Sports Medicine ( IF 9.8 ) Pub Date : 2022-09-17 , DOI: 10.1007/s40279-022-01751-7 Fabian Schwendinger 1 , Raphael Knaier 2, 3 , Thomas Radtke 4 , Arno Schmidt-Trucksäss 1
|
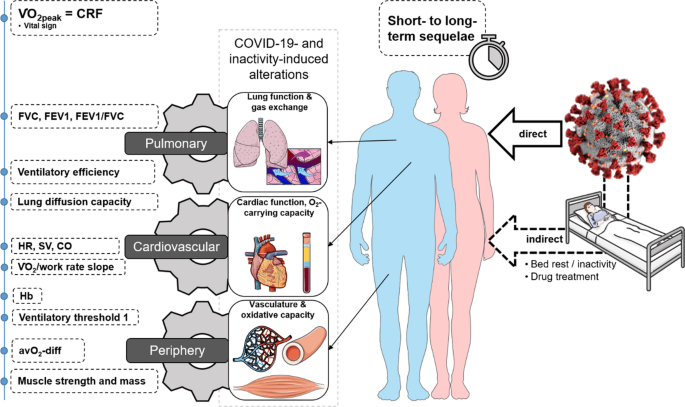
Patients recovering from COVID-19 often report symptoms of exhaustion, fatigue and dyspnoea and present with exercise intolerance persisting for months post-infection. Numerous studies investigated these sequelae and their possible underlying mechanisms using cardiopulmonary exercise testing. We aimed to provide an in-depth discussion as well as an overview of the contribution of selected organ systems to exercise intolerance based on the Wasserman gears. The gears represent the pulmonary system, cardiovascular system, and periphery/musculature and mitochondria. Thirty-two studies that examined adult patients post-COVID-19 via cardiopulmonary exercise testing were included. In 22 of 26 studies reporting cardiorespiratory fitness (herein defined as peak oxygen uptake—VO2peak), VO2peak was < 90% of predicted value in patients. VO2peak was notably below normal even in the long-term. Given the available evidence, the contribution of respiratory function to low VO2peak seems to be only minor except for lung diffusion capacity. The prevalence of low lung diffusion capacity was high in the included studies. The cardiovascular system might contribute to low VO2peak via subnormal cardiac output due to chronotropic incompetence and reduced stroke volume, especially in the first months post-infection. Chronotropic incompetence was similarly present in the moderate- and long-term follow-up. However, contrary findings exist. Peripheral factors such as muscle mass, strength and perfusion, mitochondrial function, or arteriovenous oxygen difference may also contribute to low VO2peak. More data are required, however. The findings of this review do not support deconditioning as the primary mechanism of low VO2peak post-COVID-19. Post-COVID-19 sequelae are multifaceted and require individual diagnosis and treatment.
中文翻译:
COVID-19 后心肺健康水平低下:叙述回顾
从 COVID-19 中恢复的患者通常会出现精疲力尽、疲劳和呼吸困难的症状,并且在感染后持续数月出现运动不耐症。许多研究利用心肺运动测试研究了这些后遗症及其可能的潜在机制。我们的目的是对基于 Wasserman 齿轮的选定器官系统对不耐受行为的贡献进行深入讨论和概述。齿轮代表肺系统、心血管系统、外周/肌肉系统和线粒体。其中包括 32 项通过心肺运动测试对 COVID-19 后成年患者进行检查的研究。在报告心肺健康(本文定义为峰值摄氧量 — V O 2peak)的 26 项研究中,有 22 项研究中,V O 2peak小于患者预测值的 90%。即使从长期来看,V O 2peak也明显低于正常水平。鉴于现有证据,除了肺扩散能力之外,呼吸功能对低V O 2peak的贡献似乎很小。在纳入的研究中,肺扩散能力低下的患病率很高。由于变时性功能不全和每搏输出量减少,心血管系统可能会通过低于正常的心输出量导致低V O 2peak,尤其是在感染后的头几个月。在中长期随访中也同样存在变时性功能不全。然而,存在相反的发现。肌肉质量、力量和灌注、线粒体功能或动静脉氧差等外围因素也可能导致低V O 2peak。然而,还需要更多数据。本综述的结果并不支持去适应作为COVID-19 后低V O 2peak的主要机制。COVID-19 后遗症是多方面的,需要个体化诊断和治疗。
























 京公网安备 11010802027423号
京公网安备 11010802027423号