Our official English website, www.x-mol.net, welcomes your feedback! (Note: you will need to create a separate account there.)
Effect of Single-Fraction vs Multifraction Radiotherapy on Ambulatory Status Among Patients With Spinal Canal Compression From Metastatic Cancer
JAMA ( IF 120.7 ) Pub Date : 2019-12-03 , DOI: 10.1001/jama.2019.17913 Peter J Hoskin 1, 2 , Kirsten Hopkins 3 , Vivek Misra 4 , Tanya Holt 5 , Rhona McMenemin 6 , Danny Dubois 7 , Fiona McKinna 8 , Bernadette Foran 9 , Krishnaswamy Madhavan 10 , Carol MacGregor 11 , Andrew Bates 12 , Noelle O'Rourke 13 , Jason F Lester 14 , Tim Sevitt 15 , Daniel Roos 16, 17 , Sanjay Dixit 18 , Gillian Brown 9 , Seonaid Arnott 11 , Sharon Shibu Thomas 10 , Sharon Forsyth 19 , Sandy Beare 19 , Krystyna Reczko 19 , Allan Hackshaw 19 , Andre Lopes 19
JAMA ( IF 120.7 ) Pub Date : 2019-12-03 , DOI: 10.1001/jama.2019.17913 Peter J Hoskin 1, 2 , Kirsten Hopkins 3 , Vivek Misra 4 , Tanya Holt 5 , Rhona McMenemin 6 , Danny Dubois 7 , Fiona McKinna 8 , Bernadette Foran 9 , Krishnaswamy Madhavan 10 , Carol MacGregor 11 , Andrew Bates 12 , Noelle O'Rourke 13 , Jason F Lester 14 , Tim Sevitt 15 , Daniel Roos 16, 17 , Sanjay Dixit 18 , Gillian Brown 9 , Seonaid Arnott 11 , Sharon Shibu Thomas 10 , Sharon Forsyth 19 , Sandy Beare 19 , Krystyna Reczko 19 , Allan Hackshaw 19 , Andre Lopes 19
Affiliation
|
Importance
Malignant spinal canal compression, a major complication of metastatic cancer, is managed with radiotherapy to maintain mobility and relieve pain, although there is no standard radiotherapy regimen. Objective
To evaluate whether single-fraction radiotherapy is noninferior to 5 fractions of radiotherapy. Design, Setting, and Participants
Multicenter noninferiority randomized clinical trial conducted in 42 UK and 5 Australian radiotherapy centers. Eligible patients (n = 686) had metastatic cancer with spinal cord or cauda equina compression, life expectancy greater than 8 weeks, and no previous radiotherapy to the same area. Patients were recruited between February 2008 and April 2016, with final follow-up in September 2017. Interventions
Patients were randomized to receive external beam single-fraction 8-Gy radiotherapy (n = 345) or 20 Gy of radiotherapy in 5 fractions over 5 consecutive days (n = 341). Main Outcomes and Measures
The primary end point was ambulatory status at week 8, based on a 4-point scale and classified as grade 1 (ambulatory without the use of aids and grade 5 of 5 muscle power) or grade 2 (ambulatory using aids or grade 4 of 5 muscle power). The noninferiority margin for the difference in ambulatory status was -11%. Secondary end points included ambulatory status at weeks 1, 4, and 12 and overall survival. Results
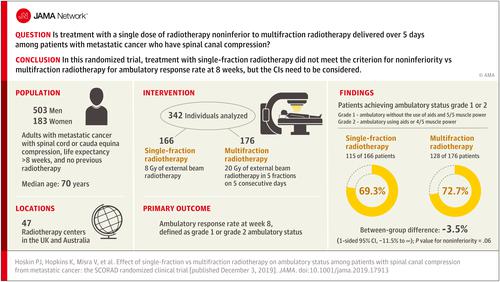
Among 686 randomized patients (median [interquartile range] age, 70 [64-77] years; 503 (73%) men; 44% had prostate cancer, 19% had lung cancer, and 12% had breast cancer), 342 (49.8%) were analyzed for the primary end point (255 patients died before the 8-week assessment). Ambulatory status grade 1 or 2 at week 8 was achieved by 115 of 166 (69.3%) patients in the single-fraction group vs 128 of 176 (72.7%) in the multifraction group (difference, -3.5% [1-sided 95% CI, -11.5% to ∞]; P value for noninferiority = .06). The difference in ambulatory status grade 1 or 2 in the single-fraction vs multifraction group was -0.4% (63.9% vs 64.3%; [1-sided 95% CI, -6.9 to ∞]; P value for noninferiority = .004) at week 1, -0.7% (66.8% vs 67.6%; [1-sided 95% CI, -8.1 to ∞]; P value for noninferiority = .01) at week 4, and 4.1% (71.8% vs 67.7%; [1-sided 95% CI, -4.6 to ∞]; P value for noninferiority = .002) at week 12. Overall survival rates at 12 weeks were 50% in the single-fraction group vs 55% in the multifraction group (stratified hazard ratio, 1.02 [95% CI, 0.74-1.41]). Of the 11 other secondary end points that were analyzed, the between-group differences were not statistically significant or did not meet noninferiority criterion. Conclusions and Relevance
Among patients with malignant metastatic solid tumors and spinal canal compression, a single radiotherapy dose, compared with a multifraction dose delivered over 5 days, did not meet the criterion for noninferiority for the primary outcome (ambulatory at 8 weeks). However, the extent to which the lower bound of the CI overlapped with the noninferiority margin should be considered when interpreting the clinical importance of this finding. Trial Registration
ISRCTN Identifiers: ISRCTN97555949 and ISRCTN97108008.
中文翻译:

单次与多次放疗对转移性癌椎管受压患者行走状态的影响
重要性恶性椎管压迫是转移性癌症的主要并发症,尽管没有标准的放疗方案,但通过放疗来控制以保持活动能力和缓解疼痛。目的评价单次放疗是否不劣于5次放疗。设计、设置和参与者 在 42 个英国和 5 个澳大利亚放射治疗中心进行的多中心非劣效性随机临床试验。符合条件的患者 (n = 686) 患有脊髓或马尾神经受压的转移性癌症,预期寿命超过 8 周,且之前未曾对同一区域进行过放射治疗。患者于 2008 年 2 月至 2016 年 4 月期间招募,最终随访于 2017 年 9 月。干预 患者随机接受外照射单次 8-Gy 放射治疗(n = 345)或连续 5 天分 5 次接受 20 Gy 放射治疗(n = 341)。主要结果和测量 主要终点是第 8 周时的走动状态,基于 4 分制,分为 1 级(不使用辅助设备的走动和 5 级肌肉力量)或 2 级(使用辅助设备或5 级肌肉力量中的 4 级)。动态状态差异的非劣效性边际为-11%。次要终点包括第 1、4 和 12 周的动态状态和总生存期。结果 在 686 名随机患者(中位 [四分位距] 年龄,70 [64-77] 岁;503 名 (73%) 男性;44% 患有前列腺癌,19% 患有肺癌,12% 患有乳腺癌)中,342 ( 49. 8%)的主要终点(255 名患者在 8 周评估前死亡)进行了分析。在第 8 周,单次分割组 166 名患者中有 115 名 (69.3%) 达到 1 级或 2 级动态状态,而多次分割组 176 名患者中有 128 名 (72.7%)(差异,-3.5% [单侧 95%) CI,-11.5% 至 ∞];非劣效性的 P 值 = .06)。单次与多次组的 1 级或 2 级动态状态差异为 -0.4%(63.9% 与 64.3%;[单侧 95% CI,-6.9 至 ∞];非劣效性的 P 值 = .004)在第 1 周时,-0.7%(66.8% 对 67.6%;[单侧 95% CI,-8.1 到∞];非劣效性的 P 值 = .01)和第 4 周时为 4.1%(71.8% 对 67.7%; [单侧 95% CI,-4.6 至 ∞];非劣效性的 P 值 = .002)在第 12 周。12 周时的总生存率在单次组中为 50%,在多次组中为 55%(分层风险比,1.02 [95% CI,0.74-1.41])。在分析的其他 11 个次要终点中,组间差异无统计学意义或不符合非劣效性标准。结论和相关性 在患有恶性转移性实体瘤和椎管压迫的患者中,与超过 5 天的多次放射治疗相比,单一放射治疗剂量不符合主要结果(8 周时走动)的非劣效性标准。然而,在解释这一发现的临床重要性时,应考虑 CI 下限与非劣效性边界重叠的程度。试用注册 ISRCTN 标识符:
更新日期:2019-12-03
中文翻译:
单次与多次放疗对转移性癌椎管受压患者行走状态的影响
重要性恶性椎管压迫是转移性癌症的主要并发症,尽管没有标准的放疗方案,但通过放疗来控制以保持活动能力和缓解疼痛。目的评价单次放疗是否不劣于5次放疗。设计、设置和参与者 在 42 个英国和 5 个澳大利亚放射治疗中心进行的多中心非劣效性随机临床试验。符合条件的患者 (n = 686) 患有脊髓或马尾神经受压的转移性癌症,预期寿命超过 8 周,且之前未曾对同一区域进行过放射治疗。患者于 2008 年 2 月至 2016 年 4 月期间招募,最终随访于 2017 年 9 月。干预 患者随机接受外照射单次 8-Gy 放射治疗(n = 345)或连续 5 天分 5 次接受 20 Gy 放射治疗(n = 341)。主要结果和测量 主要终点是第 8 周时的走动状态,基于 4 分制,分为 1 级(不使用辅助设备的走动和 5 级肌肉力量)或 2 级(使用辅助设备或5 级肌肉力量中的 4 级)。动态状态差异的非劣效性边际为-11%。次要终点包括第 1、4 和 12 周的动态状态和总生存期。结果 在 686 名随机患者(中位 [四分位距] 年龄,70 [64-77] 岁;503 名 (73%) 男性;44% 患有前列腺癌,19% 患有肺癌,12% 患有乳腺癌)中,342 ( 49. 8%)的主要终点(255 名患者在 8 周评估前死亡)进行了分析。在第 8 周,单次分割组 166 名患者中有 115 名 (69.3%) 达到 1 级或 2 级动态状态,而多次分割组 176 名患者中有 128 名 (72.7%)(差异,-3.5% [单侧 95%) CI,-11.5% 至 ∞];非劣效性的 P 值 = .06)。单次与多次组的 1 级或 2 级动态状态差异为 -0.4%(63.9% 与 64.3%;[单侧 95% CI,-6.9 至 ∞];非劣效性的 P 值 = .004)在第 1 周时,-0.7%(66.8% 对 67.6%;[单侧 95% CI,-8.1 到∞];非劣效性的 P 值 = .01)和第 4 周时为 4.1%(71.8% 对 67.7%; [单侧 95% CI,-4.6 至 ∞];非劣效性的 P 值 = .002)在第 12 周。12 周时的总生存率在单次组中为 50%,在多次组中为 55%(分层风险比,1.02 [95% CI,0.74-1.41])。在分析的其他 11 个次要终点中,组间差异无统计学意义或不符合非劣效性标准。结论和相关性 在患有恶性转移性实体瘤和椎管压迫的患者中,与超过 5 天的多次放射治疗相比,单一放射治疗剂量不符合主要结果(8 周时走动)的非劣效性标准。然而,在解释这一发现的临床重要性时,应考虑 CI 下限与非劣效性边界重叠的程度。试用注册 ISRCTN 标识符:
























 京公网安备 11010802027423号
京公网安备 11010802027423号