Journal of Hepatology ( IF 25.7 ) Pub Date : 2023-04-23 , DOI: 10.1016/j.jhep.2023.04.006 Rakhi Maiwall 1 , Samba Siva Rao Pasupuleti 2 , Ashini Kumar Hidam 3 , Anupam Kumar 3 , Harsh Vardhan Tevethia 1 , Rajan Vijayaraghavan 1 , Arpita Majumdar 1 , Adarsh Prasher 3 , Sherin Thomas 4 , Rajendra Prasad Mathur 5 , Guresh Kumar 6 , Shiv Kumar Sarin 1
|
Background & Aims
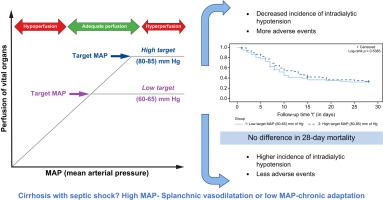
A high mean arterial pressure (MAP) target has been associated with improved renal outcomes in patients with cirrhosis, though it has not been studied in critically ill patients with cirrhosis and septic shock (CICs). We compared the efficacy of a high (80-85 mmHg; H-MAP) vs. low (60-65; L-MAP) target MAP strategy in improving 28-day mortality in CICs.
Methods
We performed open-label 1:1 randomisation of 150 CICs (H-MAP 75; L-MAP 75). The primary endpoint was 28-day mortality and secondary endpoints included reversal of shock, acute kidney injury (AKI) at day 5, the incidence of intradialytic hypotension (IDH), and adverse events. Endothelial markers were analysed in a subset of patients.
Results
The baseline characteristics were comparable. On intention-to-treat analysis, 28-day mortality (65% vs. 56%; p = 0.54), reversal of shock (47% vs. 53%; p = 0.41) and AKI development (45% vs. 31%;p = 0.06) were not different between the H-MAP and L-MAP groups, respectively. A lower incidence of IDH (12% vs. 48%; p <0.001) and higher adverse events necessitating protocol discontinuation (24% vs. 11%; p = 0.031) were noted in the H-MAP group. On per-protocol analysis (L-MAP 67; H-MAP 57), a significantly higher reversal of AKI (53% vs. 31%; p = 0.02) and a lower incidence of IDH (4% vs. 53%; p <0.001) were observed in the H-MAP group. Endothelial repair markers such as ADAMTS (2.11 ± 1.13 vs. 1.15 ± 0.48; p = 0.002) and angiopoietin-2 (74.08 ± 53.00 vs. 41.80 ± 15.95; p = 0.016) were higher in the H-MAP group.
Conclusions
A higher MAP strategy does not confer a survival benefit in CICs, but improves tolerance to dialysis, lactate clearance and renal recovery. Higher adverse events indicate the need for better tools to evaluate target microcirculation pressures in CICs.
Impact and implications
Maintaining an appropriate organ perfusion pressure during sepsis is the ultimate goal of haemodynamic management. A higher mean arterial pressure (MAP) improves renal outcomes in patients with hepatorenal syndrome. Patients with cirrhosis and septic shock have severe circulatory disturbances, low MAP, and poor tissue perfusion. In these patients, targeting higher MAP vs. lower MAP does not confer any survival benefit but is associated with more adverse events. A higher target strategy was associated with better tolerance and lesser episodes of hypotension on dialysis. Patients who could achieve the higher target MAP, without the development of adverse events, had improved renal outcomes and better lactate clearance. Higher MAP was also associated with improvements in markers of endothelial function. A higher target MAP strategy, with close monitoring of adverse events, may be recommended for patients with cirrhosis and septic shock.
Clinical trial number
NCT03145168.
中文翻译:
肝硬化和感染性休克患者的高目标平均动脉压与低目标平均动脉压的随机对照试验 (TARGET-C)
背景与目标
高平均动脉压(MAP)目标与肝硬化患者肾脏结局的改善相关,但尚未在患有肝硬化和感染性休克(CIC)的危重患者中进行研究。我们比较了高(80-85 mmHg;H-MAP)与低(60-65;L-MAP)目标 MAP 策略在改善 CIC 28 天死亡率方面的功效。
方法
我们对 150 个 CIC(H-MAP 75;L-MAP 75)进行开放标签 1:1 随机化。主要终点是 28 天死亡率,次要终点包括休克逆转、第 5 天急性肾损伤 (AKI)、透析中低血压 (IDH) 发生率和不良事件。对一部分患者的内皮标志物进行了分析。
结果
基线特征具有可比性。在意向治疗分析中,28 天死亡率(65% vs. 56%;p = 0.54)、休克逆转(47% vs. 53%;p = 0.41)和 AKI 发生(45% vs. 31%) ;p = 0.06)H-MAP 和 L-MAP 组之间分别没有差异。H-MAP 组中IDH 发生率较低(12% vs. 48%;p < 0.001),而需要终止方案的不良事件较高(24% vs. 11%;p = 0.031)。根据每个方案分析(L-MAP 67;H-MAP 57),AKI 逆转显着较高(53% vs. 31%;p = 0.02),IDH 发生率较低(4% vs. 53%;p = 0.02) < 0.001)在 H-MAP 组中观察到。 H-MAP 组的ADAMTS(2.11 ± 1.13对比1.15 ± 0.48;p = 0.002)和血管生成素-2(74.08 ± 53.00对比41.80 ± 15.95;p = 0.016)等内皮修复标志物较高。
结论
较高的 MAP 策略不会给 CIC 带来生存获益,但会提高对透析的耐受性、乳酸清除率和肾脏恢复。较高的不良事件表明需要更好的工具来评估 CIC 的目标微循环压力。
影响和影响
脓毒症期间维持适当的器官灌注压是血流动力学管理的最终目标。较高的平均动脉压 (MAP) 可改善肝肾综合征患者的肾脏结局。肝硬化和感染性休克患者存在严重的循环障碍、MAP低和组织灌注不良。在这些患者中,相对于较低的 MAP,以较高的 MAP 为目标不会带来任何生存获益,但会导致更多的不良事件。更高的目标策略与更好的耐受性和更少的透析时低血压发作相关。能够达到更高目标 MAP 且不会发生不良事件的患者,肾脏结局得到改善,乳酸清除率也更高。较高的 MAP 还与内皮功能标志物的改善相关。对于肝硬化和感染性休克患者,可能会建议采用更高目标的 MAP 策略,并密切监测不良事件。
临床试验编号
NCT03145168。
























 京公网安备 11010802027423号
京公网安备 11010802027423号