
Abstract
Background:
Utilization of active surveillance (AS) for prostate cancer is increasing. Optimal selection criteria for this approach are undefined and questions remain on how best to expand inclusion beyond typical men with very low- or low-risk disease. We sought to review the current experience with AS for men with intermediate-risk features
Methods:
PubMed was queried for all relevant original publications describing outcomes for men with prostate cancer managed with AS. Outcomes for patients with intermediate-risk features as defined by the primary investigators were studied when available and compared with similar risk men undergoing immediate treatment.
Results:
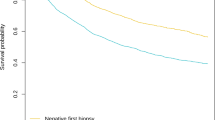
Cancer-specific survival for men managed initially with AS is similar to results published with immediate radical intervention. A total of five published AS series describe some outcomes for men with intermediate-risk features. Definitions of intermediate risk vary between studies. Men with Gleason 7 disease experience higher rates of clinical progression and are more likely to undergo treatment over time. Intermediate-risk men with Gleason 6 disease have similar outcomes to low-risk men. Men with Gleason 7 disease appear at higher risk for metastatic disease. Novel technologies including imaging and biomarkers may assist with patient selection and disease surveillance.
Conclusions:
The contemporary experiences of AS for men with intermediate-risk features suggest that although these men are at higher risk for eventual prostate-directed treatment, some are not significantly compromising chances for longer-term cure. Men with more than minimal Gleason pattern 4, however, must be carefully selected and surveyed for early signs of progression and may be at increased risk of metastases. Incorporating information from advanced imaging and biomarker technology will likely individualize future treatment decisions while improving overall surveillance strategies.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 4 print issues and online access
$259.00 per year
only $64.75 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout
Similar content being viewed by others

References
Cooperberg MR, Carroll PR . Trends in management for patients with localized prostate cancer, 1990-2013. JAMA 2015; 314: 80–82.
Moyer VA . Force USPST. Screening for prostate cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med 2012; 157: 120–134.
Hernandez DJ, Nielsen ME, Han M, Partin AW . Contemporary evaluation of the D'amico risk classification of prostate cancer. Urology 2007; 70: 931–935.
Cooperberg MR, Freedland SJ, Pasta DJ, Elkin EP, Presti JC Jr, Amling CL et al. Multiinstitutional validation of the UCSF cancer of the prostate risk assessment for prediction of recurrence after radical prostatectomy. Cancer 2006; 107: 2384–2391.
Klotz L, Vesprini D, Sethukavalan P, Jethava V, Zhang L, Jain S et al. Long-term follow-up of a large active surveillance cohort of patients with prostate cancer. J Clin Oncol 2015; 33: 272–277.
Stephenson AJ, Kattan MW, Eastham JA, Bianco FJ Jr, Yossepowitch O, Vickers AJ et al. Prostate cancer-specific mortality after radical prostatectomy for patients treated in the prostate-specific antigen era. J Clin Oncol 2009; 27: 4300–4305.
Stattin P, Holmberg E, Johansson JE, Holmberg L, Adolfsson J, Hugosson J et al. Outcomes in localized prostate cancer: National Prostate Cancer Register of Sweden follow-up study. J Natl Cancer Inst 2010; 102: 950–958.
Eggener SE, Scardino PT, Walsh PC, Han M, Partin AW, Trock BJ et al. Predicting 15-year prostate cancer specific mortality after radical prostatectomy. J Urol 2011; 185: 869–875.
Gandaglia G, Schiffmann J, Schlomm T, Fossati N, Moschini M, Suardi N et al. Identification of pathologically favorable disease in intermediate-risk prostate cancer patients: implications for active surveillance candidates selection. Prostate 2015; 75: 1484–1491.
Arvold ND, Chen MH, Moul JW, Moran BJ, Dosoretz DE, Banez LL et al. Risk of death from prostate cancer after radical prostatectomy or brachytherapy in men with low or intermediate risk disease. J Urol 2011; 186: 91–96.
Raldow AC, Zhang D, Chen MH, Braccioforte MH, Moran BJ, D'Amico AV . Risk group and death from prostate cancer: implications for active surveillance in men with favorable intermediate-risk prostate cancer. JAMA Oncol 2015; 1: 334–340.
Schiavina R, Borghesi M, Brunocilla E, Romagnoli D, Diazzi D, Giunchi F et al. The biopsy Gleason score 3+4 in a single core does not necessarily reflect an unfavourable pathological disease after radical prostatectomy in comparison with biopsy Gleason score 3+3: looking for larger selection criteria for active surveillance candidates. Prostate Cancer Prostatic Dis 2015; 18: 270–275.
Weiner AB, Patel SG, Etzioni R, Eggener SE . National trends in the management of low and intermediate risk prostate cancer in the United States. J Urol 2015; 193: 95–102.
Loeb S, Berglund A, Stattin P . Population based study of use and determinants of active surveillance and watchful waiting for low and intermediate risk prostate cancer. J Urol 2013; 190: 1742–1749.
Epstein JI, Allsbrook WC Jr, Amin MB, Egevad LL, Committee IG . The 2005 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma. Am J Surg Pathol 2005; 29: 1228–1242.
Yamamoto T, Musunuru B, Vesprini D, Zhang L, Ghanem G, Loblaw A et al. Metastatic prostate cancer in men initially treated with active surveillance. J Urol 2015; 195: 1409–1414.
Cooperberg MR, Cowan JE, Hilton JF, Reese AC, Zaid HB, Porten SP et al. Outcomes of active surveillance for men with intermediate-risk prostate cancer. J Clin Oncol 2011; 29: 228–234.
Bul M, van den Bergh RC, Zhu X, Rannikko A, Vasarainen H, Bangma CH et al. Outcomes of initially expectantly managed patients with low or intermediate risk screen-detected localized prostate cancer. BJU Int 2012; 110: 1672–1677.
van den Bergh RC, Roemeling S, Roobol MJ, Aus G, Hugosson J, Rannikko AS et al. Gleason score 7 screen-detected prostate cancers initially managed expectantly: outcomes in 50 men. BJU Int 2009; 103: 1472–1477.
Selvadurai ED, Singhera M, Thomas K, Mohammed K, Woode-Amissah R, Horwich A et al. Medium-term outcomes of active surveillance for localised prostate cancer. Eur Urol 2013; 64: 981–987.
Newcomb LF, Thompson IM Jr, Boyer HD, Brooks JD, Carroll PR, Cooperberg MR et al. Outcomes of active surveillance for the management of clinically localized prostate cancer in the prospective, multi-institutional canary PASS cohort. J Urol 2015; 195: 313–320.
Daskivich TJ, Kwan L, Dash A, Saigal C, Litwin MS . An age adjusted comorbidity index to predict long-term, other cause mortality in men with prostate cancer. J Urol 2015; 194: 73–78.
Conti SL, Dall'era M, Fradet V, Cowan JE, Simko J, Carroll PR . Pathological outcomes of candidates for active surveillance of prostate cancer. J Urol 2009; 181: 1628–1633.
Smaldone MC, Cowan JE, Carroll PR, Davies BJ . Eligibility for active surveillance and pathological outcomes for men undergoing radical prostatectomy in a large, community based cohort. J Urol 2010; 183: 138–143.
Tosoian JJ, JohnBull E, Trock BJ, Landis P, Epstein JI, Partin AW et al. Pathological outcomes in men with low risk and very low risk prostate cancer: implications on the practice of active surveillance. J Urol 2013; 190: 1218–1222.
El Hajj A, Ploussard G, de la Taille A, Allory Y, Vordos D, Hoznek A et al. Analysis of outcomes after radical prostatectomy in patients eligible for active surveillance (PRIAS). BJU Int 2013; 111: 53–59.
Thomsen FB, Marcussen N, Berg KD, Christensen IJ, Vainer B, Iversen P et al. Repeated biopsies in patients with prostate cancer on active surveillance: clinical implications of interobserver variation in histopathological assessment. BJU Int 2015; 115: 599–605.
Dinh KT, Muralidhar V, Mahal BA, Chen YW, Nezolosky MD, Beard CJ et al. Occult high-risk disease in clinically low-risk prostate cancer with >/=50% positive biopsy cores: should national guidelines stop calling them low-risk? Urology 2015; 87: 125–132.
Yu J, Kwon YS, Kim S, Han CS, Farber N, Kim J et al. Pathological outcome following radical prostatectomy in men with PSA greater than 10 and histologically favorable-risk prostate cancer. J Urol 2015; 195: 1464–1470.
Faisal FA, Sundi D, Pierorazio PM, Ball MW, Humphreys EB, Han M et al. Outcomes of men with an elevated prostate-specific antigen (PSA) level as their sole preoperative intermediate- or high-risk feature. BJU Int 2014; 114: E120–E129.
Epstein JI, Egevad L, Amin MB, Delahunt B, Srigley JR, Humphrey PA et al. The 2014 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma: Definition of Grading Patterns and Proposal for a New Grading System. Am J Surg Pathol 2016; 40: 244–252.
Huang CC, Kong MX, Zhou M, Rosenkrantz AB, Taneja SS, Melamed J et al. Gleason score 3 + 4=7 prostate cancer with minimal quantity of Gleason pattern 4 on needle biopsy is associated with low-risk tumor in radical prostatectomy specimen. Am J Surg Pathol 2014; 38: 1096–1101.
Cuzick J, Stone S, Fisher G, Yang ZH, North BV, Berney DM et al. Validation of an RNA cell cycle progression score for predicting death from prostate cancer in a conservatively managed needle biopsy cohort. Br J Cancer 2015; 113: 382–389.
Klein EA, Cooperberg MR, Magi-Galluzzi C, Simko JP, Falzarano SM, Maddala T et al. A 17-gene assay to predict prostate cancer aggressiveness in the context of Gleason grade heterogeneity, tumor multifocality, and biopsy undersampling. Eur Urol 2014; 66: 550–560.
Cullen J, Rosner IL, Brand TC, Zhang N, Tsiatis AC, Moncur J et al. A biopsy-based 17-gene genomic prostate score predicts recurrence after radical prostatectomy and adverse surgical pathology in a racially diverse population of men with clinically low- and intermediate-risk prostate cancer. Eur Urol 2015; 68: 123–131.
Leapman MS, Nguyen HG, Cooperberg MR . Clinical utility of biomarkers in localized prostate cancer. Curr Oncol Rep 2016; 18: 30.
Goh CL, Saunders EJ, Leongamornlert DA, Tymrakiewicz M, Thomas K, Selvadurai ED et al. Clinical implications of family history of prostate cancer and genetic risk single nucleotide polymorphism (SNP) profiles in an active surveillance cohort. BJU Int 2013; 112: 666–673.
Kearns JT, Lapin B, Wang E, Roehl KA, Cooper P, Catalona WJ et al. Associations between iCOGS single nucleotide polymorphisms and upgrading in both surgical and active surveillance cohorts of men with prostate cancer. Eur Urol 2016; 69: 223–228.
Oh JJ, Park S, Lee SE, Hong SK, Lee S, Choe G et al. The use of exome genotyping to predict pathological Gleason score upgrade after radical prostatectomy in low-risk prostate cancer patients. PLoS One 2014; 9: e104146.
Dall'Era MA, Konety BR, Cowan JE, Shinohara K, Stauf F, Cooperberg MR et al. Active surveillance for the management of prostate cancer in a contemporary cohort. Cancer 2008; 112: 2664–2670.
Washington SL, Bonham M, Whitson JM, Cowan JE, Carroll PR . Transrectal ultrasonography-guided biopsy does not reliably identify dominant cancer location in men with low-risk prostate cancer. BJU Int 2012; 110: 50–55.
Siddiqui MM, Rais-Bahrami S, Turkbey B, George AK, Rothwax J, Shakir N et al. Comparison of MR/ultrasound fusion-guided biopsy with ultrasound-guided biopsy for the diagnosis of prostate cancer. JAMA 2015; 313: 390–397.
Walton Diaz A, Shakir NA, George AK, Rais-Bahrami S, Turkbey B, Rothwax JT et al. Use of serial multiparametric magnetic resonance imaging in the management of patients with prostate cancer on active surveillance. Urol Oncol 2015; 33: 202 e1–202 e7.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
Dr Dall’Era has received compensation from Genomic Health for his roles as advisor and speaker. Dr Klotz declares no conflict of interest.
Rights and permissions
About this article

Cite this article
Dall'Era, M., Klotz, L. Active surveillance for intermediate-risk prostate cancer. Prostate Cancer Prostatic Dis 20, 1–6 (2017). https://doi.org/10.1038/pcan.2016.51
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/pcan.2016.51
This article is cited by
-
No significant difference in intermediate key outcomes in men with low- and intermediate-risk prostate cancer managed by active surveillance
Scientific Reports (2022)
-
Five-alpha reductase inhibitors in men undergoing active surveillance for prostate cancer: impact on treatment and reclassification after 6 years follow-up
World Journal of Urology (2021)
-
Active surveillance voor prostaatkanker: vergelijking van uitkomsten tussen patiënten die wel of niet aan de PRIAS-criteria voldoen
Tijdschrift voor Urologie (2020)
-
Understanding of prognosis in non-metastatic prostate cancer: a randomised comparative study of clinician estimates measured against the PREDICT prostate prognostic model
British Journal of Cancer (2019)
-
Radical prostatectomy or radiotherapy reduce prostate cancer mortality in elderly patients: a population-based propensity score adjusted analysis
World Journal of Urology (2018)
