Our official English website, www.x-mol.net, welcomes your feedback! (Note: you will need to create a separate account there.)
Mechanical and oral antibiotic bowel preparation versus no bowel preparation for elective colectomy (MOBILE): a multicentre, randomised, parallel, single-blinded trial.
The Lancet ( IF 168.9 ) Pub Date : 2019-08-08 , DOI: 10.1016/s0140-6736(19)31269-3 Laura Koskenvuo 1 , Taru Lehtonen 1 , Selja Koskensalo 1 , Suvi Rasilainen 1 , Kai Klintrup 2 , Anu Ehrlich 3 , Tarja Pinta 4 , Tom Scheinin 1 , Ville Sallinen 1
The Lancet ( IF 168.9 ) Pub Date : 2019-08-08 , DOI: 10.1016/s0140-6736(19)31269-3 Laura Koskenvuo 1 , Taru Lehtonen 1 , Selja Koskensalo 1 , Suvi Rasilainen 1 , Kai Klintrup 2 , Anu Ehrlich 3 , Tarja Pinta 4 , Tom Scheinin 1 , Ville Sallinen 1
Affiliation
|
BACKGROUND
Decreased surgical site infections (SSIs) and morbidity have been reported with mechanical and oral antibiotic bowel preparation (MOABP) compared with no bowel preparation (NBP) in colonic surgery. Several societies have recommended routine use of MOABP in patients undergoing colon resection on the basis of these data. Our aim was to investigate this recommendation in a prospective randomised context.
METHODS
In this multicentre, parallel, single-blinded trial, patients undergoing colon resection were randomly assigned (1:1) to either MOABP or NBP in four hospitals in Finland, using a web-based randomisation technique. Randomly varying block sizes (four, six, and eight) were used for randomisation, and stratification was done according to centre. The recruiters, treating physicians, operating surgeons, data collectors, and analysts were masked to the allocated treatment. Key exclusion criteria were need for emergency surgery; bowel obstruction; colonoscopy planned during surgery; allergy to polyethylene glycol, neomycin, or metronidazole; and age younger than 18 years or older than 95 years. Study nurses opened numbered opaque envelopes containing the patient allocated group, and instructed the patients according to the allocation group to either prepare the bowel, or not prepare the bowel. Patients allocated to MOABP prepared their bowel by drinking 2 L of polyethylene glycol and 1 L of clear fluid before 6 pm on the day before surgery and took 2 g of neomycin orally at 7 pm and 2 g of metronidazole orally at 11 pm the day before surgery. The primary outcome was SSI within 30 days after surgery, analysed in the modified intention-to-treat population (all patients who were randomly allocated to and underwent elective colon resection with an anastomosis) along with safety analyses. The trial is registered with ClinicalTrials.gov, NCT02652637, and EudraCT, 2015-004559-38, and is closed to new participants.
FINDINGS
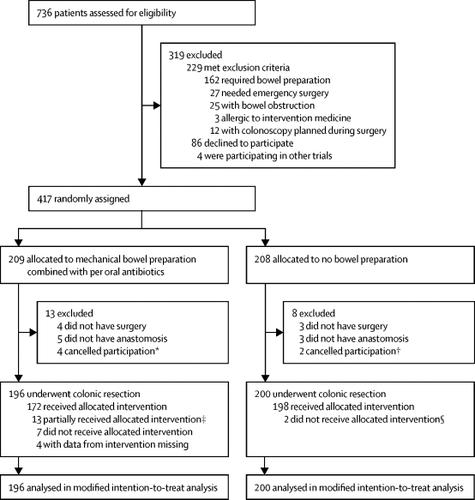
Between March 17, 2016, and Aug 20, 2018, 738 patients were assessed for eligibility. Of the 417 patients who were randomised (209 to MOABP and 208 to NBP), 13 in the MOABP group and eight in the NBP were excluded before undergoing colonic resection; therefore, the modified intention-to-treat analysis included 396 patients (196 for MOABP and 200 for NBP). SSI was detected in 13 (7%) of 196 patients randomised to MOABP, and in 21 (11%) of 200 patients randomised to NBP (odds ratio 1·65, 95% CI 0·80-3·40; p=0·17). Anastomotic dehiscence was reported in 7 (4%) of 196 patients in the MOABP group and in 8 (4%) of 200 in the NBP group, and reoperations were necessary in 16 (8%) of 196 compared with 13 (7%) of 200 patients. Two patients died in the NBP group and none in the MOABP group within 30 days.
INTERPRETATION
MOABP does not reduce SSIs or the overall morbidity of colon surgery compared with NBP. We therefore propose that the current recommendations of using MOABP for colectomies to reduce SSIs or morbidity should be reconsidered.
FUNDING
Vatsatautien Tutkimussäätiö Foundation, Mary and Georg Ehrnrooth's Foundation, and Helsinki University Hospital research funds.
中文翻译:

机械和口服抗生素肠道准备与非肠道准备的选择性结肠切除术(MOBILE):一项多中心,随机,平行,单盲试验。
背景技术在结肠手术中,与不使用肠道准备液(NBP)相比,机械和口服抗生素肠道准备液(MOABP)的手术部位感染(SSIs)和发病率有所降低。根据这些数据,一些学会建议在行结肠切除术的患者中常规使用MOABP。我们的目的是在前瞻性随机背景下研究此建议。方法在这项多中心,平行,单盲试验中,采用基于网络的随机技术,在芬兰的四家医院中,将接受结肠切除术的患者随机分配(1:1)到MOABP或NBP中。使用随机变化的块大小(四个,六个和八个)进行随机化,并根据中心进行分层。招募人员,主治医师,手术外科医生,数据收集者,分析师被掩盖了分配的待遇。主要的排除标准是急诊手术的需要;肠梗阻 计划在手术期间进行结肠镜检查;对聚乙二醇,新霉素或甲硝唑过敏;且年龄小于18岁或大于95岁。研究护士打开了包含患者分配组的编号不透明信封,并根据分配组指示患者准备肠或不准备肠。分配至MOABP的患者在手术前一天的下午6点之前喝了2 L的聚乙二醇和1 L的清液来准备肠道,并在前一天的7 pm口服了2 g的新霉素和在前一天的11 pm口服了2 g的甲硝唑。外科手术。主要结果是手术后30天内出现SSI,在改良的意向性治疗人群(所有患者中随机分配并接受了吻合术并进行选择性结肠切除术的患者)进行了分析,并进行了安全性分析。该试验已在ClinicalTrials.gov,NCT02652637和EudraCT进行了注册,2015-004559-38,并且不对新参与者开放。结果在2016年3月17日至2018年8月20日之间,评估了738例患者的资格。在417例随机分组的患者中(209例为MOABP,208例为NBP),MOABP组中的13例和NBP中的8例在进行结肠切除之前被排除在外;因此,修改后的意向治疗分析包括396例患者(MOABP为196例,NBP为200例)。随机分为MOABP的196例患者中有13例(7%),随机分为NBP的200例中有21例(11%)(赔率1·65,95%CI 0·80-3·40; p = 0 ·17)。据报道,MOABP组196例患者中有7例(4%)吻合口裂,而NBP组200例中有8例(4%)吻合口裂,196例中有16例(8%)需要再次手术,而13例(7%) 200名患者。在30天内,NBP组有2例患者死亡,MOABP组无1例死亡。与NBP相比,MOABP不能降低SSI或结肠手术的整体发病率。因此,我们建议应重新考虑当前使用MOABP进行Colectomies减少SSI或发病率的建议。基金VatsatautienTutkimussäätiö基金会,Mary and Georg Ehrnrooth基金会和赫尔辛基大学医院研究基金。196例中有16例(8%)需要再次手术,而200例中有13例(7%)需要再次手术。在30天内,NBP组有2例患者死亡,MOABP组无1例死亡。与NBP相比,MOABP不能降低SSI或结肠手术的整体发病率。因此,我们建议应重新考虑当前使用MOABP进行Colectomies减少SSI或发病率的建议。基金VatsatautienTutkimussäätiö基金会,Mary and Georg Ehrnrooth基金会和赫尔辛基大学医院研究基金。196例中有16例(8%)需要再次手术,而200例中有13例(7%)需要再次手术。在30天内,NBP组有2例患者死亡,MOABP组无1例死亡。与NBP相比,MOABP不能降低SSI或结肠手术的整体发病率。因此,我们建议应重新考虑当前使用MOABP进行Colectomies减少SSI或发病率的建议。基金VatsatautienTutkimussäätiö基金会,Mary and Georg Ehrnrooth基金会和赫尔辛基大学医院研究基金。因此,我们建议应重新考虑当前使用MOABP进行Colectomies减少SSI或发病率的建议。基金VatsatautienTutkimussäätiö基金会,Mary and Georg Ehrnrooth基金会和赫尔辛基大学医院研究基金。因此,我们建议应重新考虑当前使用MOABP进行Colectomies减少SSI或发病率的建议。基金VatsatautienTutkimussäätiö基金会,Mary and Georg Ehrnrooth基金会和赫尔辛基大学医院研究基金。
更新日期:2019-09-06
中文翻译:
机械和口服抗生素肠道准备与非肠道准备的选择性结肠切除术(MOBILE):一项多中心,随机,平行,单盲试验。
背景技术在结肠手术中,与不使用肠道准备液(NBP)相比,机械和口服抗生素肠道准备液(MOABP)的手术部位感染(SSIs)和发病率有所降低。根据这些数据,一些学会建议在行结肠切除术的患者中常规使用MOABP。我们的目的是在前瞻性随机背景下研究此建议。方法在这项多中心,平行,单盲试验中,采用基于网络的随机技术,在芬兰的四家医院中,将接受结肠切除术的患者随机分配(1:1)到MOABP或NBP中。使用随机变化的块大小(四个,六个和八个)进行随机化,并根据中心进行分层。招募人员,主治医师,手术外科医生,数据收集者,分析师被掩盖了分配的待遇。主要的排除标准是急诊手术的需要;肠梗阻 计划在手术期间进行结肠镜检查;对聚乙二醇,新霉素或甲硝唑过敏;且年龄小于18岁或大于95岁。研究护士打开了包含患者分配组的编号不透明信封,并根据分配组指示患者准备肠或不准备肠。分配至MOABP的患者在手术前一天的下午6点之前喝了2 L的聚乙二醇和1 L的清液来准备肠道,并在前一天的7 pm口服了2 g的新霉素和在前一天的11 pm口服了2 g的甲硝唑。外科手术。主要结果是手术后30天内出现SSI,在改良的意向性治疗人群(所有患者中随机分配并接受了吻合术并进行选择性结肠切除术的患者)进行了分析,并进行了安全性分析。该试验已在ClinicalTrials.gov,NCT02652637和EudraCT进行了注册,2015-004559-38,并且不对新参与者开放。结果在2016年3月17日至2018年8月20日之间,评估了738例患者的资格。在417例随机分组的患者中(209例为MOABP,208例为NBP),MOABP组中的13例和NBP中的8例在进行结肠切除之前被排除在外;因此,修改后的意向治疗分析包括396例患者(MOABP为196例,NBP为200例)。随机分为MOABP的196例患者中有13例(7%),随机分为NBP的200例中有21例(11%)(赔率1·65,95%CI 0·80-3·40; p = 0 ·17)。据报道,MOABP组196例患者中有7例(4%)吻合口裂,而NBP组200例中有8例(4%)吻合口裂,196例中有16例(8%)需要再次手术,而13例(7%) 200名患者。在30天内,NBP组有2例患者死亡,MOABP组无1例死亡。与NBP相比,MOABP不能降低SSI或结肠手术的整体发病率。因此,我们建议应重新考虑当前使用MOABP进行Colectomies减少SSI或发病率的建议。基金VatsatautienTutkimussäätiö基金会,Mary and Georg Ehrnrooth基金会和赫尔辛基大学医院研究基金。196例中有16例(8%)需要再次手术,而200例中有13例(7%)需要再次手术。在30天内,NBP组有2例患者死亡,MOABP组无1例死亡。与NBP相比,MOABP不能降低SSI或结肠手术的整体发病率。因此,我们建议应重新考虑当前使用MOABP进行Colectomies减少SSI或发病率的建议。基金VatsatautienTutkimussäätiö基金会,Mary and Georg Ehrnrooth基金会和赫尔辛基大学医院研究基金。196例中有16例(8%)需要再次手术,而200例中有13例(7%)需要再次手术。在30天内,NBP组有2例患者死亡,MOABP组无1例死亡。与NBP相比,MOABP不能降低SSI或结肠手术的整体发病率。因此,我们建议应重新考虑当前使用MOABP进行Colectomies减少SSI或发病率的建议。基金VatsatautienTutkimussäätiö基金会,Mary and Georg Ehrnrooth基金会和赫尔辛基大学医院研究基金。因此,我们建议应重新考虑当前使用MOABP进行Colectomies减少SSI或发病率的建议。基金VatsatautienTutkimussäätiö基金会,Mary and Georg Ehrnrooth基金会和赫尔辛基大学医院研究基金。因此,我们建议应重新考虑当前使用MOABP进行Colectomies减少SSI或发病率的建议。基金VatsatautienTutkimussäätiö基金会,Mary and Georg Ehrnrooth基金会和赫尔辛基大学医院研究基金。


























 京公网安备 11010802027423号
京公网安备 11010802027423号