当前位置:
X-MOL 学术
›
JACC Heart Fail.
›
论文详情
Our official English website, www.x-mol.net, welcomes your feedback! (Note: you will need to create a separate account there.)
Diuretic Strategies for Loop Diuretic Resistance in Acute Heart Failure: The 3T Trial.
JACC: Heart Failure ( IF 13.0 ) Pub Date : 2019-12-11 , DOI: 10.1016/j.jchf.2019.09.012 Zachary L Cox 1 , Rebecca Hung 2 , Daniel J Lenihan 3 , Jeffrey M Testani 4
JACC: Heart Failure ( IF 13.0 ) Pub Date : 2019-12-11 , DOI: 10.1016/j.jchf.2019.09.012 Zachary L Cox 1 , Rebecca Hung 2 , Daniel J Lenihan 3 , Jeffrey M Testani 4
Affiliation
|
OBJECTIVES
This study compared combination diuretic strategies in acute heart failure (AHF) complicated by diuretic resistance (DR).
BACKGROUND
Combination diuretic regimens to overcome loop DR are commonly used but with limited evidence.
METHODS
This study was a randomized, double-blinded trial in 60 patients hospitalized with AHF and intravenous (IV) loop DR. Patients were randomized to oral metolazone, IV chlorothiazide, or tolvaptan therapy. All patients received concomitant high-dose IV infusions of furosemide. The primary outcome was 48-h weight loss.
RESULTS
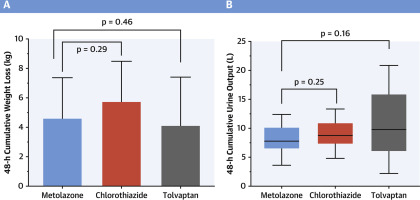
The cohort exhibited DR prior to enrollment, producing 1,188 ± 476 ml of urine in 12 h during high-dose loop diuretic therapy (IV furosemide: 612 ± 439 mg/day). All 3 interventions significantly improved diuretic efficacy (p < 0.001). Compared to metolazone (4.6 ± 2.7 kg), neither IV chlorothiazide (5.8 ± 2.7 kg; 1.2 kg [95% confidence interval [CI]: -2.9 to 0.6; p = 0.292) nor tolvaptan (4.1 ± 3.3 kg; 0.5 kg [95% CI: -1.5 to 2.4; p = 0.456) resulted in more weight loss at 48 h. Median (interquartile range [IQR]) Cumulative urine output increased significantly and did not differ among those receiving metolazone (7.78 [IQR: 6.59 to 10.10] l) and chlorothiazide (8.77 [IQR: 7.37 to 10.86] l; p = 0.245) or tolvaptan (9.70 [IQR: 6.36 to 13.81] l; p = 0.160). Serum sodium decreased less with tolvaptan than with metolazone (+4 ± 5 vs. -1 ± 3 mEq/l; p = 0.001), but 48-h spot urine sodium was lower with tolvaptan (58 ± 25 mmol/l) than with metolazone (104 ± 16 mmol/l; p = 0.002) and with chlorothiazide (117 ± 14 mmol/l; p < 0.001).
CONCLUSIONS
In this moderately sized DR trial, weight loss was excellent with the addition of metolazone, IV chlorothiazide, or tolvaptan to loop diuretics, without a detectable between-group difference. (Comparison of Oral or Intravenous Thiazides vs. tolvaptan in Diuretic Resistant Decompensated Heart Failure [3T]; NCT02606253).
中文翻译:

急性心力衰竭中循环利尿阻力的利尿策略:3T试验。
目的本研究比较了急性心力衰竭(AHF)并发利尿抵抗(DR)的联合利尿策略。背景技术通常使用联合利尿剂方案来克服环DR,但证据有限。方法该研究是一项随机,双盲试验,共60例接受AHF和静脉(IV)回路DR住院治疗的患者。患者被随机分为口服美托拉酮,静脉注射氯噻嗪或托伐普坦治疗。所有患者均接受速尿大剂量静脉输注。主要结果是体重减轻48小时。结果该队列在入组前表现出DR,在大剂量loop利尿剂治疗(IV速尿:612±439 mg /天)期间,在12小时内产生1,188±476 ml尿液。所有3种干预措施均显着提高了利尿剂的疗效(p <0.001)。与美托拉宗(4.6±2.7公斤)相比,IV氯噻嗪(5.8±2.7 kg; 1.2 kg [95%置信区间[CI]:-2.9至0.6; p = 0.292])和托伐普坦(4.1±3.3 kg; 0.5 kg [95%CI:-1.5至2.4; p = 0.456)在48小时时导致更多的体重减轻。中位数(四分位间距[IQR])累积尿量显着增加,接受甲氧氮酮(7.78 [IQR:6.59至10.10] l)和氯噻嗪(8.77 [IQR:7.37至10.86] l; p = 0.245)的患者的尿量无明显差异托伐普坦(9.70 [IQR:6.36至13.81] l; p = 0.160)。托伐普坦的血清钠减少量少于美托拉宗(+4±5 vs. -1±3 mEq / l; p = 0.001),但是托伐普坦48小时点尿钠含量降低(58±25 mmol / l)甲霜灵(104±16 mmol / l; p = 0.002)和氯噻嗪(117±14 mmol / l; p <0.001)。结论在这项中等规模的DR试验中,在环利尿剂中添加甲硝唑,IV氯噻嗪或托伐普坦后,体重减轻效果非常好,而组间无差异。(利尿剂抗失代偿性心力衰竭患者口服或静脉注射噻嗪类药物与托伐普坦的比较[3T]; NCT02606253)。
更新日期:2019-12-11
中文翻译:
急性心力衰竭中循环利尿阻力的利尿策略:3T试验。
目的本研究比较了急性心力衰竭(AHF)并发利尿抵抗(DR)的联合利尿策略。背景技术通常使用联合利尿剂方案来克服环DR,但证据有限。方法该研究是一项随机,双盲试验,共60例接受AHF和静脉(IV)回路DR住院治疗的患者。患者被随机分为口服美托拉酮,静脉注射氯噻嗪或托伐普坦治疗。所有患者均接受速尿大剂量静脉输注。主要结果是体重减轻48小时。结果该队列在入组前表现出DR,在大剂量loop利尿剂治疗(IV速尿:612±439 mg /天)期间,在12小时内产生1,188±476 ml尿液。所有3种干预措施均显着提高了利尿剂的疗效(p <0.001)。与美托拉宗(4.6±2.7公斤)相比,IV氯噻嗪(5.8±2.7 kg; 1.2 kg [95%置信区间[CI]:-2.9至0.6; p = 0.292])和托伐普坦(4.1±3.3 kg; 0.5 kg [95%CI:-1.5至2.4; p = 0.456)在48小时时导致更多的体重减轻。中位数(四分位间距[IQR])累积尿量显着增加,接受甲氧氮酮(7.78 [IQR:6.59至10.10] l)和氯噻嗪(8.77 [IQR:7.37至10.86] l; p = 0.245)的患者的尿量无明显差异托伐普坦(9.70 [IQR:6.36至13.81] l; p = 0.160)。托伐普坦的血清钠减少量少于美托拉宗(+4±5 vs. -1±3 mEq / l; p = 0.001),但是托伐普坦48小时点尿钠含量降低(58±25 mmol / l)甲霜灵(104±16 mmol / l; p = 0.002)和氯噻嗪(117±14 mmol / l; p <0.001)。结论在这项中等规模的DR试验中,在环利尿剂中添加甲硝唑,IV氯噻嗪或托伐普坦后,体重减轻效果非常好,而组间无差异。(利尿剂抗失代偿性心力衰竭患者口服或静脉注射噻嗪类药物与托伐普坦的比较[3T]; NCT02606253)。

























 京公网安备 11010802027423号
京公网安备 11010802027423号