npj Breast Cancer ( IF 5.9 ) Pub Date : 2019-11-08 , DOI: 10.1038/s41523-019-0137-3 Salomon M Stemmer 1, 2 , Mariana Steiner 3 , Shulamith Rizel 1 , Noa Ben-Baruch 4 , Beatrice Uziely 5 , Debbie M Jakubowski 6 , Julie Baron 6 , Steven Shak 6 , Lior Soussan-Gutman 7 , Avital Bareket-Samish 8 , Georgeta Fried 9 , Ora Rosengarten 10 , Amit Itay 11 , Bella Nisenbaum 12 , Daniela Katz 13 , Michelle Leviov 3 , Margarita Tokar 14, 15 , Nicky Liebermann 16 , David B Geffen 14, 15
|
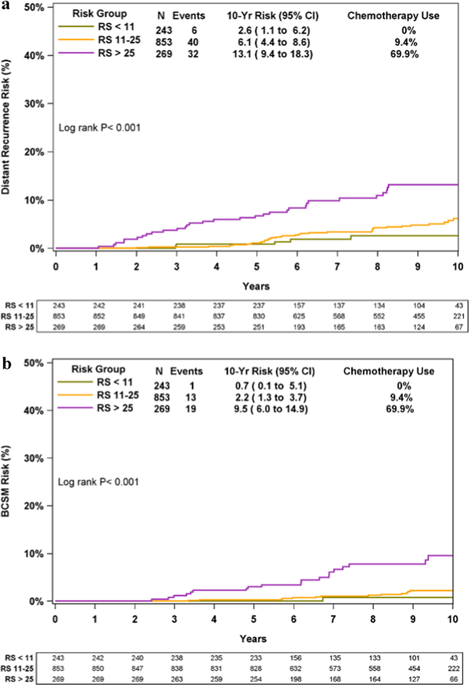
The 21-gene Recurrence Score (RS) assay is a validated prognosticator/predictor of chemotherapy (CT) benefit in early-stage estrogen receptor (ER)-positive breast cancer (BC). Long-term data from real-life clinical practice where treatment was guided by the RS result are lacking. We performed exploratory analysis of the Clalit Health Services (CHS) registry, which included all CHS patients with node-negative ER+ HER2-negative BC who underwent RS testing between 1/2006 and 12/2009 to determine 10-year Kaplan–Meier estimates for distant recurrence/BC-specific mortality (BCSM) in this cohort. The analysis included 1365 patients. Distribution of RS results: RS 0–10, 17.8%; RS 11–25, 62.5%; RS 26–100, 19.7%. Corresponding CT use: 0, 9.4, and 69.9%. Ten-year distant recurrence rates in patients with RS 0–10, 11–25, and 26–100: 2.6% (95% confidence interval [CI], 1.1–6.2%), 6.1% (95% CI, 4.4–8.6%), and 13.1% (95% CI, 9.4–18.3%), respectively (P < 0.001); corresponding BCSM rates: 0.7% (95% CI 0.1–5.1%), 2.2% (95% CI, 1.3–3.7%), and 9.5% (95% CI, 6.0–14.9%) (P < 0.001). When the analysis included patients treated with endocrine therapy alone (95.5/87.5% of patients with RS 0–10/11–25), 10-year distant recurrence and BCSM rates for RS 0–10 patients were 2.7% (95% CI, 1.1–6.5%) and 0.8% (95% CI, 0.1–5.3%), respectively, and for RS 11–25 patients, 5.7% (95% CI, 3.9–8.3%) and 2.0% (95% CI, 1.1–3.7%), respectively. For RS 11–25 patients, no statistically significant differences were observed in 10-year distant recurrence/BCSM rates between CT-treated and untreated patients; however, this should be interpreted cautiously since the number of events was low and patients were not randomized. In conclusion, in node-negative ER+ HER2-negative BC patients, where treatment decisions in real-life clinical practice incorporated the RS, patients with RS 0–25 (~80% of patients, <10% CT use) had excellent outcomes at 10 years. Patients with RS 26–100 had high distant recurrence risk despite CT use and are candidates for new treatment approaches.
中文翻译:
采用复发评分引导治疗的 N0 ER+ 乳腺癌患者的十年临床结果
21 基因复发评分 (RS) 测定是早期雌激素受体 (ER) 阳性乳腺癌 (BC) 化疗 (CT) 获益的经过验证的预后/预测指标。缺乏以 RS 结果指导治疗的现实临床实践的长期数据。我们对 Clalit 健康服务 (CHS) 登记处进行了探索性分析,其中包括所有在 2006 年 1 月至 2009 年 12 月期间接受 RS 检测的淋巴结阴性 ER+ HER2 阴性 BC 的 CHS 患者,以确定 10 年 Kaplan-Meier 估计值该队列中的远处复发/BC 特异性死亡率 (BCSM)。该分析包括 1365 名患者。RS结果分布:RS 0-10,17.8%;RS 11–25, 62.5%;RS 26–100,19.7%。相应的 CT 使用:0、9.4 和 69.9%。RS 0-10、11-25 和 26-100 患者的十年远处复发率:2.6%(95% 置信区间 [CI],1.1-6.2%)、6.1%(95% CI,4.4-8.6) %)和 13.1%(95% CI,9.4–18.3%)(P < 0.001);相应的 BCSM 率:0.7% (95% CI 0.1–5.1%)、2.2% (95% CI, 1.3–3.7%) 和 9.5% (95% CI, 6.0–14.9%) ( P < 0.001 ) 。当分析包括仅接受内分泌治疗的患者(RS 0-10/11-25 的患者中 95.5/87.5%)时,RS 0-10 患者的 10 年远处复发率和 BCSM 率为 2.7%(95% CI,分别为 1.1–6.5%)和 0.8%(95% CI,0.1–5.3%),对于 RS 11–25 患者,分别为 5.7%(95% CI,3.9–8.3%)和 2.0%(95% CI,1.1) –3.7%)。对于RS 11-25患者,CT治疗和未治疗患者之间的10年远处复发/BCSM率没有观察到统计学上的显着差异;然而,应谨慎解释这一点,因为事件数量较少且患者未随机分组。总之,在淋巴结阴性 ER+ HER2 阴性 BC 患者中,现实临床实践中的治疗决策结合了 RS,RS 0-25 的患者(约 80% 的患者,<10% CT 使用)在10年。尽管使用了 CT,RS 26-100 的患者仍具有较高的远处复发风险,并且是新治疗方法的候选者。


























 京公网安备 11010802027423号
京公网安备 11010802027423号