
Abstract
Objective: To analyze the lipid and glycemic profiles in relation to age, time elapsed post injury and the level of injury in a group of patients with SCI.
Subjects: 2135 subjects with SCI were recruited during the annual routine health check-up carried out at the Institut Guttmann of Badalona, in Spain. The patients were classified according to the level of SCI and their age.
Methods: Serum lipid profiles and glycemic (glucose) levels were determined. Data was collected between 1996 and 2001, all biochemical analysis being performed by the same laboratory.
Results: Serum cholesterol levels show a statistically significant correlation with patient's age (P<0.001) and with time elapsed after injury (P<0.05). Differences can be observed between the values obtained from the different injury level groups (F=22.14; P<0.001). LDL-c shows a statistically significant difference between the four different age groups (F=3.51, P<0.05). There is an increase in plasma triglycerides related to the increase in age of the patients without observable differences between the injury level groups. The concentration of serum glucose increases with age (P<0.001) and also with the time elapsed after injury (P<0.05).
Conclusion: There is a direct relationship between various biochemical parameters (total cholesterol, LDL-c and glucose) and the age of the patients, but not with the severity or time of evolution of the spinal cord injury.
Similar content being viewed by others

Introduction
Thanks to recent medical and surgical advances, the life expectancy in patients with spinal cord injuries now approximates to that of the general population. They have a better quality of life due in part to present rehabilitation programs. The causes of mortality in SCI patients have varied over the years: urological sepsis, pressure sores, kidney failure, or pneumonia have been replaced by that of cardiovascular disease, which correlates with that observed in the general population.1 The risk of cardiovascular disease continues to be one of the emergent pathologies in the general population and therefore, the increase in life expectancy of these spinal cord injury patients allows for the manifestation of this pathology, which occurs prematurely, possibly because of the sedentary lifestyle imposed by paralysis.
It is well-known that an increase in LDL-cholesterol (LDL-c) and a decrease in HDL-cholesterol (HDL-c) are indicators of an increased risk of atherogenesis and, therefore, of an increase morbidity and mortality due to cardiovascular disease.2,3 In patients with spinal cord injuries, a higher incidence of premature cardiovascular disease4 has been reported by some authors, on the other hand serum HDL-c levels are lower in spinal cord injury (SCI) patients compared with those of a control group of able bodied individuals, possibly due to an inactive lifestyle and a concomitant reduction of cardiopulmonary fitness of persons with SCI.5 The determination of the lipid profile continues to be one of the basic parameters for the evaluation of the vascular risk. Coronary heart disease is the cause of death of 46% of the patients who live more than 30 years after a spinal cord injury, but despite reductions in functional abilities associated with the aging process, the patients reported generally to be in good health and rated their current quality of life as either good or excellent.6
The neurological level, the patient's age, the degree of physical activity, and diet are factors that influence the lipid profile of patients with SCI. Some authors find no relationship between the level of the injury or the duration since the injury and the lipid profile7,8 and report that, compared to the able bodied population, patients with a spinal cord injury do not show higher levels of cholesterol or LDL, or lower levels of HDL.
Not only have risk factors associated with the metabolism of the lipids been described but some authors have shown that intolerance to glucose is more frequent in patients with SCI than in able-bodied persons,9 prolonged inactivity has been shown to impair glucose tolerance and is associated with hyperinsulinemia.10,11 A state of insulin resistance and hyperinsulinemia is becoming recognized as an atherogenic condition.
The present study analyzes the lipid glucemic profiles in relation to age, time of lesion and the level of injury in a group of patients with SCI.
Patients and methods
Patients
This study has been carried out at the Institut Guttmann of Badalona, in Spain, a Neurorehabilitation Hospital where a complete medical check up for all patients affected by paraplegia or tetraplegia is routinely being performed. This is done in order to detect and, eventually, correct any metabolic and/or functional disturbances that can lead, in the future to overt pathologies. The protocol of this study was previously accepted by the Research and Ethical Committee.
In this study the data obtained in 2135 annual routine health check-ups carried out on patients referred to the Institut Guttmann between 1996 and 2001 were analyzed; 72% were men and 28% were women aged 50.08±16.25 años (average±SD). The distribution of the population studied according to the ASIA classification was 65% ASIA A, 17% B, 10% C and 8% D. The patients were divided into three groups according to the level of SCI: group 1, with cervical and high thoracic lesions (lesions above Th5); group 2, with thoracic lesions between Th6 and Th12; group 3, patients with lesions below L1. On the other hand the patients have been divided into four groups according to age: group I (younger than 35 years), group II (between 35 and 55 years), group III (between 55 and 70 years) and group IV (older than 70 years).
Methods
Blood samples were obtained during the annual revision, after an overnight fast; the subjects had done no strenuous physical exercise the day before. A complete biochemical analysis was done using an automatic analyser Hitachi model 717 (Roche, Japan) and the following blood parameters were determined: total cholesterol, HDL-c, LDL-c, triglycerides and glucose.
The age of the patients or the time elapsed post injury were compared with each of the biochemical parameters obtained. An analysis of variance was carried out, to determine the possible influence of the age and level of the injury of the patients on the values obtained (P<0.5 is considered statistically significant).
Results
There is a statistically significant correlation betwen serum cholesterol levels and patient's age (P<0.001) (Figure 1) and also the duration since the injury (P<0.05). A statistically significant difference was also observed between the values obtained in the different groups according to the injury level groups (F=22.14; P<0.01) (Table 2) and to the age range of the four different groups (F=116.25; P<0.001). (Table 1). Serum HDL-c values show a significant increase with age (P<0.05), with the highest levels in those patients older than 70 years (group IV). LDL-c showed a statistically significant correlation with age (P=0.001) and also with the duration of the injury (P<0.05); values increased over time. A statistically significant difference was observed for the values obtained in the four different age groups (F=3.51; P<0.05), (Table 1). Serum triglycerides showed a statistically significant correlation with the patient's age (P<0.05), the highest levels being found in the older patients. Serum glucose shows a statistically significant correlation with the patient's age (P<0.001) and also with the time elapsed post injury (P<0.05); glucose levels increased over time. Statistically significant differences can be observed between the values obtained in the four different age groups (F=83.49; P<0.001), (Table 1), while no differences between the three injury level groups nor in those patients distributed according to the ASIA classification can be observed.

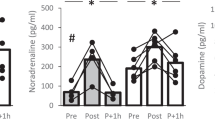
Evolution of the different parameters in the different age groups. (*P<0.05)
Discussion
In the general population, the concentration of total serum cholesterol shows a significant tendency to increase with age, with clear differences between the different age groups. Patients with SCI exhibit a similar temporal evolution as the able bodied. In our study the observed values for total cholesterol in spinal cord injury patients are very similar to those found by other authors in studies carried out in similar populations of able-bodied persons at the moment of the check up12 and within the parameters defined by the laboratory of reference. In our group a higher concentration of serum cholesterol appears to be present in a higher proportion of patients affected by a lower lesion; thus serum cholesterol values are 10% higher in patients with lesion levels below L1 compared to those with an injury at the cervical region or high thoracic level (group 1) (Figure 2). The reason for this difference could be that the age of those of group 3 (patients with lesions below L1) is superior to those in groups 1 and 2; in the normal population, serum cholesterol increases with age. In any case, age has a greater effect on the levels of total cholesterol than the level of injury.

Evolution of the different biochemical parameters in the different injury level groups
HCL-c levels did not show a correlation with the level of lesion, although lower values were found where the lesion is higher (the lowest values were in group 1). This has also been described by other authors where the most adverse lipid changes correlated with the severity of neurological deficit.13 An inverse correlation between serum triglycerides and HDL-c has been described in subjects with paraplegia and quadriplegia.14 In our case, this inverse correlation is not statistically significant although a trend in this direction can be observed in the patients pertaining to group 1 (with cervical and high thoracic lesions) showing the highest serum triglyceride concentrations and the lowest levels of HDLc (Table 2). This inverse relationship may reflect the effects of plasma insulin, elevated as a consequence of reduced peripheral insulin sensitivity, on lipid metabolism. The ratio of serum total cholesterol to HDL-c is a particularly strong discriminator of risk of myocardial infarction.14
The concentration of LDL-c shows a tendency to increase with age, this depended more on the normal evolution that this value undergoes over the years than with the spinal cord injury or the level of the same. The SCI population does not show levels of LDL-c significantly higher than those of the normal population.7 In our group no statistically significant correlation between age, duration post injury or level of injury and serum LDL-c were observed, a fact confirmed also by other authors.15
Glucose intolerance occurs more frequently in individuals with SCI than in able bodied persons. Some authors have reported the existence of higher plasma glucose levels in patients with complete motor tetraplegia, and in other groups with different neurological deficits after a 75 g glucose load,15 in our case, the plasma glucose values appear to be within normal limits. Nevertheless, a statistically significant tendency to increase with age can be observed, (Figure 1) although with no correlation with the level of injury.
Conclusion
In summary, important modifications of certain biochemical parameters (total cholesterol, HDL-c, LDL-c, and glucose) with age can be observed in these patients, but not with the severity or time of evolution of the spinal cord injury. The evolution of these metabolic parameters is similar to that observed in the able-bodied population.
References
Washburn RA & Figoni SF . High density lipoprotein cholesterol in individuals with spinal cord injury. The potential role of physical activity. Spinal Cord 1999; 37: 685–695.
Castelli WP & Lead A . Identification and assessment of cardiac risk an overview. Cardiol Clin 1985; 3: 171–178.
Gordon T & Castelli WP . High density lipoprotein as a protective factor against CHD. The Framinghan Study. Am J Med 1977; 62: 707–709.
Samsa P, Patrick C & Feusner JR . Long term survival of veterans with traumatic spinal cord injury. Arch Neurol 1993; 50: 909–914.
Bauman WA et al. Is immobilization associated with an abnormal lipoprotein profile? Observations from a diverse cohort. Spinal Cord 1999; 37: 485–493.
Whiteneck GG et al. Mortality, morbidity, and psychosocial outcomes of persons spinal cord injured more than 20 years ago. Paraplegia 1992; 30: 617–630.
Cardús F, Ribas-Cardús F & Taggant MC . Lipid profiles in spinal cord injury. Paraplegia 1992; 30: 775–782.
Cardús D, Ribas-Cardús F & Taggant MC . Coronary risk in spinal cord injury: assessment following a multivariate approach. Arch Phys Med Rehabil 1992; 73: 930–933.
Duckworth WC et al. Glucose intolerance due to insulin resistance in patients with spinal cord injury. Diabetes 1980; 29: 906–910.
Lipman RL et al. Glucose intolerance during decreased physical activity in man. Diabetes 1972; 21: 101–107.
Lipman RL et al. Impairment of peripheral glucose utilitation in normal subjects by prolonged bed rest. J Lab Clin Med 1970; 76: 221–230.
Sentí M et al. Determinantes antropométricos y dietéticos de la concentración sérica del colesterol de las lipoproteínas de alta densidad en un estudio de base problacional. El estudio REGICOR. Rev Esp Cardiol 1998; 51: 979–987.
Bauman WA et al. The effect of residual neurological deficit on serum lipoproteins in individuals with chronic cord injury. Spinal Cord 1998; 36: 13–17.
Bauman WA et al. Depressed serum high density lipoprotein cholesterol levels in veterans with spinal cord injury. Paraplegia 1992; 30: 697–703.
Baunman WA & Spungen AM . Metabolic changes in persons after spinal cord injury. Topics in Spinal Cord Injury Medicine 2000; 11: 109–140.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Vidal, J., Javierre, C., Curià, F. et al. Long-term evolution of blood lipid profiles and glycemic levels in patients after spinal cord injury. Spinal Cord 41, 178–181 (2003). https://doi.org/10.1038/sj.sc.3101390
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.sc.3101390
Keywords
This article is cited by
-
Long-term follow-up of patients with spinal cord injury with a new ICF-based tool
Spinal Cord (2011)
-
Traumatic and non-traumatic spinal cord-injured patients in Quebec, Canada. Part 2: biochemical profile
Spinal Cord (2010)
-
Intensity of pain and biochemical changes in blood plasma in spinal cord trauma
Spinal Cord (2010)
