Leukemia ( IF 11.4 ) Pub Date : 2022-08-08 , DOI: 10.1038/s41375-022-01649-3 Philip A Thompson 1 , Xianli Jiang 2 , Pinaki Banerjee 3 , Rafet Basar 3 , Naveen Garg 4 , Ken Chen 2 , Mecit Kaplan 5 , Vandana Nandivada 5 , Ana Karen Nunez Cortes 5 , Alessandra Ferrajoli 1 , Michael J Keating 1 , Christine B Peterson 6 , Michael Andreeff 1 , Katayoun Rezvani 3 , William G Wierda 1
|
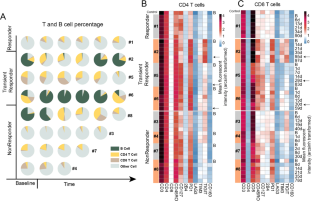
Richter’s Syndrome (RS) is an aggressive transformation of CLL, usually clonally-related diffuse large B-cell lymphoma (DLBCL), characterized by frequent TP53 mutations, intrinsic chemoresistance and poor survival. TP53-independent treatments are needed. We conducted a single center, phase 2, investigator-initiated study of high dose blinatumomab (maximum 112 mcg/d after initial, weekly dose escalation), NCT03121534, given for an 8-week induction and 4-week consolidation cycle. Responses were assessed by Lugano 2014 criteria. Serial multi-parameter flow cytometry from blood was performed to identify patient-specific biomarkers for response. Nine patients were treated. Patients had received a median of 4 and 2 prior therapies for CLL and RS, respectively. Five of 9 had del(17p) and 100% had complex karyotype. Four patients had reduction in nodal disease, including one durable complete response lasting >1 y. Treatment was well tolerated, with no grade >3 cytokine release syndrome and 1 case of grade 3, reversible neurotoxicity. Immunophenotyping demonstrated the majority of patients expressed multiple immune checkpoints, especially PD1, TIM3 and TIGIT. The patient who achieved CR had the lowest levels of immune checkpoint expression. Simultaneous targeting with immune checkpoint blockade, especially PD1 inhibition, which has already demonstrated single-agent efficacy in RS, could achieve synergistic killing and enhance outcomes.
中文翻译:
大剂量 blinatumomab 治疗里氏综合征的二期研究
里氏综合征 (RS) 是 CLL 的一种侵袭性转化,通常是与克隆相关的弥漫性大 B 细胞淋巴瘤 (DLBCL),其特征是频繁的 TP53 突变、内在的化疗耐药性和低生存率。需要 TP53 独立治疗。我们进行了一项单中心、2 期、研究者发起的高剂量 blinatumomab(初始、每周剂量递增后最大 112 微克/天)NCT03121534 研究,给予 8 周的诱导和 4 周的巩固周期。回复根据 Lugano 2014 标准进行评估。对血液进行连续多参数流式细胞术,以确定患者特异性生物标志物的反应。九名患者接受了治疗。患者先前接受的 CLL 和 RS 治疗的中位数分别为 4 次和 2 次。9 人中有 5 人有 del(17p),100% 有复杂核型。4 名患者的淋巴结疾病有所减少,包括一名持续 >1 年的持久完全反应。治疗耐受性良好,没有 3 级以上的细胞因子释放综合征和 1 例 3 级可逆性神经毒性。免疫分型表明大多数患者表达多个免疫检查点,尤其是 PD1、TIM3 和 TIGIT。达到 CR 的患者免疫检查点表达水平最低。同时靶向免疫检查点阻断,尤其是 PD1 抑制,已经在 RS 中证明了单药疗效,可以实现协同杀伤并提高疗效。免疫分型表明大多数患者表达多个免疫检查点,尤其是 PD1、TIM3 和 TIGIT。达到 CR 的患者免疫检查点表达水平最低。同时靶向免疫检查点阻断,尤其是 PD1 抑制,已经在 RS 中证明了单药疗效,可以实现协同杀伤并提高疗效。免疫分型表明大多数患者表达多个免疫检查点,尤其是 PD1、TIM3 和 TIGIT。达到 CR 的患者免疫检查点表达水平最低。同时靶向免疫检查点阻断,尤其是 PD1 抑制,已经在 RS 中证明了单药疗效,可以实现协同杀伤并提高疗效。

























 京公网安备 11010802027423号
京公网安备 11010802027423号