当前位置:
X-MOL 学术
›
Prostate Cancer Prostatic. Dis.
›
论文详情
Our official English website, www.x-mol.net, welcomes your feedback! (Note: you will need to create a separate account there.)
Validation of a genomic classifier for prediction of metastasis and prostate cancer-specific mortality in African-American men following radical prostatectomy in an equal access healthcare setting.
Prostate Cancer and Prostatic Diseases ( IF 4.8 ) Pub Date : 2019-12-16 , DOI: 10.1038/s41391-019-0197-3 Lauren E Howard 1, 2 , Jingbin Zhang 3 , Nick Fishbane 3 , Amanda M De Hoedt 2 , Zachary Klaassen 4 , Daniel E Spratt 5 , Adriana C Vidal 6 , Dechen Lin 7, 8 , Megan P Hitchins 7, 8 , Sungyong You 6, 9 , Michael R Freeman 6, 9 , Kosj Yamoah 10 , Elai Davicioni 3 , Stephen J Freedland 2, 6
Prostate Cancer and Prostatic Diseases ( IF 4.8 ) Pub Date : 2019-12-16 , DOI: 10.1038/s41391-019-0197-3 Lauren E Howard 1, 2 , Jingbin Zhang 3 , Nick Fishbane 3 , Amanda M De Hoedt 2 , Zachary Klaassen 4 , Daniel E Spratt 5 , Adriana C Vidal 6 , Dechen Lin 7, 8 , Megan P Hitchins 7, 8 , Sungyong You 6, 9 , Michael R Freeman 6, 9 , Kosj Yamoah 10 , Elai Davicioni 3 , Stephen J Freedland 2, 6
Affiliation
|
BACKGROUND
The Decipher 22-gene genomic classifier (GC) may help in post-radical prostatectomy (RP) decision making given its superior prognostic performance over clinicopathologic variables alone. However, most studies evaluating the GC have had a modest representation of African-American men (AAM). We evaluated the GC within a large Veteran Affairs cohort and compared its performance to CAPRA-S for predicting outcomes in AAM and non-AAM after RP.
METHODS
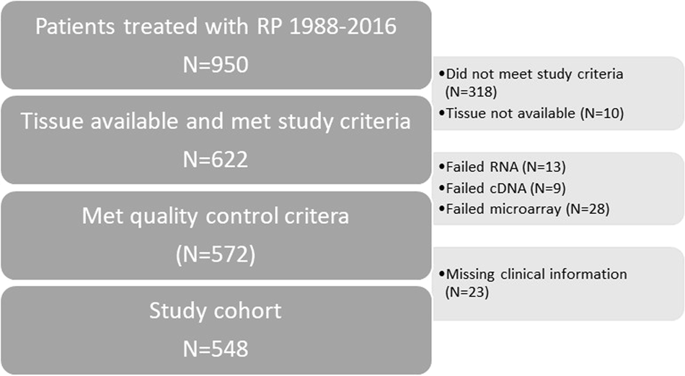
GC scores were generated for 548 prostate cancer (PC) patients, who underwent RP at the Durham Veteran Affairs Medical Center between 1989 and 2016. This was a clinically high-risk cohort and was selected to have either pT3a, positive margins, seminal vesicle invasion, or received post-RP radiotherapy. Multivariable Cox models and survival C-indices were used to compare the performance of GC and CAPRA-S for predicting the risk of metastasis and PC-specific mortality (PCSM).
RESULTS
Median follow-up was 9 years, during which 37 developed metastasis and 20 died from PC. Overall, 55% (n = 301) of patients were AAM. In multivariable analyses, GC (high vs. intermediate and intermediate vs. low) was a significant predictor of metastasis in all men (all p < 0.001). Consistent with prior studies, relative to CAPRA-S, GC had a higher C-index for 5-year metastasis (0.78 vs. 0.72) and 10-year PCSM (0.85 vs. 0.81). There was a suggestion GC was a stronger predictor in AAM than non-AAM. Specifically, the 5-year metastasis risk C-index was 0.86 in AAM vs. 0.69 in non-AAM and the 10-year PCSM risk C-index was 0.91 in AAM vs. 0.78 in non-AAM. However, the test for interaction of race and the performance of the GC in the Cox model was not significant for either metastasis or PCSM (both p ≥ 0.3).
CONCLUSIONS
GC was a very strong predictor of poor outcome and performed well in both AAM and non-AAM. Our data support the use of GC for risk stratification in AAM post-RP. While our data suggest that GC may actually work better in AAM, given the limited number of events, further validation is needed.
中文翻译:

在平等访问医疗机构中,进行根治性前列腺切除术后非裔美国人男性中转移和前列腺癌特异性死亡率的预测的基因组分类器的验证。
背景技术Decipher 22基因基因组分类器(GC)可以帮助根治性前列腺切除术(RP)做出决策,因为它的预后优于单纯的临床病理变量。但是,大多数评估GC的研究对非洲裔美国人(AAM)的代表均不多。我们评估了大型退伍军人事务队列中的GC,并将其性能与CAPRA-S进行了比较,以预测RP后AAM和非AAM的结局。方法1989年至2016年间,对548名前列腺癌(PC)患者进行了GC评分,这些患者在达勒姆退伍军人事务医疗中心接受了RP。这是临床上高危人群,被选择为pT3a,阳性切缘和精囊入侵或接受RP后放疗。使用多变量Cox模型和生存率C指数比较GC和CAPRA-S在预测转移风险和PC特异性死亡率(PCSM)方面的表现。结果中位随访9年,其中37例发生转移,20例因PC死亡。总体而言,有55%(n = 301)的患者为AAM。在多变量分析中,GC(高位vs.中位和中位vs.低位)是所有男性转移的重要预测指标(所有p <0.001)。与之前的研究一致,相对于CAPRA-S,GC的5年转移(0.78 vs. 0.72)和10年PCSM(0.85 vs. 0.81)的C指数更高。有人建议,GC比非AAM更能预测AAM。具体而言,AAM的5年转移风险C指数为0.86,非AAM为0.69,10年PCSM风险C指数在AAM为0.91,而非AAM为0.78。然而,在Cox模型中,种族之间相互作用和GC性能的测试对于转移或PCSM均不显着(均p≥0.3)。结论GC是预后不良的非常有力的预测指标,在AAM和非AAM中均表现良好。我们的数据支持在反相后AAM中使用GC进行风险分层。尽管我们的数据表明,鉴于事件数量有限,GC实际上可以在AAM中更好地工作,但仍需要进一步验证。
更新日期:2019-12-16
中文翻译:
在平等访问医疗机构中,进行根治性前列腺切除术后非裔美国人男性中转移和前列腺癌特异性死亡率的预测的基因组分类器的验证。
背景技术Decipher 22基因基因组分类器(GC)可以帮助根治性前列腺切除术(RP)做出决策,因为它的预后优于单纯的临床病理变量。但是,大多数评估GC的研究对非洲裔美国人(AAM)的代表均不多。我们评估了大型退伍军人事务队列中的GC,并将其性能与CAPRA-S进行了比较,以预测RP后AAM和非AAM的结局。方法1989年至2016年间,对548名前列腺癌(PC)患者进行了GC评分,这些患者在达勒姆退伍军人事务医疗中心接受了RP。这是临床上高危人群,被选择为pT3a,阳性切缘和精囊入侵或接受RP后放疗。使用多变量Cox模型和生存率C指数比较GC和CAPRA-S在预测转移风险和PC特异性死亡率(PCSM)方面的表现。结果中位随访9年,其中37例发生转移,20例因PC死亡。总体而言,有55%(n = 301)的患者为AAM。在多变量分析中,GC(高位vs.中位和中位vs.低位)是所有男性转移的重要预测指标(所有p <0.001)。与之前的研究一致,相对于CAPRA-S,GC的5年转移(0.78 vs. 0.72)和10年PCSM(0.85 vs. 0.81)的C指数更高。有人建议,GC比非AAM更能预测AAM。具体而言,AAM的5年转移风险C指数为0.86,非AAM为0.69,10年PCSM风险C指数在AAM为0.91,而非AAM为0.78。然而,在Cox模型中,种族之间相互作用和GC性能的测试对于转移或PCSM均不显着(均p≥0.3)。结论GC是预后不良的非常有力的预测指标,在AAM和非AAM中均表现良好。我们的数据支持在反相后AAM中使用GC进行风险分层。尽管我们的数据表明,鉴于事件数量有限,GC实际上可以在AAM中更好地工作,但仍需要进一步验证。

























 京公网安备 11010802027423号
京公网安备 11010802027423号