Surgical Endoscopy ( IF 3.1 ) Pub Date : 2022-09-19 , DOI: 10.1007/s00464-022-09613-z Takeshi Urade 1 , Masahiro Kido 1 , Kaori Kuramitsu 1 , Shohei Komatsu 1 , Hidetoshi Gon 1 , Kenji Fukushima 1 , Shinichi So 1 , Takuya Mizumoto 1 , Yoshihide Nanno 1 , Daisuke Tsugawa 1 , Tadahiro Goto 1 , Sadaki Asari 1 , Hiroaki Yanagimoto 1 , Hirochika Toyama 1 , Tetsuo Ajiki 1 , Takumi Fukumoto 1
|
Background
Anatomic liver resection (ALR) has been established to eliminate the tumor-bearing hepatic region with preservation of the remnant liver volume for liver malignancies. Recently, laparoscopic ALR has been widely applied; however, there are few reports on laparoscopic segmentectomy 2. This study aimed to present the standardization of laparoscopic segmentectomy 2 with surgical outcomes.
Methods
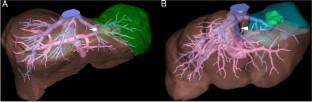
This study included seven patients who underwent pure laparoscopic segmentectomy 2 by the Glissonean approach from January 2020 to December 2021. Four of them had hepatocellular carcinoma, two had colorectal liver metastasis, and one had hepatic angiomyolipoma, which was preoperatively diagnosed with hepatocellular carcinoma. In all patients, preoperative three-dimensional (3D) simulation images from dynamic CT were reconstructed using a 3D workstation. The layer between the hepatic parenchyma and the Glissonean pedicle of segment 2 (G2) was dissected to encircle the root of G2. After clamping or ligation of the G2, 2.5 mg of indocyanine green was injected intravenously to identify the boundaries between segments 2 and 3 with a negative staining method under near-infrared light. Parenchymal transection was performed from the caudal side to the cranial side according to the demarcation on the liver surface, and the left hepatic vein was exposed on the cut surface if possible.
Results
The mean operative time for all patients was 281 min. The mean blood loss was 37 mL, and no transfusion was necessary. Estimated liver resection volumes significantly correlated with actual liver resection volumes (r = 0.61, P = 0.035). After the operation, one patient presented with asymptomatic deep venous and pulmonary thrombosis, which was treated with anticoagulant therapy. The mean length of hospital stay was 8.9 days.
Conclusion
Laparoscopic segmentectomy 2 by the Glissonean approach is a feasible and safe procedure with the preservation of the nontumor-bearing segment 3 for liver tumors in segment 2.
中文翻译:
Glissonean 入路腹腔镜第 2 段解剖性肝切除术的标准化
背景
解剖性肝切除术(ALR)已被建立来消除荷瘤肝脏区域,并保留剩余肝脏体积以治疗肝脏恶性肿瘤。近年来,腹腔镜ALR得到广泛应用;然而,关于腹腔镜肺段切除术 2 的报道很少。本研究旨在介绍腹腔镜肺段切除术 2 与手术结果的标准化。
方法
本研究纳入了 2020 年 1 月至 2021 年 12 月期间接受 Glissonean 入路单纯腹腔镜肺段切除术 2 的 7 例患者。其中 4 例患有肝细胞癌,2 例患有结直肠肝转移,1 例患有肝血管平滑肌脂肪瘤,且术前诊断为肝细胞癌。对于所有患者,术前使用 3D 工作站重建来自动态 CT 的三维 (3D) 模拟图像。解剖肝实质和第 2 段 (G2) 的 Glissonean 蒂之间的层,以包围 G2 的根部。夹闭或结扎G2后,静脉注射2.5mg吲哚菁绿,用近红外光下负染色法识别第2段和第3段之间的边界。按肝脏表面分界,从尾侧向头侧进行实质横断,尽可能在切面显露左肝静脉。
结果
所有患者的平均手术时间为 281 分钟。平均失血量为37毫升,无需输血。估计的肝切除体积与实际肝切除体积显着相关(r = 0.61,P = 0.035)。术后1例患者出现无症状深静脉血栓和肺血栓,接受抗凝治疗。平均住院时间为 8.9 天。
结论
采用 Glissonean 入路的腹腔镜肝段切除术 2 是一种可行且安全的手术,可保留第 2 段肝脏肿瘤的非肿瘤段 3。


























 京公网安备 11010802027423号
京公网安备 11010802027423号