Journal of Clinical Monitoring and Computing ( IF 2.2 ) Pub Date : 2022-07-27 , DOI: 10.1007/s10877-022-00893-3 Jennifer Jouwena 1, 2, 3 , Sarah A Eerlings 1, 2, 3 , Andre M De Wolf 4 , Lieve Van Hoovels 5 , Arne Neyrinck 2, 3 , Marc Van de Velde 2, 3 , Jan F A Hendrickx 1, 2, 3, 6
|
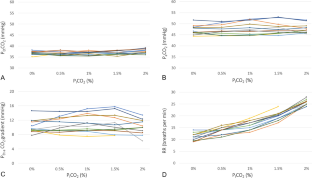
Isocapnic hyperventilation (ICHV) is occasionally used to maintain the end-expired CO2 partial pressure (PETCO2) when the inspired CO2 (PICO2) rises. Whether maintaining PETCO2 with ICHV during an increase of the PICO2 also maintains arterial PCO2 (PaCO2) remains poorly documented. 12 ASA PS I–II subjects undergoing a robot-assisted radical prostatectomy (RARP) (n = 11) or cystectomy (n = 1) under general endotracheal anesthesia with sevoflurane in O2/air (40% inspired O2) were enrolled. PICO2 was sequentially increased from 0 to 0.5, 1.0, 1.5 and 2% by adding CO2 to the inspiratory limb of the circle system, while increasing ventilation to a target PETCO2 of 4.7–4.9% by adjusting respiratory rate during controlled mechanical ventilation. Pa-ETCO2 gradients were determined after a 15 min equilibration period at each PICO2 level and compared using ANOVA. Mean (standard deviation) age, height, and weight were 66 (6) years, 171 (6) cm, and 75 (8) kg, respectively. Capnograms were normal and hemodynamic parameters remained stable. PETCO2 could be maintained within 4.7–4.9% in all subjects at all times except in 1 subject with 1.5% PICO2 and 5 subjects with 2.0% PICO2; data from the one subject in whom both 1.5 and 2.0% PICO2 resulted in PETCO2 > 5.1% were excluded from analysis. Pa-ETCO2 gradients did not change when PICO2 increased. The effect of a modest rise of PICO2 up to 1.5% on PETCO2 during RARP can be readily overcome by increasing ventilation without altering the Pa-ETCO2 gradients. At higher PICO2, airway pressures may become a limiting factor, which requires further study.
中文翻译:
等碳酸过度通气期间动脉到呼气末 CO2 梯度
当吸入的 CO 2 (P I CO 2 ) 升高时,偶尔会使用等碳酸过度通气 (ICHV) 来维持呼气末 CO 2分压 ( P ET CO 2 )。在 P I CO 2增加期间维持 P ET CO 2与 ICHV 是否也维持动脉 PCO 2 (P a CO 2 ) 仍然缺乏记录。12 名接受机器人辅助根治性前列腺切除术 (RARP) (n = 11) 或膀胱切除术 (n = 1) 的 ASA PS I–II 受试者在气管内全身麻醉下使用 O 2 /空气中的七氟醚(40%吸入O2)被录取。通过将 CO 2添加到循环系统的吸气肢,将P I CO 2从 0 依次增加到 0.5、1.0、1.5 和 2% ,同时通过调整呼吸频率将通气量增加到 4.7–4.9% 的目标 P ET CO 2在控制机械通气期间。在每个 P I CO 2水平的15 分钟平衡期后确定P a-ET CO 2梯度,并使用方差分析进行比较。平均(标准差)年龄、身高和体重分别为 66 (6) 岁、171 (6) cm 和 75 (8) kg。二氧化碳图正常,血流动力学参数保持稳定。聚乙二醇_除了 1 名 P I CO 2为 1.5% 的受试者和 5 名 P I CO 2为 2.0% 的受试者外,所有受试者的2可始终保持在 4.7–4.9% 以内;来自 1.5% 和 2.0% P I CO 2导致 P ET CO 2 > 5.1% 的受试者的数据被排除在分析之外。当 P I CO 2增加时, P a-ET CO 2梯度没有改变。P I CO 2适度上升至 1.5% 对 P ET CO 2的影响在不改变 P a-ET CO 2梯度的情况下,可以通过增加通风轻松克服 RARP 期间的问题。在较高的 P I CO 2下,气道压力可能成为一个限制因素,这需要进一步研究。

























 京公网安备 11010802027423号
京公网安备 11010802027423号