Our official English website, www.x-mol.net, welcomes your feedback! (Note: you will need to create a separate account there.)
Association Between Dialysis Facility Ownership and Access to Kidney Transplantation
JAMA ( IF 120.7 ) Pub Date : 2019-09-10 , DOI: 10.1001/jama.2019.12803 Jennifer C Gander 1 , Xingyu Zhang 2 , Katherine Ross 3, 4 , Adam S Wilk 5 , Laura McPherson 3 , Teri Browne 6 , Stephen O Pastan 7 , Elizabeth Walker 3 , Zhensheng Wang 3, 8 , Rachel E Patzer 3, 4, 8
JAMA ( IF 120.7 ) Pub Date : 2019-09-10 , DOI: 10.1001/jama.2019.12803 Jennifer C Gander 1 , Xingyu Zhang 2 , Katherine Ross 3, 4 , Adam S Wilk 5 , Laura McPherson 3 , Teri Browne 6 , Stephen O Pastan 7 , Elizabeth Walker 3 , Zhensheng Wang 3, 8 , Rachel E Patzer 3, 4, 8
Affiliation
|
Importance
For-profit (vs nonprofit) dialysis facilities have historically had lower kidney transplantation rates, but it is unknown if the pattern holds for living donor and deceased donor kidney transplantation, varies by facility ownership, or has persisted over time in a nationally representative population. Objective
To determine the association between dialysis facility ownership and placement on the deceased donor kidney transplantation waiting list, receipt of a living donor kidney transplant, or receipt of a deceased donor kidney transplant. Design, Setting, and Participants
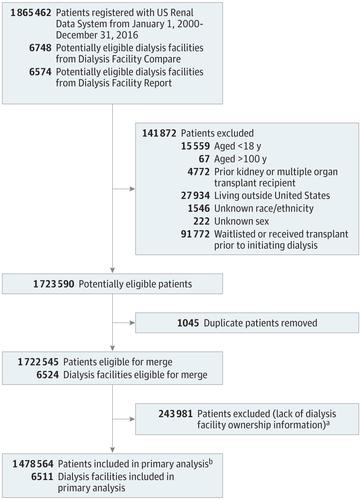
Retrospective cohort study that included 1 478 564 patients treated at 6511 US dialysis facilities. Adult patients with incident end-stage kidney disease from the US Renal Data System (2000-2016) were linked with facility ownership (Dialysis Facility Compare) and characteristics (Dialysis Facility Report). Exposures
The primary exposure was dialysis facility ownership, which was categorized as nonprofit small chains, nonprofit independent facilities, for-profit large chains (>1000 facilities), for-profit small chains (<1000 facilities), and for-profit independent facilities. Main Outcomes and Measures
Access to kidney transplantation was defined as time from initiation of dialysis to placement on the deceased donor kidney transplantation waiting list, receipt of a living donor kidney transplant, or receipt of a deceased donor kidney transplant. Cumulative incidence differences and multivariable Cox models assessed the association between dialysis facility ownership and each outcome. Results
Among 1 478 564 patients, the median age was 66 years (interquartile range, 55-76 years), with 55.3% male, and 28.1% non-Hispanic black patients. Eighty-seven percent of patients received care at a for-profit dialysis facility. A total of 109 030 patients (7.4%) received care at 435 nonprofit small chain facilities; 78 287 (5.3%) at 324 nonprofit independent facilities; 483 988 (32.7%) at 2239 facilities of large for-profit chain 1; 482 689 (32.6%) at 2082 facilities of large for-profit chain 2; 225 890 (15.3%) at 997 for-profit small chain facilities; and 98 680 (6.7%) at 434 for-profit independent facilities. During the study period, 121 680 patients (8.2%) were placed on the deceased donor waiting list, 23 762 (1.6%) received a living donor kidney transplant, and 49 290 (3.3%) received a deceased donor kidney transplant. For-profit facilities had lower 5-year cumulative incidence differences for each outcome vs nonprofit facilities (deceased donor waiting list: -13.2% [95% CI, -13.4% to -13.0%]; receipt of a living donor kidney transplant: -2.3% [95% CI, -2.4% to -2.3%]; and receipt of a deceased donor kidney transplant: -4.3% [95% CI, -4.4% to -4.2%]). Adjusted Cox analyses showed lower relative rates for each outcome among patients treated at all for-profit vs all nonprofit dialysis facilities: deceased donor waiting list (hazard ratio [HR], 0.36 [95% CI, 0.35 to 0.36]); receipt of a living donor kidney transplant (HR, 0.52 [95% CI, 0.51 to 0.54]); and receipt of a deceased donor kidney transplant (HR, 0.44 [95% CI, 0.44 to 0.45]). Conclusions and Relevance
Among US patients with end-stage kidney disease, receiving dialysis at for-profit facilities compared with nonprofit facilities was associated with a lower likelihood of accessing kidney transplantation. Further research is needed to understand the mechanisms behind this association.
中文翻译:

透析设施所有权与肾脏移植机会之间的关联
重要性 营利性(与非营利性)透析设施历来具有较低的肾移植率,但尚不清楚该模式是否适用于活体和已故供体肾移植,因设施所有权而异,还是在具有全国代表性的人群中持续存在. 目的 确定透析设施的所有权与已故供肾移植等候名单、接受活体供肾移植或接受已故供肾移植之间的关联。设计、设置和参与者 回顾性队列研究包括在美国 6511 家透析机构接受治疗的 1478564 名患者。来自美国肾脏数据系统(2000-2016)的终末期肾病成年患者与设施所有权(透析设施比较)和特征(透析设施报告)相关联。暴露 主要暴露是透析设施所有权,分为非营利性小型连锁店、非营利性独立设施、营利性大型连锁店(>1000 个设施)、营利性小型连锁店(<1000 个设施)和营利性独立设施。主要结果和措施 获得肾移植的定义为从开始透析到进入已故供肾移植等候名单、接受活体供肾移植或接受已故供肾移植的时间。累积发生率差异和多变量 Cox 模型评估了透析设施所有权与每个结果之间的关联。结果在1 478 564例患者中,中位年龄为66岁(四分位距,55-76岁),男性占55.3%,非西班牙裔黑人占28.1%。87% 的患者在营利性透析机构接受治疗。共有 109 030 名患者 (7.4%) 在 435 家非营利性小型连锁机构接受治疗;78 287 (5.3%) 在 324 个非营利性独立机构;483 988 (32.7%) 在大型营利性连锁店 1 的 2239 个设施;482 689 (32.6%) 在大型营利性连锁店 2 的 2082 个设施;225 890 (15.3%) 在 997 家营利性小型连锁设施;和 98 680 (6.7%) 在 434 个营利性独立设施。在研究期间,121 680 名患者 (8. 2%) 被列入已故供体等候名单,23 762 (1.6%) 人接受了活体供肾移植,49 290 (3.3%) 接受了已故供肾移植。与非营利机构相比,营利性机构的每个结果的 5 年累积发生率差异较低(已故捐赠者等候名单:-13.2% [95% CI,-13.4% 至 -13.0%];接受活体肾移植:- 2.3% [95% CI,-2.4% 至 -2.3%];接受已故供肾移植:-4.3% [95% CI,-4.4% 至 -4.2%])。调整后的 Cox 分析显示,在所有营利性透析机构与所有非营利性透析机构接受治疗的患者中,每种结果的相对发生率较低:已故捐赠者等候名单(风险比 [HR],0.36 [95% CI,0.35 至 0.36]);接受活体供肾移植(HR,0.52 [95% CI,0.51 至 0.54]);接受已故供肾移植(HR,0.44 [95% CI,0.44 至 0.45])。结论和相关性 在患有终末期肾病的美国患者中,与非营利机构相比,在营利机构接受透析与接受肾移植的可能性较低相关。需要进一步研究以了解这种关联背后的机制。
更新日期:2019-09-10
中文翻译:
透析设施所有权与肾脏移植机会之间的关联
重要性 营利性(与非营利性)透析设施历来具有较低的肾移植率,但尚不清楚该模式是否适用于活体和已故供体肾移植,因设施所有权而异,还是在具有全国代表性的人群中持续存在. 目的 确定透析设施的所有权与已故供肾移植等候名单、接受活体供肾移植或接受已故供肾移植之间的关联。设计、设置和参与者 回顾性队列研究包括在美国 6511 家透析机构接受治疗的 1478564 名患者。来自美国肾脏数据系统(2000-2016)的终末期肾病成年患者与设施所有权(透析设施比较)和特征(透析设施报告)相关联。暴露 主要暴露是透析设施所有权,分为非营利性小型连锁店、非营利性独立设施、营利性大型连锁店(>1000 个设施)、营利性小型连锁店(<1000 个设施)和营利性独立设施。主要结果和措施 获得肾移植的定义为从开始透析到进入已故供肾移植等候名单、接受活体供肾移植或接受已故供肾移植的时间。累积发生率差异和多变量 Cox 模型评估了透析设施所有权与每个结果之间的关联。结果在1 478 564例患者中,中位年龄为66岁(四分位距,55-76岁),男性占55.3%,非西班牙裔黑人占28.1%。87% 的患者在营利性透析机构接受治疗。共有 109 030 名患者 (7.4%) 在 435 家非营利性小型连锁机构接受治疗;78 287 (5.3%) 在 324 个非营利性独立机构;483 988 (32.7%) 在大型营利性连锁店 1 的 2239 个设施;482 689 (32.6%) 在大型营利性连锁店 2 的 2082 个设施;225 890 (15.3%) 在 997 家营利性小型连锁设施;和 98 680 (6.7%) 在 434 个营利性独立设施。在研究期间,121 680 名患者 (8. 2%) 被列入已故供体等候名单,23 762 (1.6%) 人接受了活体供肾移植,49 290 (3.3%) 接受了已故供肾移植。与非营利机构相比,营利性机构的每个结果的 5 年累积发生率差异较低(已故捐赠者等候名单:-13.2% [95% CI,-13.4% 至 -13.0%];接受活体肾移植:- 2.3% [95% CI,-2.4% 至 -2.3%];接受已故供肾移植:-4.3% [95% CI,-4.4% 至 -4.2%])。调整后的 Cox 分析显示,在所有营利性透析机构与所有非营利性透析机构接受治疗的患者中,每种结果的相对发生率较低:已故捐赠者等候名单(风险比 [HR],0.36 [95% CI,0.35 至 0.36]);接受活体供肾移植(HR,0.52 [95% CI,0.51 至 0.54]);接受已故供肾移植(HR,0.44 [95% CI,0.44 至 0.45])。结论和相关性 在患有终末期肾病的美国患者中,与非营利机构相比,在营利机构接受透析与接受肾移植的可能性较低相关。需要进一步研究以了解这种关联背后的机制。

























 京公网安备 11010802027423号
京公网安备 11010802027423号