Annals of Intensive Care ( IF 8.1 ) Pub Date : 2022-08-17 , DOI: 10.1186/s13613-022-01036-2 Sandrine Valade 1, 2 , Michael Darmon 1, 2 , Lara Zafrani 1, 2 , Eric Mariotte 1, 2 , Virginie Lemiale 1, 2 , Swann Bredin 1, 2 , Guillaume Dumas 1, 2 , Nicolas Boissel 2, 3 , Florence Rabian 2, 3 , André Baruchel 4 , Isabelle Madelaine 5 , Jérôme Larghero 6, 7 , Anne Brignier 8 , Etienne Lengliné 9 , Stéphanie Harel 2, 10 , Bertrand Arnulf 2, 10 , Roberta Di Blasi 2, 11 , Catherine Thieblemont 2, 11 , Elie Azoulay 1, 2
|
Background
CAR-T cell (chimeric antigen receptor T) therapy has emerged as an effective treatment of refractory hematological malignancies. Intensive care management is intrinsic to CAR-T cell therapy. We aim to describe and to assess outcomes in critically ill CAR-T cell recipients.
Study design and methods
Hospital-wide retrospective study. Consecutive CAR-T cell recipients requiring ICU admission from July 2017 and December 2020 were included.
Results
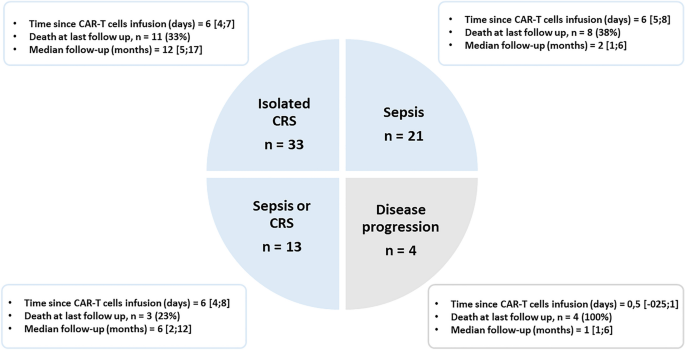
71 patients (median age 60 years [37–68]) were admitted to the ICU 6 days [4–7] after CAR-T cell infusion. Underlying malignancies included diffuse large B cell lymphoma (n = 53, 75%), acute lymphoblastic leukemia (17 patients, 24%) and multiple myeloma (n = 1, 1.45%). Performance status (PS) was 1 [1–2]. Shock was the main reason for ICU admission (n = 40, 48%). Isolated cytokine release syndrome (CRS) was the most common complication (n = 33, 46%), while 21 patients (30%) had microbiologically documented bacterial infection (chiefly catheter-related infection). Immune effector cell-associated neurotoxicity syndrome was reported in 26 (37%) patients. At ICU admission, vasopressors were required in 18 patients (25%) and invasive mechanical ventilation in two. Overall, 49 (69%) and 40 patients (56%) received tocilizumab or steroids, respectively.
Determinant of mortality were the reason for ICU admission (disease progression vs. sepsis or CRS (HR 4.02 [95%CI 1.10–14.65]), Performance status (HR 1.97/point [95%CI 1.14–3.41]) and SOFA score (HR 1.16/point [95%CI 1.01–1.33]).
Conclusions
Meaningful survival could be achieved in up to half the CAR-T cell recipients. The severity of organ dysfunction is a major determinant of death, especially in patients with altered performance status or disease progression.
中文翻译:
ICU 资源在 CAR-T 细胞受者中的使用:一项全院范围的研究
背景
CAR-T细胞(嵌合抗原受体T)疗法已成为难治性血液系统恶性肿瘤的有效治疗方法。重症监护管理是 CAR-T 细胞疗法所固有的。我们旨在描述和评估危重 CAR-T 细胞受体的结果。
研究设计和方法
医院范围的回顾性研究。包括从 2017 年 7 月和 2020 年 12 月起需要入住 ICU 的连续 CAR-T 细胞受体。
结果
71 名患者(中位年龄 60 岁 [37-68])在 CAR-T 细胞输注后 6 天 [4-7] 入住 ICU。潜在的恶性肿瘤包括弥漫性大 B 细胞淋巴瘤 ( n = 53, 75%)、急性淋巴细胞白血病 (17 例, 24%) 和多发性骨髓瘤 ( n = 1, 1.45%)。性能状态 (PS) 为 1 [1-2]。休克是入住 ICU 的主要原因(n = 40, 48%)。孤立性细胞因子释放综合征 (CRS) 是最常见的并发症 ( n = 33, 46%),而 21 名患者 (30%) 有微生物学记录的细菌感染(主要是导管相关感染)。在 26 名 (37%) 患者中报告了免疫效应细胞相关的神经毒性综合征。入住 ICU 时,18 名患者 (25%) 需要血管加压药,2 名患者需要有创机械通气。总体而言,分别有 49 名 (69%) 和 40 名 (56%) 患者接受了托珠单抗或类固醇治疗。
死亡率的决定因素是入住 ICU 的原因(疾病进展与败血症或 CRS(HR 4.02 [95%CI 1.10–14.65])、体能状态(HR 1.97/点 [95%CI 1.14–3.41])和 SOFA 评分( HR 1.16/点 [95%CI 1.01–1.33])。
结论
多达一半的 CAR-T 细胞受体可以实现有意义的生存。器官功能障碍的严重程度是死亡的主要决定因素,特别是在体能状态改变或疾病进展的患者中。

























 京公网安备 11010802027423号
京公网安备 11010802027423号