Our official English website, www.x-mol.net, welcomes your feedback! (Note: you will need to create a separate account there.)
Opioid agonist treatment scale-up and the initiation of injection drug use: A dynamic modeling analysis.
PLOS Medicine ( IF 15.8 ) Pub Date : 2019-11-26 , DOI: 10.1371/journal.pmed.1002973 Charles Marks 1, 2, 3 , Annick Borquez 3 , Sonia Jain 4 , Xiaoying Sun 4 , Steffanie A Strathdee 3 , Richard S Garfein 3 , M-J Milloy 5, 6 , Kora DeBeck 5, 7 , Javier A Cepeda 3 , Dan Werb 3 , Natasha K Martin 3, 8
PLOS Medicine ( IF 15.8 ) Pub Date : 2019-11-26 , DOI: 10.1371/journal.pmed.1002973 Charles Marks 1, 2, 3 , Annick Borquez 3 , Sonia Jain 4 , Xiaoying Sun 4 , Steffanie A Strathdee 3 , Richard S Garfein 3 , M-J Milloy 5, 6 , Kora DeBeck 5, 7 , Javier A Cepeda 3 , Dan Werb 3 , Natasha K Martin 3, 8
Affiliation
|
BACKGROUND
Injection drug use (IDU) is associated with multiple health harms. The vast majority of IDU initiation events (in which injection-naïve persons first adopt IDU) are assisted by a person who injects drugs (PWID), and as such, IDU could be considered as a dynamic behavioral transmission process. Data suggest that opioid agonist treatment (OAT) enrollment is associated with a reduced likelihood of assisting with IDU initiation. We assessed the association between recent OAT enrollment and assisting IDU initiation across several North American settings and used dynamic modeling to project the potential population-level impact of OAT scale-up within the PWID population on IDU initiation.
METHODS AND FINDINGS
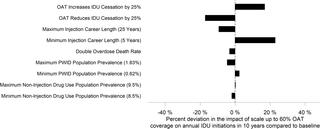
We employed data from a prospective multicohort study of PWID in 3 settings (Vancouver, Canada [n = 1,737]; San Diego, United States [n = 346]; and Tijuana, Mexico [n = 532]) from 2014 to 2017. Site-specific modified Poisson regression models were constructed to assess the association between recent (past 6 month) OAT enrollment and history of ever having assisted an IDU initiation with recently assisting IDU initiation. Findings were then pooled using linear mixed-effects techniques. A dynamic transmission model of IDU among the general population was developed, stratified by known factors associated with assisting IDU initiation and relevant drug use behaviors. The model was parameterized to a generic North American setting (approximately 1% PWID) and used to estimate the impact of increasing OAT coverage among PWID from baseline (approximately 21%) to 40%, 50%, and 60% on annual IDU initiation incidence and corresponding PWID population size across a decade. From Vancouver, San Diego, and Tijuana, respectively, 4.5%, 5.2%, and 4.3% of participants reported recently assisting an IDU initiation, and 49.4%, 19.7%, and 2.1% reported recent enrollment in OAT. Recent OAT enrollment was significantly associated with a 45% lower likelihood of providing recent IDU initiation assistance among PWID (relative risk [RR] 0.55 [95% CI 0.36-0.84], p = 0.006) compared to those not recently on OAT. Our dynamic model predicts a baseline mean of 1,067 (2.5%-97.5% interval [95% I 490-2,082]) annual IDU initiations per 1,000,000 individuals, of which 886 (95% I 406-1,750) are assisted by PWID. Based on our observed statistical associations, our dynamic model predicts that increasing OAT coverage from approximately 21% to 40%, 50%, or 60% among PWID could reduce annual IDU initiations by 11.5% (95% I 2.4-21.7), 17.3% (95% I 5.6-29.4), and 22.8% (95% I 8.1-36.8) and reduce the PWID population size by 5.4% (95% I 0.1-12.0), 8.2% (95% I 2.2-16.9), and 10.9% (95% I 3.2-21.8) relative to baseline, respectively, in a decade. Less impact occurs when the protective effect of OAT is diminished, when a greater proportion of IDU initiations are unassisted by PWID, and when average IDU career length is longer. The study's main limitations are uncertainty in the causal pathway between OAT enrollment and assisting with IDU initiation and the use of a simplified model of IDU initiation.
CONCLUSIONS
In addition to its known benefits on preventing HIV, hepatitis C virus (HCV), and overdose among PWID, our modeling suggests that OAT scale-up may also reduce the number of IDU initiations and PWID population size.
中文翻译:

阿片类激动剂治疗规模扩大和注射药物使用的开始:动态模型分析。
背景技术注射吸毒(IDU)与多种健康危害相关。绝大多数 IDU 起始事件(其中未注射过注射者首次采用 IDU)是由注射吸毒者 (PWID) 协助的,因此,IDU 可以被视为动态行为传播过程。数据表明,阿片类药物激动剂治疗 (OAT) 的入组与协助 IDU 启动的可能性降低相关。我们评估了北美多个地区近期 OAT 注册与协助 IDU 启动之间的关联,并使用动态模型来预测吸毒者人群中 OAT 规模扩大对 IDU 启动的潜在人群影响。方法和结果 我们采用了 2014 年至 3 个地区(加拿大温哥华 [n = 1,737];美国圣地亚哥 [n = 346];和墨西哥蒂华纳 [n = 532])中吸毒者前瞻性多队列研究的数据。 2017 年。构建了特定地点的改良泊松回归模型,以评估最近(过去 6 个月)OAT 注册与曾经协助 IDU 启动的历史与最近协助 IDU 启动之间的关联。然后使用线性混合效应技术汇总研究结果。开发了一般人群中注射吸毒者的动态传播模型,并根据与协助注射吸毒者开始和相关吸毒行为相关的已知因素进行分层。该模型针对一般北美环境(约 1% 注射吸毒者)进行了参数化,并用于估计注射吸毒者中 OAT 覆盖率从基线(约 21%)增加到 40%、50% 和 60% 对每年注射吸毒者起始发生率的影响以及十年内相应的吸毒者人口规模。来自温哥华、圣地亚哥和蒂华纳的参与者分别有 4.5%、5.2% 和 4.3% 报告最近协助了 IDU 启动,49.4%、19.7% 和 2.1% 报告最近参加了 OAT。与近期未参加 OAT 的人群相比,最近参加 OAT 的注射吸毒者中近期提供 IDU 启动援助的可能性显着降低 45%(相对风险 [RR] 0.55 [95% CI 0.36-0.84],p = 0.006)。我们的动态模型预测每 1,000,000 人中每年有 1,067 例(2.5%-97.5% 区间 [95% I 490-2,082])注射吸毒者开始注射,其中 886 例(95% I 406-1,750)得到注射吸毒者的帮助。根据我们观察到的统计关联,我们的动态模型预测,将注射吸毒者中的 OAT 覆盖率从约 21% 提高到 40%、50% 或 60% 可以将每年注射吸毒者的数量减少 11.5% (95% I 2.4-21.7)、17.3% (95% I 5.6-29.4)、22.8% (95% I 8.1-36.8),并将吸毒者人口规模减少 5.4% (95% I 0.1-12.0)、8.2% (95% I 2.2-16.9) 和十年内相对于基线分别下降 10.9% (95% I 3.2-21.8)。当 OAT 的保护作用减弱、较大比例的注射吸毒者开始没有获得注射吸毒者的帮助以及注射吸毒者的平均职业生涯较长时,影响就会较小。该研究的主要局限性是 OAT 登记与协助 IDU 启动之间的因果关系以及使用简化的 IDU 启动模型之间的因果关系。结论 除了已知的预防艾滋病毒、丙型肝炎病毒 (HCV) 和吸毒者过量用药方面的益处外,我们的模型表明,扩大 OAT 规模还可能减少注射吸毒者的数量和吸毒者人口规模。
更新日期:2019-12-03
中文翻译:
阿片类激动剂治疗规模扩大和注射药物使用的开始:动态模型分析。
背景技术注射吸毒(IDU)与多种健康危害相关。绝大多数 IDU 起始事件(其中未注射过注射者首次采用 IDU)是由注射吸毒者 (PWID) 协助的,因此,IDU 可以被视为动态行为传播过程。数据表明,阿片类药物激动剂治疗 (OAT) 的入组与协助 IDU 启动的可能性降低相关。我们评估了北美多个地区近期 OAT 注册与协助 IDU 启动之间的关联,并使用动态模型来预测吸毒者人群中 OAT 规模扩大对 IDU 启动的潜在人群影响。方法和结果 我们采用了 2014 年至 3 个地区(加拿大温哥华 [n = 1,737];美国圣地亚哥 [n = 346];和墨西哥蒂华纳 [n = 532])中吸毒者前瞻性多队列研究的数据。 2017 年。构建了特定地点的改良泊松回归模型,以评估最近(过去 6 个月)OAT 注册与曾经协助 IDU 启动的历史与最近协助 IDU 启动之间的关联。然后使用线性混合效应技术汇总研究结果。开发了一般人群中注射吸毒者的动态传播模型,并根据与协助注射吸毒者开始和相关吸毒行为相关的已知因素进行分层。该模型针对一般北美环境(约 1% 注射吸毒者)进行了参数化,并用于估计注射吸毒者中 OAT 覆盖率从基线(约 21%)增加到 40%、50% 和 60% 对每年注射吸毒者起始发生率的影响以及十年内相应的吸毒者人口规模。来自温哥华、圣地亚哥和蒂华纳的参与者分别有 4.5%、5.2% 和 4.3% 报告最近协助了 IDU 启动,49.4%、19.7% 和 2.1% 报告最近参加了 OAT。与近期未参加 OAT 的人群相比,最近参加 OAT 的注射吸毒者中近期提供 IDU 启动援助的可能性显着降低 45%(相对风险 [RR] 0.55 [95% CI 0.36-0.84],p = 0.006)。我们的动态模型预测每 1,000,000 人中每年有 1,067 例(2.5%-97.5% 区间 [95% I 490-2,082])注射吸毒者开始注射,其中 886 例(95% I 406-1,750)得到注射吸毒者的帮助。根据我们观察到的统计关联,我们的动态模型预测,将注射吸毒者中的 OAT 覆盖率从约 21% 提高到 40%、50% 或 60% 可以将每年注射吸毒者的数量减少 11.5% (95% I 2.4-21.7)、17.3% (95% I 5.6-29.4)、22.8% (95% I 8.1-36.8),并将吸毒者人口规模减少 5.4% (95% I 0.1-12.0)、8.2% (95% I 2.2-16.9) 和十年内相对于基线分别下降 10.9% (95% I 3.2-21.8)。当 OAT 的保护作用减弱、较大比例的注射吸毒者开始没有获得注射吸毒者的帮助以及注射吸毒者的平均职业生涯较长时,影响就会较小。该研究的主要局限性是 OAT 登记与协助 IDU 启动之间的因果关系以及使用简化的 IDU 启动模型之间的因果关系。结论 除了已知的预防艾滋病毒、丙型肝炎病毒 (HCV) 和吸毒者过量用药方面的益处外,我们的模型表明,扩大 OAT 规模还可能减少注射吸毒者的数量和吸毒者人口规模。


























 京公网安备 11010802027423号
京公网安备 11010802027423号