• Adding CCTA variables to clinical and echocardiographic factors may increase the predictions of adverse cardiac events in HCM patients, and thus evaluating coronary atherosclerosis using CCTA may be helpful for HCM patients with chest pain.



Similar content being viewed by others

Abbreviations
- ACEs:
-
Adverse cardiovascular events
- AF:
-
Atrial fibrillation
- APCs:
-
Adverse plaque characteristics
- AUC:
-
Area under the curves
- CAD:
-
Coronary artery disease
- CCTA:
-
Coronary computed tomography angiography
- CI:
-
Confidence interval
- ECG:
-
Electrocardiography
- EF:
-
Ejection fraction
- HCM:
-
Hypertrophic cardiomyopathy
- HR:
-
Hazard ratio
- HU:
-
Hounsfield units
- ICD:
-
Implantable cardioverter-defibrillator
- LV:
-
Left ventricle
- MI:
-
Myocardial infarction
- ROC:
-
Receiver-operator characteristic
- UA:
-
Unstable angina
References
Maron BJ (2002) Hypertrophic cardiomyopathy: a systematic review. JAMA 287:1308–1320
McKenna WJ, Camm AJ (1989) Sudden death in hypertrophic cardiomyopathy. Assessment of patients at high risk. Circulation 80:1489–1492
Spirito P, Chiarella F, Carratino L, Berisso MZ, Bellotti P, Vecchio C (1989) Clinical course and prognosis of hypertrophic cardiomyopathy in an outpatient population. N Engl J Med 320:749–755
Kofflard MJ, Waldstein DJ, Vos J, ten Cate FJ (1993) Prognosis in hypertrophic cardiomyopathy observed in a large clinic population. Am J Cardiol 72:939–943
Maron BJ, Casey SA, Hauser RG, Aeppli DM (2003) Clinical course of hypertrophic cardiomyopathy with survival to advanced age. J Am Coll Cardiol 42:882–888
Maron BJ, Bonow RO, Cannon RO 3rd, Leon MB, Epstein SE (1987) Hypertrophic cardiomyopathy. Interrelations of clinical manifestations, pathophysiology, and therapy (1). N Engl J Med 316:780–789
Ito C, Asano H, Shimada E, Yamane Y (1983) Hypertrophic cardiomyopathy presenting ECG changes mimicking myocardial infarction during 18 years: report of a case. J Cardiogr 13:1041–1049
Luzza F, Carerj S, Oreto G (2004) Hypertrophic cardiomyopathy with persistent ST segment elevation simulating acute myocardial infarction. Heart 90:380
Zhao L, Ma X, Ge H et al (2015) Diagnostic performance of computed tomography for detection of concomitant coronary disease in hypertrophic cardiomyopathy. Eur Radiol 25:767–775
Chun EJ, Choi SI, Jin KN et al (2010) Hypertrophic cardiomyopathy: assessment with MR imaging and multidetector CT. Radiographics 30:1309–1328
Voros S, Rinehart S, Qian Z et al (2011) Coronary atherosclerosis imaging by coronary CT angiography: current status, correlation with intravascular interrogation and meta-analysis. JACC Cardiovasc Imaging 4:537–548
Authors/Task Force Members, Elliott PM, Anastasakis A et al (2014) 2014 ESC guidelines on diagnosis and management of hypertrophic cardiomyopathy: the Task Force for the Diagnosis and Management of Hypertrophic Cardiomyopathy of the European Society of Cardiology (ESC). Eur Heart J 35:2733–2779
Rodrigues JC, Rohan S, Ghosh Dastidar A et al (2017) Hypertensive heart disease versus hypertrophic cardiomyopathy: multi-parametric cardiovascular magnetic resonance discriminators when end-diastolic wall thickness ≥ 15 mm. Eur Radiol 27:1125–1135
Messroghli DR, Moon JC, Ferreira VM et al (2018) Correction to: Clinical recommendations for cardiovascular magnetic resonance mapping of T1, T2, T2* and extracellular volume: a consensus statement by the Society for Cardiovascular Magnetic Resonance (SCMR) endorsed by the European Association for Cardiovascular Imaging (EACVI). J Cardiovasc Magn Reson 20:9
Anderson KM, Odell PM, Wilson PW, Kannel WB (1991) Cardiovascular disease risk profiles. Am Heart J 121:293–298
Sohn DW, Chai IH, Lee DJ et al (1997) Assessment of mitral annulus velocity by Doppler tissue imaging in the evaluation of left ventricular diastolic function. J Am Coll Cardiol 30:474–480
Maurovich-Horvat P, Schlett CL, Alkadhi H et al (2012) The napkin-ring sign indicates advanced atherosclerotic lesions in coronary CT angiography. JACC Cardiovasc Imaging 5:1243–1252
Motoyama S, Sarai M, Harigaya H et al (2009) Computed tomographic angiography characteristics of atherosclerotic plaques subsequently resulting in acute coronary syndrome. J Am Coll Cardiol 54:49–57
Nakazato R, Otake H, Konishi A et al (2015) Atherosclerotic plaque characterization by CT angiography for identification of high-risk coronary artery lesions: a comparison to optical coherence tomography. Eur Heart J Cardiovasc Imaging 16:373–379
Mintz GS, Nissen SE, Anderson WD et al (2001) American College of Cardiology Clinical Expert Consensus Document on Standards for Acquisition, Measurement and Reporting of Intravascular Ultrasound Studies (IVUS). a report of the American College of Cardiology Task Force on Clinical Expert Consensus Documents. J Am Coll Cardiol 37:1478–1492
Nishimura RA, Holmes DR Jr (2004) Clinical practice. Hypertrophic obstructive cardiomyopathy. N Engl J Med 350:1320–1327
Tio RA, Van Gelder IC, Boonstra PW, Crijns HJ (1997) Myocardial bridging in a survivor of sudden cardiac near-death: role of intracoronary doppler flow measurements and angiography during dobutamine stress in the clinical evaluation. Heart 77:280–282
Rowin EJ, Maron BJ, Olivotto I, Maron MS (2017) Role of exercise testing in hypertrophic cardiomyopathy. JACC Cardiovasc Imaging 10:1374–1386
O’Gara PT, Bonow RO, Maron BJ et al (1987) Myocardial perfusion abnormalities in patients with hypertrophic cardiomyopathy: assessment with thallium-201 emission computed tomography. Circulation 76:1214–1223
Cannon RO 3rd, Rosing DR, Maron BJ et al (1985) Myocardial ischemia in patients with hypertrophic cardiomyopathy: contribution of inadequate vasodilator reserve and elevated left ventricular filling pressures. Circulation 71:234–243
Maron BJ, Wolfson JK, Epstein SE, Roberts WC (1986) Intramural (“small vessel”) coronary artery disease in hypertrophic cardiomyopathy. J Am Coll Cardiol 8:545–557
Sorajja P, Ommen SR, Nishimura RA, Gersh BJ, Berger PB, Tajik AJ (2003) Adverse prognosis of patients with hypertrophic cardiomyopathy who have epicardial coronary artery disease. Circulation 108:2342–2348
Lazzeroni E, Rolli A, Aurier E, Botti G (1992) Clinical significance of coronary artery disease in hypertrophic cardiomyopathy. Am J Cardiol 70:499–501
Cokkinos DV, Krajcer Z, Leachman RD (1985) Hypertrophic cardiomyopathy and associated coronary artery disease. Tex Heart Inst J 12:147–151
Alegria JR, Herrmann J, Holmes DR Jr, Lerman A, Rihal CS (2005) Myocardial bridging. Eur Heart J 26:1159–1168
Shariat M, Thavendiranathan P, Nguyen E et al (2014) Utility of coronary CT angiography in outpatients with hypertrophic cardiomyopathy presenting with angina symptoms. J Cardiovasc Comput Tomogr 8:429–437
Sorajja P, Ommen SR, Nishimura RA, Gersh BJ, Tajik AJ, Holmes DR (2003) Myocardial bridging in adult patients with hypertrophic cardiomyopathy. J Am Coll Cardiol 42:889–894
Davies MJ (1996) Detecting vulnerable coronary plaques. Lancet 347:1422–1423
Virmani R, Kolodgie FD, Burke AP, Farb A, Schwartz SM (2000) Lessons from sudden coronary death: a comprehensive morphological classification scheme for atherosclerotic lesions. Arterioscler Thromb Vasc Biol 20:1262–1275
Puchner SB, Liu T, Mayrhofer T et al (2014) High-risk plaque detected on coronary CT angiography predicts acute coronary syndromes independent of significant stenosis in acute chest pain: results from the ROMICAT-II trial. J Am Coll Cardiol 64:684–692
Shapiro LM, Zezulka A (1983) Hypertrophic cardiomyopathy: a common disease with a good prognosis. Five year experience of a district general hospital. Br Heart J 50:530–533
Maron BJ, Roberts WC, Epstein SE (1982) Sudden death in hypertrophic cardiomyopathy: a profile of 78 patients. Circulation 65:1388–1394
Maron BJ, Rowin EJ, Casey SA et al (2013) Risk stratification and outcome of patients with hypertrophic cardiomyopathy >=60 years of age. Circulation 127:585–593
Sakamoto T, Amano K, Hada Y et al (1986) Asymmetric apical hypertrophy: ten years experience. Postgrad Med J 62:567–570
Funding
This work was supported by the National Research Foundation grant NRF-2015R1D1A1A01059717 funded by the Korea government (MEST).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Guarantor
The scientific guarantor of this publication is Kyung Won Lee.
Conflict of interest
The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article.
Statistics and biometry
Yongho Jeon, PhD (Department of Applied statistics, College of Commerce and Economics, Yonsei University), one of the authors, has contributed to the statistical analysis.
Informed consent
Written informed consent was waived by the Institutional Review Board.
Ethical approval
Institutional Review Board approval was obtained.
Methodology
• retrospective
• observational
• performed at one institution
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Shin, Y.J., Lee, J.H., Yoo, J.Y. et al. Clinical significance of evaluating coronary atherosclerosis in adult patients with hypertrophic cardiomyopathy who have chest pain. Eur Radiol 29, 4593–4602 (2019). https://doi.org/10.1007/s00330-018-5951-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-018-5951-8