
Abstract
Background
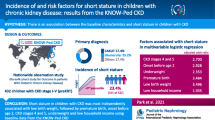
Among children who receive a kidney transplant, short stature is associated with a more complicated post-transplant course and increased mortality. Short stature prior to transplant may reflect the accumulated risk of multiple factors during chronic kidney disease (CKD); however, its relationship with post-transplant kidney function has not been well characterized.
Methods
In the Chronic Kidney Disease in Children (CKiD) cohort restricted to children who received a kidney transplant, short stature (i.e., growth failure) was defined as age-sex-specific height < 3rd percentile. The outcome was time to estimated glomerular filtration rate (eGFR) < 45 ml/min/1.73 m2 after transplant. Parametric survival models, including adjustment for disease severity, socioeconomic status (SES), and parental height by inverse probability weighting, described the relative times to eGFR< 45 ml/min/1.73 m2.
Results
Of 138 children (median CKD duration at transplant: 13 years), 20% (28) had short stature before the transplant. The median time to eGFR < 45 ml/min/1.73 m2 after kidney transplantation was 6.6 years and those with short stature had a significantly faster time to the poor outcome (log-rank p value 0.004). Children with short stature tended to have lower SES, nephrotic proteinuria, higher blood pressure, and lower mid-parental height before transplant. After adjusting for these variables, children with growth failure had 40% shorter time to eGFR < 45 ml/min/1.73 m2 than those with normal stature (relative time 0.60, 95%CI 0.32, 1.03).
Conclusions
Short stature was associated with a faster time to low kidney function after transplant. SES, disease severity, and parental height partially explained the association. Clinicians should be aware of the implications of growth failure on the outcome of this unique population, while continued attempts are made to define modifiable factors that contribute to this association.

Similar content being viewed by others

References
Wong H, Mylrea K, Feber J, Drukker A, Filler G (2006) Prevalence of complications in children with chronic kidney disease according to KDOQI. Kidney Int 70(3):585–590
Fine R, Martz K, Stablein D (2010) What have 20 years of data from the North American pediatric renal transplant cooperative study taught us about growth following renal transplantation in infants, children, and adolescents with end-stage renal disease? Pediatr Nephrol 25(4):739–746
Wong CS, Gipson DS, Gillen DL, Emerson S, Koepsell T, Sherrard DJ, Watkins SL, Stehman-Breen C (2000) Anthropometric measures and risk of death in children with end-stage renal disease. Am J Kidney Dis 36(4):811–819
Furth SL, Hwang W, Yang C, Neu AM, Fivush BA, Powe NR (2002) Growth failure, risk of hospitalization and death for children with end-stage renal disease. Pediatr Nephrol 17(6):450–455
Ku E, Fine RN, Hsu CY, McCulloch C, Glidden DV, Grimes B, Johansen KL (2016) Height at first RRT and mortality in children. Clin J Am Soc Nephrol 11(5):832–839
Zemel BS, Riley EM, Stallings VA (1997) Evaluation of methodology for nutritional assessment in children: anthropometry, body composition, and energy expenditure. Annu Rev Nutr 17(1):211–235
Prista A, Maia JAR, Damasceno A, Beunen G (2003) Anthropometric indicators of nutritional status: implications for fitness, activity, and health in school-age children and adolescents from Maputo, Mozambique. Am J Clin Nutr 77(4):952–959
Greenbaum LA, Warady BA, Furth SL (2009) Current advances in chronic kidney disease in children: growth, cardiovascular, and neurocognitive risk factors. Semin Nephrol 29(4):425–434
Abubakar A (2012) Socioeconomic status, anthropometric status and developmental outcomes of East-African children. In: Handbook of anthropometry. 2012th ed. Springer, New York, pp 2679–2693
Gurzkowska B, Kułaga Z, Litwin M, Gurzkowska B, Kułaga Z, Litwin M (2014) The relationship between selected socioeconomic factors and basic anthropometric parameters of school-aged children and adolescents in Poland. Eur J Pediatr 173(1):45–52
Gross R, Lima FD, Freitas CJ, Gross U (1990) The relationships between selected anthropometric and socio-economic data in schoolchildren from different social strata in Rio de Janeiro, Brazil. Rev Saude Publica 24(1):11–19
Furth SL, Cole SR, Moxey-Mims M, Kaskel F, Mak R, Schwartz G, Wong C, Muñoz A, Warady BA (2006) Design and methods of the chronic kidney disease in children (CKiD) prospective cohort study. Clin J Am Soc Nephrol 1(5):1006–1015
Schwartz GJ, Munoz A, Schneider MF, Mak RH, Kaskel F, Warady BA, Furth SL (2009) New equations to estimate GFR in children with CKD. J Am Soc Nephrol 20(3):629–637
de Souza V, Cochat P, Rabilloud M, Selistre L, Wagner M, Hadj-Aissa A, Dolomanova O, Ranchin B, Iwaz J, Dubourg L (2015) Accuracy of different equations in estimating GFR in pediatric kidney transplant recipients. Clin J Am Soc Nephrol 10(3):463–470
Center for Disease Control and Prevention (2000) Clinical Growth Charts. http://www.cdc.gov/growthcharts/ . Accessed 13 December 2017
Schwartz GJ, Schneider MF, Maier PS, Moxey-Mims M, Dharnidharka VR, Warady BA, Furth SL, Muñoz A (2012) Improved equations estimating GFR in children with chronic kidney disease using an immunonephelometric determination of cystatin C. Kidney Int 82(4):445–453
Pierce CB, Cox C, Saland JM, Furth SL, Muñoz A (2011) Methods for characterizing differences in longitudinal glomerular filtration rate changes between children with glomerular chronic kidney disease and those with nonglomerular chronic kidney disease. Am J Epidemiol 174(5):604–612
National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents (2004) The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics 114(2):555–576
Nwosu BU, Lee MM (2008) Evaluation of short and tall stature in children. Am Fam Physician 78(5):597–604
Ng DK, Moxey-Mims M, Warady BA, Furth SL, Muñoz A (2016) Racial differences in renal replacement therapy initiation among children with a nonglomerular cause of chronic kidney disease. Ann Epidemiol 26(11):780–787
Cole SR, Hernán MA (2008) Constructing inverse probability weights for marginal structural models. Am J Epidemiol 168(6):656–664
Rees L, Mak RH (2011) Nutrition and growth in children with chronic kidney disease. Nat Rev Nephrol 7(11):615–623
Apostolou A, Printza N, Karagiozoglou-Lampoudi T, Dotis J, Papachristou F (2014) Nutrition assessment of children with advanced stages of chronic kidney disease—a single center study. Hippokratia 18(3):212–216
Wesseling K, Bakkaloglu S, Salusky I (2008) Chronic kidney disease mineral and bone disorder in children. Pediatr Nephrol 23(2):195–207
Hidalgo G, Ng DK, Moxey-Mims M, Minnick ML, Blydt-Hansen T, Warady BA, Furth SL (2013) Association of income level with kidney disease severity and progression among children and adolescents with CKD: a report from the chronic kidney disease in children (CKiD) study. Am J Kidney Dis 62(6):1087–1094
Portale AA, Wolf M, Jüppner H, Messinger S, Kumar J, Wesseling-Perry K, Schwartz GJ, Furth SL, Warady BA, Salusky IB (2014) Disordered FGF23 and mineral metabolism in children with CKD. Clin J Am Soc Nephrol 9(2):344–353
Van Husen M, Fischer AK, Lehnhardt A, Klaassen I, Möller K, Müller-Wiefel KMJ (2010) Fibroblast growth factor 23 and bone metabolism in children with chronic kidney disease. Kidney Int 78(2):200–206
Wolf M, Molnar MZ, Amaral AP, Czira ME, Rudas A, Ujszaszi A, Kiss I, Rosivall L, Kosa J, Lakatos P, Kovesdy CP, Mucsi I (2011) Elevated fibroblast growth factor 23 is a risk factor for kidney transplant loss and mortality. J Am Soc Nephrol 22(5):956–966
Wesseling-Perry K, Tsai EW, Ettenger RB, Jüppner H, Salusky IB (2011) Mineral abnormalities and long-term graft function in pediatric renal transplant recipients: a role for FGF-23? Nephrol Dial Transplant 26(11):3779–3784
Seifert ME, Ashoor IF, Chiang ML, Chishti AS, Dietzen DJ, Gipson DS, Janjua HS, Selewski DT, Hruska KA (2016) Fibroblast growth factor-23 and chronic allograft injury in pediatric renal transplant recipients: a Midwest pediatric nephrology consortium study. Pediatr Transplant 20(3):378–387
Rees L (2016) Growth hormone therapy in children with CKD after more than two decades of practice. Pediatr Nephrol 31(9):1421–1435
Wong SC, Dobie R, Altowati MA, Werther GA, Farquharson C, Ahmed SF (2015) Growth and the growth hormone-insulin like growth factor 1 axis in children with chronic inflammation: current evidence, gaps in knowledge, and future directions. Endocr Rev 37(1):62–110
Van Ree RM, Oterdoom LH, De Vries AP, Gansevoort RT, van der Heide JJ, van Son WJ, Ploeg RJ, de Jong PE, Gans RO, Bakker SJ (2006) Elevated levels of C-reactive protein independently predict accelerated deterioration of graft function in renal transplant recipients. Nephrol Dial Transplant 22(1):246–253
Fink JC, Onuigbo MA, Blahut SA, Christenson RH, Mann D, Bartlett ST, Weir MR (2002) Pretransplant serum C-reactive protein and the risk of chronic allograft nephropathy in renal transplant recipients: a pilot case-control study. Am J Kidney Dis 39(5):1096–1101
Acknowledgements
Data in this manuscript were collected by the Chronic Kidney Disease in children prospective cohort study (CKiD) with clinical coordinating centers (Principal Investigators) at Children’s Mercy Hospital and the University of Missouri-Kansas City (Bradley Warady, MD) and Children’s Hospital of Philadelphia (Susan Furth, MD, PhD), Central Biochemistry Laboratory (George Schwartz, MD) at the University of Rochester Medical Center, and data coordinating center (Alvaro Muñoz, PhD) at the Johns Hopkins Bloomberg School of Public Health.
Funding
The CKiD Study is supported by grants from the National Institute of Diabetes and Digestive and Kidney Diseases, with additional funding from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, and the National Heart, Lung, and Blood Institute (U01-DK-66143, U01-DK-66174, U01DK-082194, U01-DK-66116). Supported by the National Center for Advancing Translational Sciences of the National Institutes of Health under Award number UL1TR002378. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The CKiD website is located at http://www.statepi.jhsph.edu/ckid.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The study protocol was approved by the institutional review board of each participating center. All participants and their families provided informed consent.
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Li, Y., Greenbaum, L.A., Warady, B.A. et al. Short stature in advanced pediatric CKD is associated with faster time to reduced kidney function after transplant. Pediatr Nephrol 34, 897–905 (2019). https://doi.org/10.1007/s00467-018-4165-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-018-4165-2