当前位置:
X-MOL 学术
›
Hypertens. Res.
›
论文详情
Our official English website, www.x-mol.net, welcomes your feedback! (Note: you will need to create a separate account there.)
Interpreting stimulated plasma renin and aldosterone to select physiologically individualized therapy for resistant hypertension: importance of the class of stimulating drugs
Hypertension Research ( IF 5.4 ) Pub Date : 2019-09-27 , DOI: 10.1038/s41440-019-0327-2 Xiao Huang 1 , Junpei Li 1 , Lishun Liu 2 , Guangliang Chen 3 , Yingping Yi 4 , Ping Li 1 , Yanqing Wu 1 , Yuan Xu 4 , Huihui Bao 1 , Lianbao Yu 5 , Xianhui Qin 6 , Yan Zhang 7 , Binyan Wang 8 , Jianping Li 7 , Fan Fan Hou 6 , Yong Huo 7 , Xiaoshu Cheng 1 , J David Spence 9
Hypertension Research ( IF 5.4 ) Pub Date : 2019-09-27 , DOI: 10.1038/s41440-019-0327-2 Xiao Huang 1 , Junpei Li 1 , Lishun Liu 2 , Guangliang Chen 3 , Yingping Yi 4 , Ping Li 1 , Yanqing Wu 1 , Yuan Xu 4 , Huihui Bao 1 , Lianbao Yu 5 , Xianhui Qin 6 , Yan Zhang 7 , Binyan Wang 8 , Jianping Li 7 , Fan Fan Hou 6 , Yong Huo 7 , Xiaoshu Cheng 1 , J David Spence 9
Affiliation
|
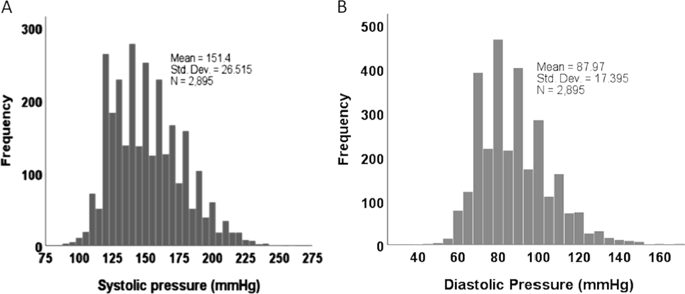
In the treatment of resistant hypertension, physiologically individualized therapy based on phenotyping with plasma renin activity (PRA) and plasma aldosterone significantly improves blood pressure control. Patients with a low-renin/low aldosterone (Liddle) phenotype respond best to amiloride, while those with low-renin/high aldosterone respond best to aldosterone antagonists, and those with high renin/high aldosterone (renal phenotype) respond best to angiotensin receptor blockers (ARB). However, it is important to measure PRA in a stimulated condition to distinguish between low levels due to high salt intake, licorice or nonsteroidal inflammatory drugs and low levels due to suppression by excess aldosterone secretion or renal tubular genetic variants causing retention of salt and water (Liddle phenotype). In the past, both diuretics and angiotensin converting inhibitors (ACEi) have been used for this purpose, and it has been assumed that these classes of drugs are equivalent. In this study of 2896 patients with hypertension, we evaluated that assumption. We found important differences among diuretics alone, ACEi/ARB alone, and ACEi/ARB + diuretics, which all stimulated PRA. However, ACEi/ARB lowers plasma aldosterone, and beta blockers lower PRA. Among patients with systolic pressure ≥ 180 mmHg ± diastolic pressure ≥ 100 mmHg stimulated only by diuretics, the phenotypes were 25% Liddle, 38% IA, 8.7% renal, and 28.3% mixed. In choosing physiologically individualized therapy based on PRA and aldosterone, it is important to consider the classes of stimulating drugs. Phenotypes are best distinguished by taking into account the aldosterone/PRA ratio in addition to the levels of PRA and aldosterone.
中文翻译:

解释刺激的血浆肾素和醛固酮以选择针对难治性高血压的生理个体化治疗:刺激药物类别的重要性
在顽固性高血压的治疗中,基于血浆肾素活性 (PRA) 和血浆醛固酮表型的生理个体化治疗可显着改善血压控制。低肾素/低醛固酮(Liddle)表型的患者对阿米洛利的反应最好,而低肾素/高醛固酮的患者对醛固酮拮抗剂的反应最好,而高肾素/高醛固酮(肾表型)的患者对血管紧张素受体的反应最好阻滞剂(ARB)。然而,重要的是在刺激条件下测量 PRA,以区分由于高盐摄入、甘草或非甾体类炎症药物导致的低水平和由于醛固酮分泌过多或肾小管遗传变异导致盐和水潴留而导致的低水平。 Liddle 表型)。在过去,利尿剂和血管紧张素转换抑制剂 (ACEi) 都已用于此目的,并且假定这几类药物是等效的。在这项对 2896 名高血压患者的研究中,我们评估了这一假设。我们发现单独使用利尿剂、单独使用 ACEi/ARB 和 ACEi/ARB + 利尿剂之间存在重要差异,它们都刺激了 PRA。然而,ACEi/ARB 降低血浆醛固酮,而 β 受体阻滞剂降低 PRA。在仅由利尿剂刺激的收缩压 ≥ 180 mmHg ± 舒张压 ≥ 100 mmHg 的患者中,表型为 25% Liddle、38% IA、8.7% 肾和 28.3% 混合。在选择基于 PRA 和醛固酮的生理个体化治疗时,重要的是要考虑刺激药物的类别。
更新日期:2019-09-27
中文翻译:
解释刺激的血浆肾素和醛固酮以选择针对难治性高血压的生理个体化治疗:刺激药物类别的重要性
在顽固性高血压的治疗中,基于血浆肾素活性 (PRA) 和血浆醛固酮表型的生理个体化治疗可显着改善血压控制。低肾素/低醛固酮(Liddle)表型的患者对阿米洛利的反应最好,而低肾素/高醛固酮的患者对醛固酮拮抗剂的反应最好,而高肾素/高醛固酮(肾表型)的患者对血管紧张素受体的反应最好阻滞剂(ARB)。然而,重要的是在刺激条件下测量 PRA,以区分由于高盐摄入、甘草或非甾体类炎症药物导致的低水平和由于醛固酮分泌过多或肾小管遗传变异导致盐和水潴留而导致的低水平。 Liddle 表型)。在过去,利尿剂和血管紧张素转换抑制剂 (ACEi) 都已用于此目的,并且假定这几类药物是等效的。在这项对 2896 名高血压患者的研究中,我们评估了这一假设。我们发现单独使用利尿剂、单独使用 ACEi/ARB 和 ACEi/ARB + 利尿剂之间存在重要差异,它们都刺激了 PRA。然而,ACEi/ARB 降低血浆醛固酮,而 β 受体阻滞剂降低 PRA。在仅由利尿剂刺激的收缩压 ≥ 180 mmHg ± 舒张压 ≥ 100 mmHg 的患者中,表型为 25% Liddle、38% IA、8.7% 肾和 28.3% 混合。在选择基于 PRA 和醛固酮的生理个体化治疗时,重要的是要考虑刺激药物的类别。

























 京公网安备 11010802027423号
京公网安备 11010802027423号